Demographic, Epidiomologic and Nutrition Transitions Faced by India and Its Implications on Oral Diseases and Dental Services
Info: 4447 words (18 pages) Dissertation
Published: 9th Dec 2019
Candidate number- z22917
STAGES OF DEMOGRAPHIC, EPIDIOMOLOGIC AND NUTRITION TRANSITIONS FACED BY MY COUNTRY AND ITS IMPLICATIONS ON ORAL DISEASES AND DENTAL SERVICES
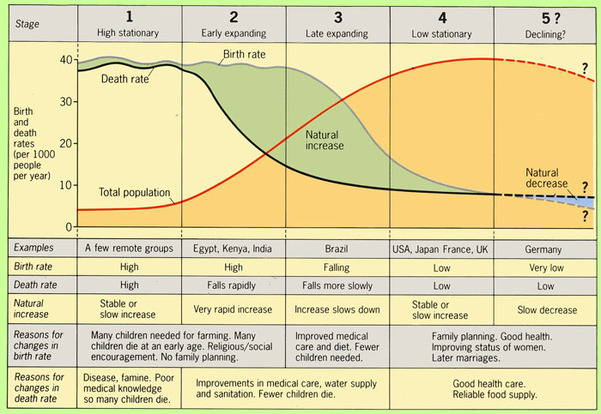
Transitions or changes are inevitable which takes place during a period. These are described as a process of change from one condition to another. The three important phases of transitions are Demographic, Epidemiologic and Nutrition. These periods have significantly made an impact in the country over the decade. The facts are evident on their implications in various diseases and services. However, its evidence on oral diseases and dental services are prime importance to us. Let us first understand the concept behind the three different transitional periods. Demographic transition is a model used to explain the process of high natality and high mortality rate to low natality and low mortality rate. This depends on developmental changes from pre-industrialized to an industrialized economy. This model was first introduced in 1929 by an American demographer named Warren Thompson. The various stages in this model are High Stationary, Early Expanding, Late Expanding, Low Stationary and Declining.
Each stage is explained based on growth and decline of population along with taking birth rates and death rates into consideration. Stage 1 is considered as an early stage of transition. Significant feature is the fluctuation seen both in birth and death rates. Moreover, there is no significant population growth observed. The countries considered in this stage have a basic standard of living. Further, there is lack of resources, education, hygiene, nutrition and absence of family planning which determines the background of this stage. Moving on to Stage 2 which is the period of high birth rate along with significant fall in death rates. The fall in death rate is mostly due to factors like better health care, improved sanitation, resource availability, leading to improved quality of life. This stage is considered as an era of modernisation. Stage 3 explains the fall in birth rates along with established trend of fall in death rates. Factors such as better family planning, access to education and effects of industrialisation have corresponded in fall against birth rates. Stage 4, which has stable population with birth rates and death rates in control. Coming to last stage which is Stage 5, explains negative growth. Adding to it, fewer birth rate than death rate is observed. The factors mainly associated with the changes are independent trend of women and financial constraints of general population.
Now, let us look at the demographic transition faced by my country. Every country undergoes demographic transition, based on the model at different periods. In fact, majority of the developed nations are in the stage 2 and 3.(ANTHAMATTEN, 2011) Likewise, India has experienced its transitions at different time intervals. Based on Thompson model in 1929 , transition of India is quite evident in the model, with drastic fall in death rate and high birth rates rate.(ANTHAMATTEN, 2011) (Fig1)
Later period, there was evidence of birth rate getting declined significantly This was mostly seen due to quality education, rapid urbanization and better health with rise in economy. (Chaudhry, Jan., 1983),).The country approached towards the third stage in the later period. Further, the birth rate equalled the death rate during the period of 1971-81.Adding to this, crude birth rate declined by 8 percent from 1971-81 .(Gowariker, 1994, India, 2011a) In fact, birth rates have declined by about 31% from 1991-2016 with additional decline of 2 % percent from 2011-16 (India, 2011a). Another aspect to look upon is the life expectancy. Life expectancy during the period of 1950-2000 was about 26.2 years.(Choudhry and Elhorst, 2010).However, life expectancy have improved gradually from 24 years to 64 years in the present conditions.(Shradha Mathur* 1, 2015) In the coming years the tables have turned and transition is quite significant.(INDIA, 2011c).The graph below describes the comparison between different rates. It is evident from the figure that birth rate and death rates have declined significantly. Further, infant mortality rates have declined while total fertility rates have started to decline lately.(INDIA, 2011c). In fact, TFR have declined from 3.6 to 2.3 in the period of 91-2016.(India, 2011a) Factors like education and 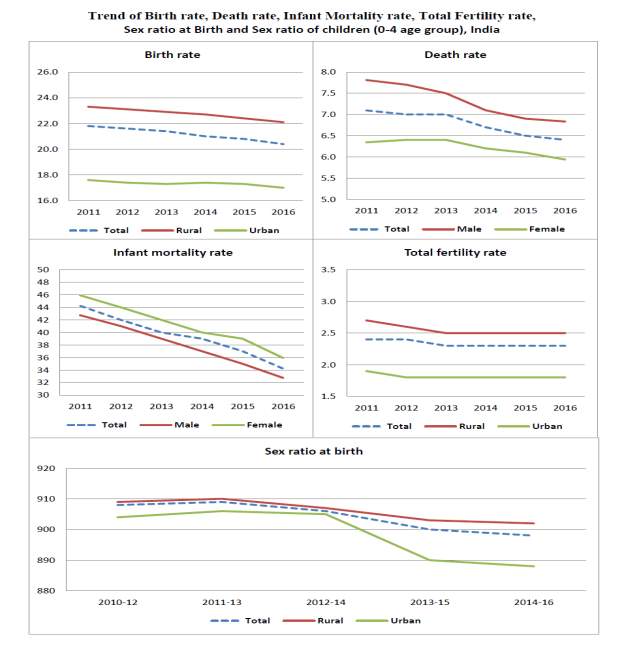
awareness, family planning and industrialisation have been influential over the population. As for sex ratio, it has been quite stable till 2014, but started to decline later. With the ongoing transition, studies have questioned it as beneficial or distress trend.(Kumar, 2014)
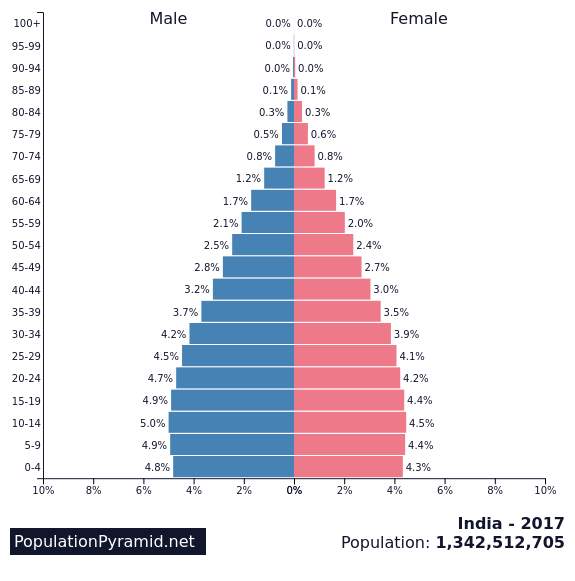
From the corresponding graph, we can see the fall in death rates. In fact, death rates have decline from 7.0 to 6.4 during the period of 2011-16(India, 2011b). Moreover, decline has been quite abrupt in rural areas compared to urban. Infant mortality rates have declined from 44 in 2011 to 36 in 2016.(India, 2011b).Total fertility rates have declined from 2.5 to 2.3 in 2016.(India, 2011b, Division, 2017). These changes gives a clear picture of ongoing modernisation taking place. India at an era of modernisation and globalisation are facing the transitory changes rapidly. Finally the population of country is estimated to be 1.3 billion people, along with the fluctuations with the rates.
The next transitional change which is quite an appealing one is called The Nutritional Transition. This transitional model was introduced by Adam Drewnowski and Barry M. Popkin based on analysis. The key events discussed in the nutritional transition are role of income on diet structure, impact of urbanisation and availability of oils and fats.(Adam Drewnowski, February 1997:) . It is observed that, prosperity and indigence has an effect on diet and nutrition. Moreover, economy has always been a major determinant in defining eating habits of individuals. For instance, diet popular with complex carbohydrates and fibre are given less importance than diets rich in fats and sugars due to effect of urbanization.(Adam Drewnowski, February 1997:). Therefore, these shifts in diet structure have led to demographic transitions with increased life expectancy and decreased fertility rate among population. Along with it, there is epidemiological shift with change from infectious and nutrient based diseases to cardiovascular and cancer diseases. Further, higher prevalence cases of childhood obesity and non-insulin dependent diabetes is evident worldwide. Consumption of junk foods, sugars and animals fats are held responsible for chronic obese cases. Moreover, there is a similarity observed in population with high income, tend to consume diet rich in fats and sugar. Let us look at the nutritional transition faced by my country. The trend has been changing since decades in the country. The country is facing scenarios related to diet causing non communicable diseases.(Misra et al., 2011) About 35% of the population consuming vegetarian diet has transformed rapidly into consumption of meat products since 2000.(Bishwajit, 2015). There is a transformative change seen in the country against replacing traditional diets with high fatty diet.(S K Kapoor, 2002).Additionally, increased demands for fish, meats and dietary products consumption are seen as an association with rise in income. Over past 30 years (1973-2004), population has lowered the deprived energy from carbohydrates by 7% and, increased energy intake from fats by 6%.(Misra et al., 2011). Per capita GDP is one of the additional factors, leading to change in diet trend. Urbanisation is an important factor associated with nutrition transition. Urbanisation has led to increased obesity cases, diabetes cases and coronary heart diseases. In fact, 60% of the total population lives in rural areas, but the effect of urbanisation is rapid.(India). Obesity cases are mostly seen in urban areas compared to rural areas. Also, rapid urbanization has reduced physical activities, with more people working towards service sector compared to agriculture.(Bishwajit, 2015). Change in working patterns such as less work shifts, longer vacations, use of vehicles are some of the factors contributing towards less physical activities. These factors have generated more obesity cases in the decade. Undernourishment is another concern in the country. In fact, country accounts about 25% undernourished people in compared to world population. Prevalence of undernourished cases are extremely high in the country.(Siddiqui et al., 2017).Further, lack of care, health and nutrition, poor nutrition status of mothers, low birth weight, poor hygiene, lack of resources due to low socioeconomic status have increased the prevalence of such cases.(Archer, 2007). Few studies have been implemented to understand the nutritional variation in the country. The studies have observed the increased intakes of fat calories among the income groups in the rural areas, while the population with poor household, living in the urbans are mostly noted with intake of fat calories.(Siddiqui et al., 2017). Moreover, higher income groups in the country consumes 32% of energy from fat while about 17% of energy is derived from fat by the lower income groups.(Shetty, 2002). Intake of fats in diet are seen as part of nutritional transitions .Transition in nutrition is also observed with per capita supply of animal products, which has increased from previous years. It has been observed that some of food items such as cereals, pulses contains invisible fats which is consumed by large proportion of population. Further, these invisible fats constitute about 15% of energy intake from the diets.(Shetty, 2002).The nutritional transition has affected largely and made a huge impact over the population. Urbanization, change in diet trends, role of physical activities, consumption of fats are some of contributing factors, accounted on basis of socioeconomic differences.(M Vaz1, 2005) These factors have imposed a threat for non-communicable diseases in the country.
Coming to last transition named: The Epidemiological Transition is given by Abdel R Omran. This model basically explains the distribution of disease and death.(Omran, (Oct., 1971),) These determinants are studied to determine the change in population. Moreover, this form of transition also helps to identify the theory behind the growth of population. This theory was established to give a more comprehensive view towards dynamics of population. Moreover, this model explains the transition in disease pattern, from infectious to non-communicable diseases. Another feature of this model is impact of demographic, economic and sociologic patterns on health and disease patterns. Most significant part of this model is its explanation about distinctive patterns of epidemiological transition. Further, to elaborate more, this model has been explained based on respected countries. The Classical or Western model represented England, The Accelerated model represented Japan and The Contemporary or Delayed model represented Chile and Ceylon.(Omran, (Oct., 1971),) There are propositions made based on mortality and populations dynamics. The first preposition denotes mortality as a fundamental factor in population dynamics. However, role of mortality in population dynamics is not directly expressed in theories of population cycle. Moreover, these cyclic movements determines growth and decline phases of population, ignoring influence of migration and variation of fertility and mortality. Second preposition discussed is about shift in pattern of diseases and mortality. Further, evidence of degenerative and manmade diseases were held factors for morbidity and death. Third preposition introduced is regarding influence of age and sex associated with risk in mortality. It gives detail account of pandemic recession and factors associated with improving pandemic recession by improved living, nutrition and sanitation measures. High evidence of recession is mostly observed in children and women, due to their high susceptibility from infection and deficiency diseases. Fourth preposition talks about association of demographic and socioeconomic factors that determines transition in disease patterns. Let’s discuss about the epidemiological transition state of my country. Both demographic and epidemiological transitions are taking place at parallel level. Based on Omran model on epidemiology, country is facing transition through second and third preposition. Age of Receding pandemic and Age of Man Made Diseases are the current transitions taking place.(Yadav and Arokiasamy, 2014). Country is facing the consequences of non-communicable diseases with the ongoing burden of communicable diseases. Current scenario is that of low mortality, high morbidity and dual diseases imposed on the country. This is mostly due to increased prevalence of chronic disease cases hampering the change in structure of disease patterns.(Quigley, 2006) In fact, old age mortality is higher in compared to children and adult. Increased life expectancy of old age people is declining due to chronic diseases affecting and lack of comprehensive health interventions by the government.(Yadav and Arokiasamy, 2014). Diseases like ischemic heart diseases, COPD and stroke are most prevalent and life taking diseases in the country.(WHO, 2011). Apart from this, other ongoing burdens estimated are diseases associated with maternal, neonatal, nutritional, diabetes and cardiovascular diseases.(WHO, 2011). It is observed that tuberculosis cases increased by 28% from 1998 to 2008. The causes associated are continuous change in BMI, diabetes, effects of urbanisation and ageing.(Dye et al., 2011). A study has estimated that death caused by NCD increased in between 1990 and 2016. It was significant for ischemic heart disease, diabetes and chronic kidney diseases.(Dandona et al., 2017).Moreover, it is observed that NCD are associated with obesity and lifestyle.(Alter and Sharma, 2016). Diabetes has always been a challenge to resolve. The cases of diabetes have increased significantly and almost doubled the findings in the current scenario.(Papers, 2005) To conclude, country is experiencing change in patterns of diseases and many factors are associated with this change such as lifestyle, socioeconomic state, nutrition, resources, behaviour with knowledge and awareness.
The three transitions have various implications on oral disease and dental services. The clear association between oral disease and NCD are presented worldwide, with tooth loss associated with premature mortality. The prevalence of oral disease is quite high with dental caries, periodontal disease and oral cancer are the most common phenomena. Starting with the most common oral disease, called the oral cancer. There has been lots of studies generated to link up the etiological factors, associated with the transitions. It is most popular disease in the country, associated with cultural, ethnic and geographical factors related to it. These factors correspond towards the development of habits and behaviour of individuals.(Byakodi et al., 2012) The habits of tobacco chewing, tobacco smoking has close association with the confounding factors like socioeconomic background, which is dependent on demographic trend.(Hernández et al., 2015) In fact, prevalence of oral cancer cases are quite high with the ongoing transitions. Incidence rate of oral cancer is estimated to be 12.6 per 100000 population in the year 2003 compared to China with 4.6(WHO, 2011). Ageing is one of the issue addressed which is associated with oral health diseases. The mark of 65 plus population is quite high, since life expectancy rates have gone high and fertility rates have gone low.(OFFICE OF THE REGISTRAR GENERAL et al., 2016). Further, studies have observed that edentulous cases were more prevalent than periodontal and root caries cases.(Sujatha et al., 2017, Moynihan and Petersen, 2007). Such cases explains the demographic transitional effects on oral health. Role of nutritional variation plays an important role in oral diseases. The studies has revealed that diet rich in vitamins C&D , antioxidants and diet rich in fibre decreases periodontal inflammations.(Woelber et al., 2016). This data explains the impact of healthy diet on oral health status. Healing with oral surgery requires appropriate diet for recovery. In fact poor nutrition hampers the healing activity.(Giridhar, 2016).The ongoing trend of replacing diets with fats and sugars has an effect over oral diseases. Caries prevalence cases are seen mostly among population consuming diet rich in sugar, carbohydrates. Epidemiological transition has dominantly affected on oral diseases and dental services. The ongoing trend of NCD has an effect on prevalence of dental diseases. Factors like diabetes and hypertension effect the oral health and increases the severity of diseases. Systemic diseases are closely related to oral health cases. Country is facing the burden of NCD which increases the incidence and prevalence cases of oral health. The dental services of the country faces challenge to cope up with the transitory effects. Workforce is not equally divided for urban and rural populations. Lack of resources, planning are some of the factors that hinders the quality of dental services.
Finally, in conclusion, the demographic transition of the country has entered the modernisation trend. The birth rates and death rates have declined significantly from the past years. The life expectancy rates have gone high with fertility rates going down. The country expects to have a better stability with all the rates. The nutritional transition has varied significantly from past years. Ongoing effects of urbanisation along with population consuming diet rich in fats and sugar has transformed immensely. Moreover obesity cases are quite high which should be addressed with improved lifestyle, support physical activities and change in diet pattern. Undernourishment is another issue raising the infant mortality cases. Lack of awareness and knowledge, poor sanitation and lifestyle issues are topics to be addressed efficiently by the governing body. The epidemiological transition is quite evident with transform of disease pattern, from infectious diseases to NCD. Diseases like heart diseases, diabetes, kidney diseases and oral diseases are extremely prevalent in the country. The oral conditions are affected by the systemic diseases. The dental services of the country is facing new challenges from the different effects of transitions taking place, coping up with the oral diseases. The dearth in workforce ratio in compared to rural and urban places should be resolved. Transitory effects have impacted the demographic status of the population, nutritional trend and finally the disease patterns and distribution.
REFERENCEs
ADAM DREWNOWSKI, P. D., AND BARRY M. POPKIN, PH.D. February 1997:. The Nutrition Transition: New Trends in the Global Diet. Nutrition Reviews, Vol. 55,, 31-43.
ALTER, J. S. & SHARMA, C. 2016. Nature cure treatment in the context of India’s epidemiological transition. Journal of Integrative Medicine, 14, 245-254.
ANTHAMATTEN, P. H., H. 2011. Demographic change and emerging and resurgent infectious diseases. An Introduction to Health Geography.
ARCHER, S. L. 2007. Staying focused on the undernourished child – India. J Am Diet Assoc, 107, 1879-81.
BISHWAJIT, G. 2015. Nutrition transition in South Asia: the emergence of non-communicable chronic diseases. F1000Res, 4, 8.
BYAKODI, R., BYAKODI, S., HIREMATH, S., BYAKODI, J., ADAKI, S., MARATHE, K. & MAHIND, P. 2012. Oral cancer in India: an epidemiologic and clinical review. J Community Health, 37, 316-9.
CHAUDHRY, M. D. Jan., 1983),. The Demographic Transition in India. University of Chicago Journal Press, Vol. 31.
CHOUDHRY, M. T. & ELHORST, J. P. 2010. Demographic transition and economic growth in China, India and Pakistan. Economic Systems, 34, 218-236.
DANDONA, L., DANDONA, R., KUMAR, G. A., SHUKLA, D. K., PAUL, V. K., BALAKRISHNAN, K., PRABHAKARAN, D., TANDON, N., SALVI, S., DASH, A. P., NANDAKUMAR, A., PATEL, V., AGARWAL, S. K., GUPTA, P. C., DHALIWAL, R. S., MATHUR, P., LAXMAIAH, A., DHILLON, P. K., DEY, S., MATHUR, M. R., AFSHIN, A., FITZMAURICE, C., GAKIDOU, E., GETHING, P., HAY, S. I., KASSEBAUM, N. J., KYU, H., LIM, S. S., NAGHAVI, M., ROTH, G. A., STANAWAY, J. D., WHITEFORD, H., CHADHA, V. K., KHAPARDE, S. D., RAO, R., RADE, K., DEWAN, P., FURTADO, M., DUTTA, E., VARGHESE, C. M., MEHROTRA, R., JAMBULINGAM, P., KAUR, T., SHARMA, M., SINGH, S., ARORA, R., RASAILY, R., ANJANA, R. M., MOHAN, V., AGRAWAL, A., CHOPRA, A., MATHEW, A. J., BHARDWAJ, D., MURALEEDHARAN, P., MUTREJA, P., BIENHOFF, K., GLENN, S., ABDULKADER, R. S., AGGARWAL, A. N., AGGARWAL, R., ALBERT, S., AMBEKAR, A., ARORA, M., BACHANI, D., BAVDEKAR, A., BEIG, G., BHANSALI, A., BHARGAVA, A., BHATIA, E., CAMARA, B., CHRISTOPHER, D. J., DAS, S. K., DAVE, P. V., DEY, S., GHOSHAL, A. G., GOPALAKRISHNAN, N., GULERIA, R., GUPTA, R., GUPTA, S. S., GUPTA, T., GUPTE, M. D., GURURAJ, G., HARIKRISHNAN, S., IYER, V., JAIN, S. K., JEEMON, P., JOSHUA, V., KANT, R., KAR, A., KATAKI, A. C., KATOCH, K., KHANNA, T., KHERA, A., KINRA, S., KOUL, P. A., KRISHNAN, A., KUMAR, A., KUMAR, R. K., KUMAR, R., KURPAD, A., et al. 2017. Nations within a nation: variations in epidemiological transition across the states of India, 1990–2016 in the Global Burden of Disease Study. The Lancet, 390, 2437-2460.
DIVISION, U. N. D. O. E. A. S. A. P. 2017. World Population 2017.
DYE, C., BOURDIN TRUNZ, B., LONNROTH, K., ROGLIC, G. & WILLIAMS, B. G. 2011. Nutrition, diabetes and tuberculosis in the epidemiological transition. PLoS One, 6, e21161.
GIRIDHAR, V. U. 2016. Role of nutrition in oral and maxillofacial surgery patients. Natl J Maxillofac Surg, 7, 3-9.
GOWARIKER, V. 1994. Demographic Transition in India. Economic and Political Weekly, Vol. 29,, 3106-3108.
HERNÁNDEZ, J. D. L. F., GARCÍA, S. S., DÍAZ, F. D. C. A., PONCE, E. H. & VILCHIS, M. D. C. V. 2015. Does the Demographic Transition Impact Health? The Oral Epidemiological Profile of the Elder Population.
INDIA, C. O. <Rural_Urban_2011.pdf>.
INDIA, G. O. 2011a. ESTIMATES OF FERTILITY INDICATORS. In: INDIA, C. O. (ed.).
INDIA, G. O. 2011b. ESTIMATES OF MORTALITY INDICATORS. Census of India.
INDIA, G. O. 2011c. Trend of Birth rate, Death rate, Infant Mortality rate, Total Fertility rate,
Sex ratio at Birth and Sex ratio of children (0-4 age group), India. In: INDIA, C. O. (ed.).
KUMAR, U. 2014. India’s Demographic Transition: Boon or Bane? Asia & the Pacific Policy Studies, 1, 186-203.
M VAZ1, S. Y., A V BHARATHI1, A V KURPAD1, S SWAMINATHAN1 2005. The nutrition transition in India. SAJCN, Vol. 18.
MISRA, A., SINGHAL, N., SIVAKUMAR, B., BHAGAT, N., JAISWAL, A. & KHURANA, L. 2011. Nutrition transition in India: secular trends in dietary intake and their relationship to diet-related non-communicable diseases. J Diabetes, 3, 278-92.
MOYNIHAN, P. & PETERSEN, P. E. 2007. Diet, nutrition and the prevention of dental diseases. Public Health Nutrition, 7.
OFFICE OF THE REGISTRAR GENERAL, I., AFFAIRS, M. O. H. & DIVISION, V. S. 2016. VITAL STATISTICS OF INDIA
OMRAN, A. R. (Oct., 1971),. The Epidemiologic Transition: A Theory of the Epidemiology of Population Change. The Milbank Memorial Fund Quarterly, Vol. 49,, 509-538.
PAPERS, G. O. I. N. B. 2005. Burden of Disease in India. In: HEALTH, N. C. O. M. A. & MINISTRY OF HEALTH & FAMILY WELFARE, G. O. I., NEW DELHI (eds.).
QUIGLEY, M. A. 2006. Commentary: shifting burden of disease–epidemiological transition in India. Int J Epidemiol, 35, 1530-1.
S K KAPOOR, K. A. 2002. Nutritional transition: a public health
challenge in developing countries. J Epidemiol Community Health, 56, 804–805.
SHETTY, P. S. 2002. Nutrition transition in India. Public Health Nutr, 5, 175-82.
SHRADHA MATHUR* 1, N. M. 2015. Demographic transition and population ageing in India: Implications on the
elderly of the future
Shradha Mathur*. GLOBAL JOURNAL OF MEDICINE AND PUBLIC HEALTH, Vol. 4.
SIDDIQUI, M. Z., DONATO, R. & JUMRANI, J. 2017. Looking Past the Indian Calorie Debate: What is Happening to Nutrition Transition in India. The Journal of Development Studies, 1-20.
SUJATHA, B., GOMEZ, M., MATHEW, N. & SURESH, J. 2017. Oral health problems among geriatric population and its implication on general health: A cross-sectional survey. Journal of Dental Research and Review, 4, 13-16.
WHO 2011. India:WHOstatisticalprofile. Countrystatisticsandglobalhealthestimates
byWHOandUNpartners.
WOELBER, J. P., BREMER, K., VACH, K., KONIG, D., HELLWIG, E., RATKA-KRUGER, P., AL-AHMAD, A. & TENNERT, C. 2016. An oral health optimized diet can reduce gingival and periodontal inflammation in humans – a randomized controlled pilot study. BMC Oral Health, 17, 28.
YADAV, S. & AROKIASAMY, P. 2014. Understanding epidemiological transition in India. Glob Health Action, 7, 23248.
Cite This Work
To export a reference to this article please select a referencing stye below:
Related Services
View all


Related Content
All TagsContent relating to: "Dentistry"
Dentistry is a branch of medicine that involves treating and preventing issues relating to your teeth, gums, and jaw. Dentistry not only ensures that you have a healthy mouth, but it can also have a positive impact on your general health and well-being.
Related Articles

DMCA / Removal Request
If you are the original writer of this dissertation and no longer wish to have your work published on the UKDiss.com website then please: