Positive Behaviour Support (PBS) Effectiveness
Info: 11198 words (45 pages) Dissertation
Published: 10th Dec 2019
Tagged: ManagementPsychology
Contents page
- Introduction
- Background of PBS
- Review of the literature
- Localised findings
- Action plan
- Summary/conclusion
- References
- Appendices
For this assignment, I have followed the Code (NMC, 2015) guidelines which states that all nurses should ensure they respect people’s rights when it comes to their privacy and confidentiality. Therefore, throughout my work I have ensured the anonymity of any organisation or person I may have referred to.
How beneficial is a PBS approach to people who present with behaviours that challenge?
Introduction
I currently work as a nursing assistant within an assessment and treatment unit for adults with learning disabilities within a health board in Scotland which covers a wide geographical area. The unit consists of four houses as we call them and all in there are sixteen beds available for admissions. As we are an assessment and treatment unit, there tends to be a variation in the needs of the patients that are admitted to the unit. Some people may be admitted due to their dietary intake being poor which has caused notable weight loss, others perhaps due to non-concordance to their medication and then there can be the severe issues such as behaviours that challenge being so extreme there has been a breakdown in community placement settings. Their needs will vary depending on the reason for admission and how severe their disability is. Some of the patients will also suffer from mental health problems alongside their learning disability which in turn can lead to them having more complex needs. The patients coming to us can have anything from a very mild to a very severe learning disability or even multiple disabilities. Therefore, when a patient is first admitted the staff are then required to decide, once they have all the relevant information about the person and reason for admission, as to which house is going to be the most suitable for that individual’s needs. When making this decision staff must consider the needs of the people and the vulnerability of those who are already in the houses. Unfortunately, we are often seeing patients being admitted who are presenting with behaviours that challenge and this can in turn mean that more vulnerable patients are living alongside the people displaying disruptive or violent behaviours, which can compromise their safety. This, unfortunately cannot always be prevented but when situations as such occur staff need to be extra vigilant and safeguard others as much as they possibly can.
We are getting more and more admissions who are presenting with behaviours that challenge, some being so severe that the person has required to be cared for in a house themselves as they have been such a threat to others. I have witnessed, been victim to and heard reports regarding incidents where either patients or staff members have sustained injuries, some severe, due to the severity of the behaviours. Therefore, I realised quickly that this was a topic I wanted to focus on and ways in which these situations could be managed more efficiently to reduce such behaviours and incidents occurring. NICE (2015), state that the Learning disabilities: challenging behaviour quality standard, expects staff to participate in facilitating towards improving areas such as; patient safety, safeguarding, control over daily life, quality of life, premature mortality, experience of care and physical and mental health wellbeing. For this reason, I am enthusiastic not only about ways in which these behaviours might be overcome but also to ensure a better quality of life for the patients displaying these behaviours, their families and others close to them. When I found out I was to base my project on an intervention, I arranged a meeting to discuss this with my manager and other members of staff within the unit it. I had informed them that I had an interest in ways behaviours that challenge could be managed more effectively. After discussion, it was proposed I should get involved in the implementation of Positive Behaviour Support (PBS), which is an intervention my workplace was currently rolling out to the unit. Two of the staff nurses along with the clinical psychologist, had been given the roles of training the staff on the PBS approach and implementing the model for the people who required such plans to be put in place. I would work alongside them and put input into the creation and implementation of the plans. At that point, a lot of the staff had already completed the PBS training and there were only a couple of small groups still to undertake the training. Being involved in the PBS model gave me the opportunity to research the topic to help answer my question on whether the PBS approach is beneficial. I would also be given the chance to see first-hand if, by utilizing the model with someone displaying the behaviours, whether this was an intervention that looked to be beneficial in making a difference to the lives of these people.
The RCP (2007) define behaviours that challenge as being a behaviour which is of such intensity, duration or frequency it can threaten an individual’s quality of life and/or their physical safety or that of others, which in turn can lead to responses which are restrictive, aversive or result in the individual being excluded. Over the year’s various studies have been carried out which indicate people with learning disabilities are at a higher risk of presenting with behaviours that challenge than the average population. These studies have shown challenging behaviour has a varying prevalence of between 5% to 15% in large population studies (Holden & Gitlesen. 2006). Rojahn et al. (2001) state that behaviours that challenge can include;
- Self-harm – when a person causes harm to themselves by repeatedly hitting, biting or scratching themselves, pulling their own hair, headbutting.
- Aggression – being deliberately violent towards another by grabbing, pulling, kicking, biting or hitting them.
- Destructiveness – deliberately damaging their surroundings or possessions, either their own or others.
- Stereotypies – repetitive movements of the body or postures such as rocking, spinning around, twisting and inappropriate smelling of objects.
According to Poppes et al. (2010), behaviours that challenge can be found more frequently in people who have profound intellectual and multiple disabilities (PIMD) and such behaviours as self-harm and stereotypies were on a daily occurrence, and in most cases this can be witnessed on an hourly basis. Social withdrawal is another behaviour which is known to be a frequent occurrence in people with PIMD, due to lack of communication skills and behaviours that challenge. Vlaskamp et al. (1997) state that people who present with social withdrawal behaviour will show no signs of attempting to make contact with others or their environment. When a person discards any attempts to make contact with their environment, it will have an impact on their ability to gain life experiences and on their development. Due to the nature of these behaviours more problems can arise for the patient, their family and those close to them and can further lead to social inclusion. People who are presenting with more severe behaviour will typically show more than one form of behaviour and the occurrence of the behaviour is often associated with the extent of their learning disabilities (Rojahn 2004). Therefore, the more severe the individuals learning disability is, the more likely there will be multiple forms of behaviours that challenge being displayed.
Bearing all of this in mind I was enthusiastic and eager for the success of the model, as this would hopefully assist in changing the lives of the people displaying behaviours that challenge. It would furthermore ensure a more relaxed working environment for the staff, as they would not be on edge, never knowing when the next incident will occur. It would also ensure the people who live alongside them would be staying in a more pleasant and peaceful environment.
Background of PBS
Positive behaviour support first came to light in the 1980’s and since then has become an established but still to this day a much under-utilised, intervention model for people who have learning disabilities and are presenting with behaviours that challenge (Shephard, 2012). (Dunlap, 2006) states that PBS originated from applied behaviour analysis (ABA) and maintains it is still closely aligned with it. PBS also has elements of other behaviour models within it, such as active support and social role valorisation. ABA used to and still is utilized and did show benefits, however, one of the components was using punishment as a way of managing behaviours and showing people there would be consequences for their actions. PBS is adamant that under no circumstances should punishment be used in the management of behaviours and the use of reactive strategies, such as control and restraint techniques are only ever to be used when a situation is so extreme that it is required to safeguard the person and others.
PBS is an intervention which uses multiple components and is designed to support people with learning disabilities and behaviours that challenge. It is a set of research-based strategies used to increase a person’s quality of life and at the same time decrease behaviours that challenge by teaching new skills and making appropriate changes within their environment (Wehmeyer, 2015). According to (Lavigna & Willis, 2005), achieving better opportunities for people with learning disabilities is a key objective of the community care movement, so as they can interact and integrate within their normal communities. However, those patients who display behaviours that challenge are left facing major barriers. To add to the unacceptability of these behaviours, the usual support strategies being utilised are also providing barriers for inclusion because of their social unacceptability. PBS is a model which has been created which will support the people affected by challenging behaviour to address those concerns and provide an effective socially valid intervention approach. PBS is an intervention which aims to help people who are displaying behaviours that challenge and rather than merely focussing on the internal drivers of the behaviour it also focusses on the environmental influences. So, staff are required to develop an understanding of the influences within the person’s environment and how they could be affecting someone’s behaviour. Once there is an understanding of this, interventions can then be designed and implemented which are specific to that person’s needs.
(LaVigna & Wills, 1992) state that the PBS model puts emphasis on four key categories for its intervention:
- Making changes to the environment before there is an occurrence of the problem behaviours by implementing strategies such as stimulation based intervention, greater choices, and changes to setting events.
- By utilizing self-management and functional communication training, appropriate behaviours can then be taught.
- By reinforcing the appropriate behaviours more so than the challenging ones.
- Reacting to behaviour so that safety and dignity are improved, while also reducing unintentional reinforcement of the behaviour.
Over the years as PBS has developed, various authors have elaborated its description and started to formulate a growing number of vital, descriptive elements. (Carr et al., 2002) were aware that not all the features of PBS were unique to its model and that many practitioners utilizing other approaches may well subscribe to similar guidelines. However, they realised that the features still define PBS and outlined nine features they felt did this. The features are as follows:
1. An improved quality of life and comprehensive change in lifestyle as being the fundamental and essential goals of the intervention;
2. To recognise that the supports and interventions implemented need to be seen from a longstanding, lifetime perspective.
3. The approaches of the interventions and support need to be appropriate to, and effective in, real life settings and circumstances. So, there needs to be a focus on ecological validity.
4. It should be insisted that Primary stakeholders (such as parents, friends, employers and siblings) take part and contribute information during the development process and implementation of the PBS model.
5. There should be an emphasis on how socially valid the procedures and outcomes are.
6. There should be an understanding that efficient, long lasting support will require changes in systems and multiple interventions.
7. It is important there is an emphasis on prevention and to recognise that functional (proactive) interventions will occur when the problem behaviours are not present
8. There will be an awareness and utilization of the knowledge that has been developed from a variety of procedural practices, and, respectively;
9. A realistic appreciation for the contributions of numerous theoretic perspectives.
Review of the literature
Research is a necessity in the successful promotion and protection of health and well-being, as well as to the latest, effective health and social services (DH, 2005). Carrying out this review will provide the evidence required for me to answer whether the PBS model is a beneficial intervention for patients who are presenting with behaviours that challenge. (Open University, 2017a) states that the literature review I create should give the main points of the papers and whether they can support my arguments or whether there is evidence within them which will go against the aspects of my project. It also states that it should show how the papers relate to the project so I can therefore create a critical analysis of same.
When I first started to research for my project it was crucial I kept records of the journals, articles, books and so on, as this would make things far more accessible to me when I got to this stage of the project. As the (Open University, 2017b) stated it is important when carrying out research to keep accurate records of all references and citations I have found this to be beneficial for the project as I ensured that I familiarised myself with endnote, as I had never used it in the past. Once I was familiar with it, developing an appropriate storage and filing system for my references was my next step. This system was easy to use and I would say it was user-friendly, which simplified things for me when accessing material for the project. It also assisted with my time management as I was not left searching through materials to find the articles I had previously accessed.
Researchers of PBS have been using a varied range of research methods so as they can explore influences, develop assessments and interventions that are useful, and assess how effective and reliable specific and wide-ranging the behaviour support strategies are. Even when using different methods, it is still evident that a PBS approach is beneficial to the person the plan has been created for.
During my research, it became apparent that the PBS approach to behaviours that challenge was indeed beneficial. One of the first studies I researched (McClean et al, 2012), had carried out a study on sixty-one members of staff who had completed training in PBS. This was person-focused training and included 5 longitudinal courses on multi-element behavioural support. Each member of staff had to carry out a functional assessment on an individual before creating and implementing a plan for them, this is a necessity of the PBS approach. The measures of the behaviours that challenge was taken after 6-months and then again after a 26-month period. The results of the study showed a clear reduction in behaviours that challenge. One of the figures shown for the study showed data from real-time behaviour observation and this showed a reduction of 61% at 3 months and then 83% at 6 months. (Mcclean et al, 2005) had carried out an earlier study which was like the previous one I discussed. In this study, there was a sample group of 138 people with learning disabilities ranging from severe to mild, of different ages and genders. Again, staff that had been trained in PBS created plans for each person and the outcome of this study again showed significant reduction in behaviours that challenge. The behaviours had reduced in 77% of the cases at 22.5 months after implementation. The fact that many of the people who part of the study were presenting with severe behaviours and self-harm, indicates that the PBS approach is a beneficial model in most cases that behaviours that challenge are being displayed.
One of the studies I researched was on an individual, rather than group of people as this individual was presenting with high level behaviours that challenge. I was keen to see if there was further evidence to support my findings as to whether the model would be successful enough to have an impact on such severe behaviours. The study carried out by (MacDonald et al, 2010) was also predominantly the same approach as I had taken with Mr B in my workplace. For the study, they carried out a functional assessment before formulating a visual formulation that outlined the issues causing the man’s behaviour and created strategies to put in place when they saw signs of the behaviours starting. To measure their findings, they used an 8-point severity scale, which showed aggression and destruction averaging at 6 and self-injurious behaviour averaging at 4.5. After implementation of the plan had been established there was a notable decrease of almost half for both the self-injurious behaviours and the aggressive and destructive behaviours. With the decrease in the behaviours, came an increase in activity participation. Further evidence that this model is beneficial in reducing behaviours and giving people a better quality of life.
(McClean et al, 2007) carried out a study on 5 people who displayed the most severe behaviours that challenge in the country (Ireland) and this was established by rating them from the subscale of the Harris Challenging Behaviour checklist. Each one of them rated a 5 on the scale which meant they had caused significant injury to themselves or others. There were no other individuals beside these 5 that scored as high on the scale. All five of the participants had significant communication problems and could only carry out one or two step requests. The results for this study amazed me as all five participants had reduced levels of behaviours to near-zero levels after the implementation of their PBS plans. There was a significant reduction in medication for 3 of the participants and four of the participants showed reduction in their depression, anxiety and hypomania scales. I think the fact the behaviours were so severe and their communication skills were so poor, led me to be optimistic surrounding the outcomes but once again the PBS approach was a success.
(LaVigna et al, 2012) carried out a study which method was to review the outcomes of a range of studies. Studies that involved punishment as consequences were excluded. The PBS model does not use punishment as a consequence for someone’s behaviours. Only studies which had investigated a variety of outcomes, due to a fully developed plan. These outcomes needed to include positive programming, proactive strategies and non-reactive strategies. Five questions were set to find out if a PBS approach could prove effective in these concerns. The questions were;
- Is PBS effective in severe behaviours? (from the studies on severe behaviour it does show reductions in these behaviours)
- Is it effective with high rate behaviours? (there is evidence of reduction again in high rate behaviours)
- Do staff need to be highly trained specialists (no was the result of this question, as it would not be possible to give the support to people needing it due to lower levels of highly trained specialists being available)
- Is PBS more expensive than previous services? (PBS approach appears to be cost effective)
- Can the model work in institutional settings? (yes, as it was proved efficient in the studies that had been carried out in institutions within the study)
(Allen et al, 2005) published an article which addressed the evidence of PBS’s effectiveness. In the article, they claim that a PBS approach appears to be the intervention of choice for those with learning disabilities and challenging needs, due to the fact it is ethically stringent and it is an evidence based approach. Therefore, an evidence based approach to the delivery of services then suggests that PBS interventions would be the approach most commonly implemented within this group of people. Unfortunately, this is not the case, as it is thought it is only a percentage of between 2 and 20% who require such interventions, are receiving some form of behavioural support. Instead of using this intervention, many services are still using psychotropic medication and restraint techniques. Surely this then poses the question, if PBS is proving to be as successful, then why is it not being made available to everybody that requires it?
The overall findings of the research I carried out appear to show PBS is a strong behaviour intervention that works well when implemented correctly. It is a model that needs to be consistent and requires to be maintained over time as opposed to short term implementation. When moving from institutional services, back to the community the plan must be kept in place, so as there is less opportunity for there to be any breakdown in the behaviours. It is also apparent that this approach needs to have widespread delivery as, even though it has been around since the 1980’s it is still very much an underutilized model for behaviours that challenge. The evidence further shows that the use of the model can contribute towards a better quality of life, as when there is a reduction in the behaviours then the person is more likely to be able to engage more in activities and not be as socially isolated as they may have been when the behaviours were present. Often, the potential for the behaviours that challenge to resurface is still there but good management and implementation serves to keep the behaviours to a minimum. I did not come across any studies during my research that maintained a PBS approach was not effective in some form. Therefore, my findings support my project question, which was ‘How beneficial is a PBS approach to patients who present with behaviours that challenge?’. A PBS approach seems to be a very beneficial intervention when working with someone displaying behaviours that challenge.
Localised findings.
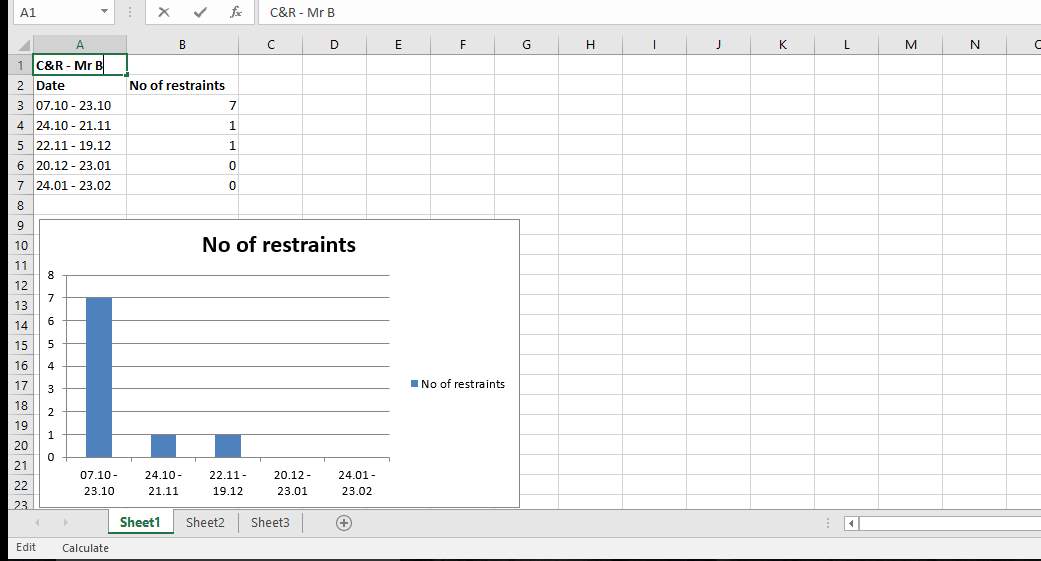
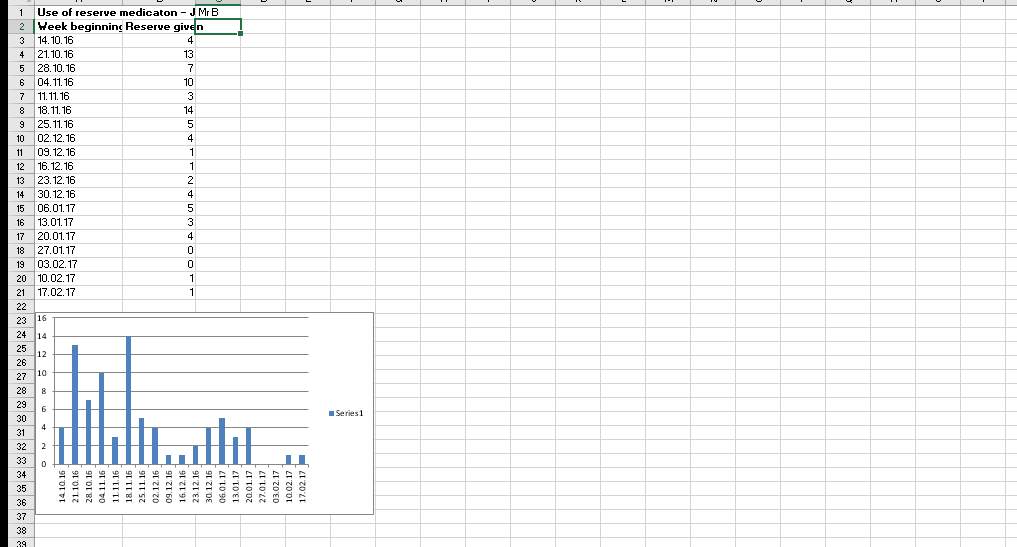
The PBS plan that was put in place for Mr B during the project shows there has been a significant reduction in his behaviours that challenge. The records that were produced throughout the process which give details of the occurrence of behaviours and the interventions used are evidence of this. The reactive strategies, which are always last resort measures that are used when the person reaches a point where the safety of themselves or others is compromised, saw the utilization of control and restraint techniques being reduced, with it being used 7 times during the first 2 weeks of his admission, which could also have had a lot to do with the change in environment and new staff members as this can often be a distressing process for people. The intervention then decreased to once a month for 2 months and since then there have been no incidents which have reached such a crisis point that it was required. There also saw a reduction in the amount of times reserve medication was administered. This has decreased from being as much as 14 times in one week to being as little as none being required some weeks. I will stress, when the medication was being administered as frequently, Mr B was also experiencing problems with his bowels which was soon picked up on and the correct treatment is now being given. Mr B has now built relationships with staff members and I feel this has a reduction in his attempts to assault members of staff anymore and the destructive behaviour is few and far between now. Due to the reduction in Mr B’s behaviours, staff are now able to engage him in activities and outings more often, which he gets much enjoyment from. Mr B loves to go out for long walks and this is now possible and can happen more frequently. He has also started to participate in group activities within the unit and is attending sessions within the occupational therapy department. The management of the behaviours and use of strategies are clearly working effectively now that the plan is well established. So much so that it is felt Mr B is now ready for discharge.
Action Plan
1 – Identify the idea/topic for my project.
This was the first stage of the project as I needed to identify what I would be basing my project on. After a meeting with my line manager and a couple of the nursing staff it was clear to myself that I wanted to do work which would improve the quality of life for those patients who were presenting with behaviours that challenge. My workplace was in the process of rolling out the PBS model and I was enthusiastic in having some input into the implementation and to research its effectiveness. There were two staff nurses who were carrying out the PBS training and implementation alongside the psychologist for the unit, whom I would be working alongside throughout the process. I was interested in trying to understand these behaviours from the patients point of view and the reasons behind them. There are various triggers that can cause the patient such distress that they communicate this by using such behaviours. Often patients with severe learning disabilities are unable to communicate, therefore they tend to use different ways of doing so which can include challenging behaviours. (Scope, 2016) report behaviours can be a way of communicating the need for food or drink. It can possibly be a sign the patient is in pain or discomfort, abuse, distress or anger and they can communicate this in varying ways such as withdrawing themselves or showing aggression. The environment could also be a factor for behaviours, for example; under or over stimulation, poor physical environment which can include extremes in noise levels or temperature and variations in staff as there is no consistency.
2 – Identify a patient
I wanted to work with a patient from the admission stage throughout the process so as I could see whether the model was successful and beneficial to the patient. At first this was not a possibility as we did not have any new admissions. However, a couple of weeks later a young man was admitted to the unit at crisis point which gave me the opportunity to work with him from the start of PBS implementation. The staff members involved in the PBS implementation were happy for me to work with Mr B and assist in his PBS plan being put in place.
Mr B is a 19-year-old man who has a diagnosis of autism spectrum disorder (ASD) and had been presenting with behaviours that challenge in his supported accommodation in the community but due to these behaviours his placement broke down. ADS’s are described by (Marco, E.J, et al. 2014) as a group of neurodevelopmental disorders of both social and communicative impairments, each one with varying severity and scope of expression. The main feature of ASDs is a profound impairment in a person’s ability to socialise and communicate. Mr B had been displaying both destructive and aggressive behaviours, so much so his home had become unliveable due to the extent of his destructive behaviours. Mr B’s communication skills are limited which makes it a challenge to understand what he is thinking and how we can best support him. Staff on the unit were aware that there would be initial issues with regards to the behaviours he displayed due to the change in his environment. Therefore, the first couple of weeks were difficult for Mr B and staff supporting him. Mr B continued with the destructive behaviour with multiple episodes of destruction of property particularly in the bathroom area causing extensive damage. He had also absconded on a couple of occasions when out with members of his family and targeted both members of staff and family members, by hitting out and scratching them.
3 – Assessment process
The next stage was to assess Mr B and attempt to identify triggers for the behaviours he was presenting with and ways in which staff could manage same. A functional assessment is one of the core assessments required to be completed when putting a PBS plan in place. These assessments are very detailed and are carried out by a clinical psychologist or a specialist on behaviour. The rationale for the assessment is that it increases understanding of what the causes are for the person’s behaviour and reduce the behaviours by making changes in the person’s life. The information collected from the functional assessment is used to create a plan that will aim to reduce the behaviour and the impact it can have on the person and people involved in their care. According to (The challenging behaviour foundation, 2017), the main aim is to have the strategies in place that will support the person learn more appropriate ways of meeting their needs, which are equally and more effective than the behaviours that are currently being displayed.
I was involved in completing and collecting the information from ABC charts that were also used in the assessment process. The ABC approach is another important model used to understand the behaviour and is known to be an effective technique which sets aside the emotions of behaviours that challenge and analysing them so that responses to them are effective. The model consists of three categories;
- Antecedents – These are the relevant events which occurred prior to the behaviour happening, which can be considered the triggers for the behaviour. The triggers can be anything from the emotional state of the person (tired, depressed etc.), things that others did or said before the behaviour and the environment (too noisy, hot, bright lighting, smells etc.).
- Behaviour – What is happening throughout the behaviour, what the person is doing (screaming, showing aggression, destructive behaviour). The behaviour may be to gain attention and at times this is best to be ignored as tactically ignoring is often linked with positive reinforcement.
- Consequences – How did the staff react immediately and after the behaviour? The consequences can be classed as both pleasant or unpleasant. A pleasant consequence will reinforce the behaviour as the person believes if they keep displaying the behaviour they get what they want. An unpleasant response will mean the person will be discouraged from the behaviour as they, for example realise they will be ignored if they display such behaviour. The best strategy seems to be positive reinforcement, when the person is given an incentive when the behaviour starts. For example; they will be praised if they use one of their distraction techniques instead of following through with the behaviour.
The charts needed to be completed consistently over a few weeks so as I could establish how often behaviours occurred, what the behaviours involved, if there were noticeable triggers for the behaviours and what strategies may be beneficial in distracting them from the behaviour.
I put aside some time to have discussions with other staff members as to what they had witnessed and their thoughts on what the triggers may be. This way I could ensure I was gathering as much information as possible so as the final PBS plan and its strategies have the biggest chance of succeeding. All staff are required to stick to the plan that is put in place and be consistent with it so as there is less chance of things breaking down.
Participation charts were put in place which would let us see exactly what Mr B was capable of partaking in. The charts have a list of activities of daily living such as washing, dressing, clearing tables, making bed and so forth. this would assist staff in realising what needs Mr B had so they could be of assistance if required. This should ensure Mr B did not become frustrated if there was something he could not manage on his own.
4 – Creating the PBS plan
Once all the evidence was gathered and triggers had been identified it was time to put the PBS plan together. A PBS plan is created using a person-centred approach so each plan is individual to a person’s needs and no two plans will be the same.
The following triggers for Mr B’s behaviour were identified;
- Increases in anxiety
- Bowel discomfort
- Overstimulation
- Transitions between activities
- Family leaving
- When unable to carry out a request (when requested to use toilet but does not need to go at that time).
- Being unable to have his requests met.
- Becoming bored with an activity
- Others being in his personal space
- Noise
- Not being involved in conversation/what’s happening
- Being left alone for too long
After identifying the triggers, strategies were created and put in place. So, to help Mr B cope with his increases in agitation such as;
- Helping Mr B cope with increases in agitation by getting him to do his controlled breathing techniques using bubbles which he was taught by staff.
- Structure to his day – activities (although staff need to be aware of length and over stimulation.
- Family visits
- Time alone – short spells alone to help him cope when he goes back to community setting
- Management of bowel issues – medication he is prescribed
- Continence and toileting issues – prompting but be aware not to prompt him too often as this can cause agitation if he does not need to go.
- Repetitive speech – staff manage this by telling Mr B “just once” indicating one with their finger.
- Fixation on breaking items – environment must be free from too many fixtures as much as possible, that may cause behaviour to occur. Have items fixed as quickly as possible when he has broken them.
Reactive strategies are utilized when Mr B is at crisis point and staff are expected to respond safely and effectively. Strategies at this stage include;
- Prevent harm to Mr B or others by using a clear and firm voice. Ask him to leave the room to an area with less triggers and continue to support throughout.
- As required medication can be offered as per protocol
- Physical intervention – staff can use prescribed C&R techniques as per NHS protocols based on management of violence and aggression techniques, using the least restrictive intervention based on clinical judgement of the incident at the time.
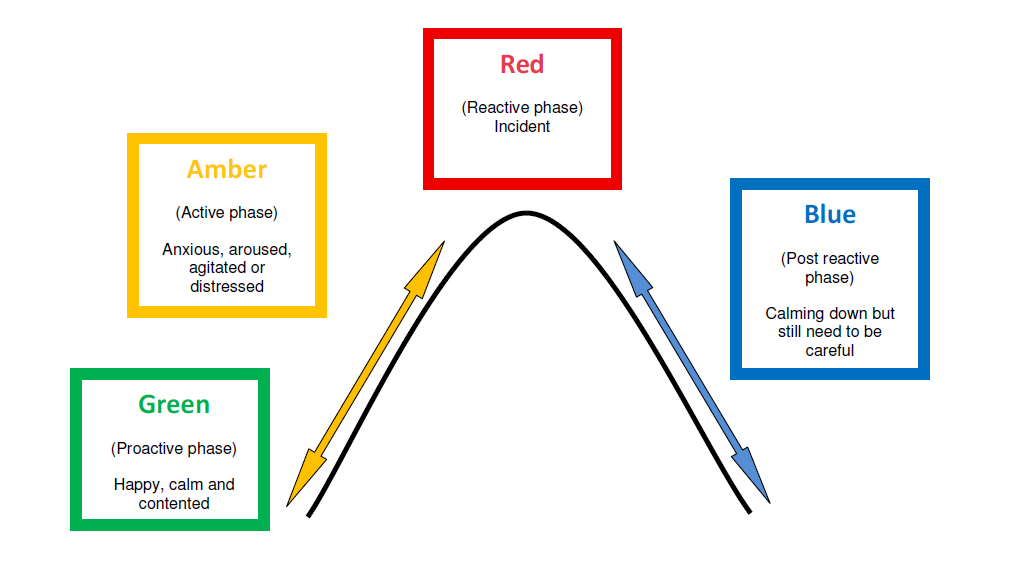
The plan has red amber and green indicators within it. These indicators express the different stages of behaviours. The green ‘proactive’ phase is when the person is calm, happy and content. Amber ‘active’ phase is when the person is becoming anxious, distressed or agitated. Then the red ‘reactive’ stage is crisis stage when staff need to react quickly for the safe and quick control of the situation this can at times lead to management of aggression techniques or reserve medication being administered. Blue ‘post reactive’ phase when the person has stopped the behaviour but still require to be precautious. Each phase in the plan will have indicators and strategies for staff to follow when Mr B’s behaviour is at each stage.
5 – Implementing the plan
The PBS plan being implemented was the next stage in the process and all staff were required to read it and sign a form attached to verify they had done so. Every member of staff needed to know the strategies that were going to be used and be aware when triggers were occurring. When the plan was first put in place it had a few minor issues due to some members of staff believing they could deal with the behaviour in their own way rather than sticking to the strategies within the plan. It was reiterated to these members of staff the importance of sticking to the plan and the benefits it could have for Mr B’s quality of life. As staff continued with the plan there was a notable reduction in the behaviours that challenge. Staff were recognising facial expressions and body movements that meant Mr B was becoming anxious, and were either providing him with coping mechanisms that had been identified or distract him from the behaviours before they escalated. Mr B is now at the stage where there was a notable reduction in the need for reserve medication and the use of violence and aggression restraining techniques. However, control and restraint is only ever utilized as a last resort when there is the risk of harm to a person or others as it is aimed to safeguard both staff and service users.
6 – Evaluation/review
Mr B’s plan is reviewed weekly and records are kept of incidents that have occurred, any management of aggression techniques that have been used and if reserve medication has been required at any point throughout the week. Any use of C&R techniques or reserve medication must be clearly documented and the incidents will be reviewed at MDT meeting for future learning points. Graphs are kept of these records so it is clearer to see reductions or fluctuations in behaviours that challenge incidences.
Summary & conclusion
As behaviours that challenge is being displayed so often in people with learning disabilities it is crucial an efficient intervention to reduce the behaviours is put in place. It is believed that once behaviours that challenge have been established, they tend to be persistent and ongoing (Kieman et al, 1996). It is important that the intervention is least restrictive to the person and ensure the person’s safety is always a priority. The PBS approach makes use of multicomponent intervention strategies that addresses the context of the behaviours, teaching of skills, different approaches to reinforcement and engagement in quality of life activities or practices. A PBS plan is always the outcome of a functional assessment of the person being carried out, and no plan will ever be produced without having gained this information prior to doing so. This is so the person is understood as much as possible and the correct interventions can be put in place to meet their needs.
From the research, I carried out during this project it is apparent that a PBS approach is a beneficial model for supporting those who present with behaviours that challenge. There have been many studies carried out to determine the benefits of the model and they are evidence in proving PBS model has had an impact on the reductions in behaviours that challenge. The results of studies have proven that the model can work for both mild and severe behavioural problems and both in the community and institutional settings. One of the studies included evidence, that 5 of the most severe cases of behaviours that challenge in Ireland, showed reduction in behaviours which I admit to being shocked about as I was clearly optimistic of the results being as such due to the extreme severity of the behaviours. Of course, the approach will not always eliminate all of the behaviours but reduction in them is always going to be better for the patient and those in close contact with them. By reducing the behaviours it will mean there will be less need to follow through with the reactive strategies, such as C&R techniques and reserve medication, which is surely better for the person and their health.
I feel that this intervention looks like it is going to have a positive impact on my workplace and practice, if the model works as well as the evidence states it does and as well as it has for Mr B. If it only works for a percentage of the patients who are presenting with these behaviours, this will still be a huge step towards improving the quality of life for others within the unit. It should also help to boost confidence and morale amongst the staff members, as at times this is low due to the challenges we are being met with daily and the injuries some members of staff have incurred. I am aware that some members of staff are a little set in their ways and do not tend to cope well with changes being made within the unit, therefore are not as cooperative with the PBS model and its implementation. This may or may not be a challenge that occurs in the future but it is also one that will be dealt with and hopefully through further explanation and evidence of the benefits it will be one which is easily overcome. Fortunately, this is only a small percentage of the staff and the majority are more willing to engage with the new approaches if it means they are going to see improvements within the workplace. It should benefit my practice as it is providing me with new skills which I can utilise and help towards giving the patients a better quality of life. As the RCN (2017) state all nurses and nursing staff should be providing a high standard of care for their patients with the best possible outcomes. Therefore, this is what I will be striving to do, so that any intervention that looks to be beneficial for my patients is going to be worth attempting if it means a better quality of care is delivered.
References
Allen, D. (2009). Positive behavioural support as a service system for people with challenging behaviour. Psychiatry, 8(10), pp.408-412.
Allen, D., James, W., Evans, J., Hawkins, S. and Jenkins, R. (2005). Positive Behavioural Support: Definition, Current Status and Future Directions. Tizard Learning Disability Review, 10(2), pp.4-11.
Carr, J. E., & Sidener, T. M. (2002). On the relation between applied behavior analysis and positive behavioral support. The Behavior Analyst, 25(2), 245–253.
Department of Health (2005) Research Governance Framework for Health and Social Care, London, Department of Health.
Dunlap, G. and Horner, R. (2006). The Applied Behavior Analytic Heritage of PBS: A Dynamic Model of Action-Oriented Research. Journal of Positive Behavior Interventions, 8(1), pp.58-60.
Emerson, E., Kiernan, C., Alborz, A., Reeves, D., Mason, H., Swarbrick, R., Mason, L. and Hatton, C. (2001). The prevalence of challenging behaviors: a total population study. Research in Developmental Disabilities, 22(1), pp.77-93.
Holden, B. and Gitlesen, J. (2006). A total population study of challenging behaviour in the county of Hedmark, Norway: Prevalence, and risk markers. Research in Developmental Disabilities, 27(4), pp.456-465.
Kieman, C. and Alborz, A. (1996). Persistence and Change in Challenging and Problem Behaviours of Young Adults with Intellectual Disability Living in the Family Home. Journal of Applied Research in Intellectual Disabilities, 9(3), pp.181-193.
LaVigna, G. and Willis, T. (2005). A Positive Behavioural Support Model for Breaking the Barriers to Social and Community Inclusion. Tizard Learning Disability Review, 10(2), pp.16-23.
LaVigna, G. and Willis, T. (1992) A model for multielement treatment planning and outcome measurement. In D. E. Berkell (Ed), Autism: Identification, education and treatment, pp. 135-149. Hillsdale, NJ: Erlbaum.
MacDonald, A., Hume, L. and McGill, P. (2010). The use of multi-element behaviour support planning with a man with severe learning disabilities and challenging behaviour. British Journal of Learning Disabilities, 38(4), pp.280-285.
Marco, E.J. Sherr, E.H. (2014) “Autism Spectrum Disorder”, Encyclopedia of the Neurological Sciences. Second edition, pp. 339-341.
McClean, B. and Grey, I. (2012). A component analysis of positive behaviour support plans. Journal of Intellectual and Developmental Disability, 37(3), pp.221-231.
McClean, B., Dench, C., Grey, I., Shanahan, S., Fitzsimons, E., Hendler, J. and Corrigan, M. (2005). Person Focused Training: a model for delivering positive behavioural supports to people with challenging behaviours. Journal of Intellectual Disability Research, 49(5), pp.340-352.
McClean, B., Grey, I. and McCracken, M. (2007). An evaluation of positive behavioural support for people with very severe challenging behaviours in community-based settings. Journal of Intellectual Disabilities, 11(3), pp.281-301.
NICE, (2015), Learning disabilities: Challenging behaviour, 28 October 2015 [Online], Available at: https://www.nice.org.uk/guidance/qs101/chapter/Introduction (Accessed 3rd April 2017).
Poppes, P., van der Putten, A. and Vlaskamp, C. (2010). Frequency and severity of challenging behaviour in people with profound intellectual and multiple disabilities. Research in Developmental Disabilities, 31(6), pp.1269-1275.
Rojahn J, Matson J, Lott D et al (2001) The behaviour Problems Inventory: An Instrument for the Assessment of Self-Injury, Stereotyped behaviour, and Aggression/Destruction in Individuals with Developmental Disabilities. Journal of Autism and Developmental Disorders. 31(6), pp. 577-588.
Rojahn, J., Matson, J., Naglieri, J. and Mayville, E. (2004). Relationships Between Psychiatric Conditions and Behavior Problems Among Adults With Mental Retardation. American Journal on Mental Retardation, 109(1), p.21.
Royal College of Psychiatrists, British Psychological Society, Royal College of Speech and Language Therapists (2007) Challenging Behaviour: A Unified Approach. Clinical and Service Guidelines for Supporting People with Learning Disabilities Who Are at Risk of Receiving Abusive or Restrictive Practices. Royal College of Psychiatrists, London.
Scope (2016) Reasons for Challenging Behaviour [Online] Available at http://www.scope.org.uk/Support/Parents/Behaviour/Reasons-for-challenging-behaviour (Accessed 20th October 2016).
Shephard, J. (2012). In celebration: living a life through Positive Behaviour Support. Tizard Learning Disability Review, 17(2), pp.69-75.
The Challenging Behavior Foundation (2017) Finding the Causes of Challenging Behavior: Part 2 [Online]. Available at http://www.challengingbehaviour.org.uk/understanding-behaviour/finding-the-causes.html (Accessed 1st May 2017).
The Open University (2017a) ‘Mini-Reviews’ KYN316 Block 2 Step2 : Writing your own mini-review, [Online] Available at https://learn2.open.ac.uk/mod/oucontent/view.php?id=910270§ion=2.2 (Accessed 12th April 2017)
The Open University (2017b) ‘2.3 Literature Reviews – preparation and practice KYN316 Block 2 Activity 3: Developing a system for recording information, [Online] Available at https://learn2.open.ac.uk/mod/oucontent/view.php?id=910266§ion=4.3 (Accessed 15th April 2017)
The Royal College of Nursing, 2017 ‘Principles of Nursing Practice’ [Online] Available at https://www.rcn.org.uk/professional-development/principles-of-nursing-practice (Accessed 8th April 2017).
Vlaskamp C., Zijlstra R. & Smets C. (1997) An exercise in balancing. In: Difficulties for Opportunities. Treatment of Behavioral Disorders in Children with Learning Disabilities(eds W. H. E. Buntinx & D. A. Flikweert. NGBZ, Utrecht.
Wehmeyer, M. (2015). The Oxford handbook of positive psychology and disability. 1st ed. New York, NY: Oxford University Press.
Appendices
Appendix 1 – Record of restraints.
Appendix 2 – record of reserve medication administered
Appendix 3 – ABC chart
BEHAVIOUR OBSERVATION CHART –
Name:
(If additional space is required – please use a separate sheet)
| DATE
|
TIME OF INCIDENT | LOCATION
|
| AT THE TIME THE INCIDENT OCCURRED DO YOU THINK BILLY WAS ….. | TIRED YES
NO |
IN PAIN YES
NO |
UNWELL YES
NO |
 OVERSTIMULATED YES OVERSTIMULATED YES
NO |
OTHER :
| TICK THE WORDS WHICH BEST DESCRIBE XXXX’S MOOD JUST PRIOR TO THE INCIDENT
CALM AGITATED HAPPY TENSE ANGRY TEARFUL EXCITED DISINTERESTED SAD ANXIOUS WITHDRAWN QUIET OTHER: |
|
| HOW LONG HAD XXXX BEEN LIKE THIS? | HAD THE MOOD BEEN GETTING MORE INTENSE PRIOR TO THE INCIDENT YES NO |
| DESCRIBE EXACTLY WHAT WAS HAPPENING BEFORE THE INCIDENT STARTED EG
|
| GIVE A FULL DESCRIPTION OF XXXX’S BEHAVIOUR DURING THE INCIDENT – EXACTLY WHAT DID XXXX DO/ SAY, WHICH ROOMS DID SHE GO INTO?
|
|
| DURATION OF INCIDENT
|
|
PLEASE REMEMBER TO COMPLETE THE OTHER SIDE ASWELL
| DESCRIBE EXACTLY HOW YOU/ OTHERS RESPONDED AT EACH POINT: -what did you say and do, where did you stand etc
|
| HOW DID XXXX RESPOND TO WHAT YOU DID/ SAID?
|
| LIST ANYTHING WITHIN THE LAST 24 HOURS WHICH MAY HAVE INFLUENCED XXXX’S MOOD, PHYSICAL STATE OR BEHAVIOUR (e.g. Being ill; routine changes; activity/visit cancelled, issue at school etc.) |
| OTHER COMMENTS: |
| CHART COMPLETED BY (name) : |
Appendix 4 – Participation Chart
PARTICIPATION RECORD
Name ………………………………………… Date ………………………………….
| SELF CARE | Mon | Tues | Wed | Thur | Fri | Sat | Sun | Total | |
| Had shower/bath | |||||||||
| Put on clean clothes | |||||||||
| Brushed teeth | |||||||||
| Washed face | |||||||||
| Combed hair | |||||||||
| Shaved | |||||||||
| Put on nightwear | |||||||||
| Total | |||||||||
| MEALS/ LAID TABLE | Mon | Tues | Wed | Thur | Fri | Sat | Sun | Total | |
| Prepared breakfast/
lunch/dinner/ |
|||||||||
| Prepared snack | |||||||||
| Made cup of tea/ coffee/juice | |||||||||
| Laid table | |||||||||
| Other (specify) | |||||||||
| Total | |||||||||
| CLEARING UP
After meals |
Mon | Tues | Wed | Thur | Fri | Sat | Sun | Total | ||
| Put dishes /cutlery away | ||||||||||
| Washed up/filled dishwasher | ||||||||||
| Dried up/ emptied dishwasher | ||||||||||
| Wiped dining table(s) | ||||||||||
| Other (specify) | ||||||||||
| TIDYING & CLEANING | Mon | Tues | Wed | Thur | Fri | Sat | Sun | Total | ||
| Daily dusting & tidying bedroom | ||||||||||
| Tidied kitchen | ||||||||||
| Changed bed | ||||||||||
| Other (specify) | ||||||||||
| Total | ||||||||||
| LAUNDRY | Mon | Tues | Wed | Thur | Fri | Sat | Sun | Total | |
| Put dirty clothes in laundry basket | |||||||||
| Used washing machine | |||||||||
| Hung out clothes | |||||||||
| Used tumble drier | |||||||||
| Put clothes away | |||||||||
| Other (specify) | |||||||||
| Total | |||||||||
| SHOPPING | Mon | Tues | Wed | Thur | Fri | Sat | Sun | Total | ||
| went to local shop | ||||||||||
| supermarket shop | ||||||||||
| Put shopping away | ||||||||||
| Other (specify) | ||||||||||
| Total | ||||||||||
| HOBBIES IN HOUSE | Mon | Tues | Wed | Thur | Fri | Sat | Sun | Total | |
| Watched TV | |||||||||
| Listened to music | |||||||||
| Read magazines / books | |||||||||
| group house activity (eg bingo) | |||||||||
| Individual activity (e.g arts/jigsaw) | |||||||||
| Other (specify) | |||||||||
| Total | |||||||||
| SOCIAL LIFE | Mon | Tues | Wed | Thur | Fri | Sat | Sun | Total | ||
| Had visitors | ||||||||||
| Visited other people | ||||||||||
| Went out with nursing staff | ||||||||||
| Went out with support team | ||||||||||
| Other (specify) | ||||||||||
| Total | ||||||||||
| HOBBIES IN THE COMMUNITY | Mon | Tues | Wed | Thur | Fri | Sat | Sun | Total | ||
| Took part in sports activity | ||||||||||
| Went to cinema/football match/restaurant | ||||||||||
| Attended Church, club or society | ||||||||||
| Went for a walk | ||||||||||
| Attended job | ||||||||||
| Other (specify) | ||||||||||
| Total | ||||||||||
Appendix 5 – Arousal curve of behaviour
Cite This Work
To export a reference to this article please select a referencing stye below:
Related Services
View all


Related Content
All TagsContent relating to: "Psychology"
Psychology is the study of human behaviour and the mind, taking into account external factors, experiences, social influences and other factors. Psychologists set out to understand the mind of humans, exploring how different factors can contribute to behaviour, thoughts, and feelings.
Related Articles

DMCA / Removal Request
If you are the original writer of this dissertation and no longer wish to have your work published on the UKDiss.com website then please: