Simulation in Undergraduate Medical Education
Info: 8044 words (32 pages) Dissertation
Published: 4th Feb 2022
Tagged: EducationHealth and Social Care
Abstract
In a climate of increasing attention to patient safety, medical graduates must be primed to manage clinical emergencies before they are required to initiate treatment whilst alone on call. Simulation is an apt teaching tool to provide undergraduates with opportunities for deliberate practice thus facilitating their development into prepared foundation doctors. This study sought to develop a simulation curriculum for medical students in Practical Emergency Care by combining quantitative and qualitative methods of enquiry. The authors reviewed medical school curricula and the literature, as well as surveying medical undergraduates and foundation doctors.
Findings include a discrepancy between the sparse advertisement of simulation in medical school curricula (only 8 of the 19 curricula available online describe simulation among their teaching methods) and the growing body of literature detailing clinical content, nontechnical skills, and execution of simulation scenarios. 6.53% of medical students and 5% of foundations doctors responded to surveys, chiefly with requests for more simulation. Both groups of respondents selected scenarios involving clinical and nontechnical skills, as well as trauma and unresponsive patients. However, the two groups disagreed as to whether subsequent scenarios should involve human factors, and common or rare scenarios. The study findings are used to determine what clinical scenarios and nontechnical skills should be incorporated into a working model curriculum as well as generating several recommendations for future enquiry.
Contents
Click to expand Contents
Introduction
Background
Aims and objectives
Methods
Results
Review of curricula
Themes in the literature
Surveys
Descriptive statistics: frequency tables for survey responses
Graphical comparison of medical student and foundation year doctor survey responses
Qualitative data: free text responses
Discussion
Curriculum consensus
Limitations
Next steps
Conclusion
References
Table of figures
Figure 1. Three stage literature search; search terms: ‘simulation AND emergency medicine AND undergraduate;’ exclusion criteria: ‘postgraduate, preclinical undergraduate, Dentistry, Veterinary, Nursing, computer-based simulation, simulation used solely to assess
Figure 2. Medical school curricula detailing use of simulation as a teaching and learning method
Figure 3. Thematic units from content analysis of the literature weighted according to frequency
Figure 4. Frequency of answers given by medical students and foundation doctors asked about learning domains to be incorporated in the simulation scenarios
Figure 5. Frequency of answers given by medical students and foundation doctors asked about clinical scenarios for inclusion in the simulation scenarios
Figure 6. Graphical comparison of survey answers on learning domains to be incorporated in the simulation scenarios
Figure 7. Graphic comparison of survey answers on clinical scenarios for inclusion in the simulation scenarios
Figure 8. Word cloud depicting themes from undergraduate free text feedback on ‘anything else that you think should be included in final year simulation training’ weighted according to frequency
Figure 9. Word cloud depicting free text feedback from foundation doctors on ‘a situation that you felt poorly prepared for as a junior doctor working in Emergency Medicine’ weighted according to frequency
Figure 10. Word cloud depicting free text feedback from foundation doctors on ‘a situation that your simulation prepared you well for’ weighted according to frequency
Figure 11. Word count depicting free text feedback from foundation doctors on ‘anything else that should be included in undergraduate simulation’ weighted according to frequency
Introduction
Background
There is mounting evidence that UK medical school curricula do not adequately prepare undergraduates for foundation training, (1) with medical students receiving minimal teaching in acute and traumatic aspects of care. (2) Despite calls for its mandate by the Quality Assurance Association for Higher Education (QAAfHE) (3) and the General Medical Council (GMC), (4) there is no standardised programme of preparation for managing acute medical emergencies, such that foundation doctors are confronted with emergencies that overstretch them. (1) Indeed, the QAAfHE Subject Benchmark Statement for Medicine states that ‘Graduates must be able to recognise and carry out the initial treatment of the following emergency situations, which require immediate action, such as: cardiac arrest; anaphylactic shock; the unconscious patient.’ (3)
The GMC and Department of Health have called on medical schools to employ new technologies among their educational arsenal and have students practice in a simulated environment before clinical reality. (5, 6) Simulation has repeatedly been proven as an effective teaching method and arguably there is no teaching tool better placed to reconcile the needs of medical students as adult learners with the demands of the modern healthcare environment where patient-safety concerns (7-17) and resource-restriction (9, 11, 15, 18, 19) are ubiquitous.
Simulation has been proven uniquely capable of satisfying multiple simultaneous teaching and learning needs. It can facilitate opportunities for reflective practice (7, 9, 10, 13-15, 20-26) and develop confidence (18, 25-30) as well as increase learners’ perceptions of their own readiness for clinical practice. (7, 9, 31) Simulation is an adept tool for developing team communication skills. (9, 16, 25, 32-34) Not only has the utility of simulation for ensuring clinical competency been proven, (8, 9, 14, 15, 18, 21, 25, 35, 36) but perhaps most importantly, as a cornerstone of modern adult learning theory,(37) learners themselves perceive simulation as useful and relevant.(7, 11, 18, 38-41)
Aims and objectives
The aim of this study was to contribute to improved relevance and efficacy of the undergraduate medical curriculum and thus better prepare final year medical students for independent clinical practice. The objectives to achieve this aim were to develop a simulation curriculum for medical students in Practical Emergency Care using a mixed methods approach and to synthesize four simulation sessions to be undertaken by medical students during their final year Emergency Medicine placements at the University of Manchester.
Methods
This quantitative and qualitative study comprised several elements including review of UK medical school curricula and programme specifications, literature review, and surveys of medical trainees at both undergraduate and postgraduate level.
Curricula and programme specifications for all 32 medical schools in the United Kingdom were accessed via the internet on 17th May 2017. Those publicly available were reviewed for reference to ‘simulation,’ and positive results were contacted via email with a request to provide further detail on how simulation is used to teach acute medical emergencies to their final year students.
A three-stage search of the literature was conducted comprising an initial broad search including grey literature, followed by a PubMed search on 19th May 2017 using the search criteria ‘simulation AND undergraduate AND emergency medicine,’ which generated 94 articles published since 2010. Exclusion criteria entailed articles focused primarily on postgraduate or preclinical undergraduate studies; students of Dentistry, Veterinary Science, and Nursing; simulation used as a tool primarily for assessment rather than teaching or simulation used to teach specialties other than Emergency Medicine; as well as virtual simulation. Identical searches were conducted in Medline, EMBase, and Cochrane and the same exclusion criteria applied.
The remaining papers were categorised as reviews, meta-analysis, or descriptive studies so that the bibliographies of the 14 reviews, meta-analyses, and best evidence guides therein could be reviewed according to the same criteria to improve catchment and reduce search bias. This generated a final body of 57 papers, which were analysed according to the following themes: what is simulation effective at teaching, what clinical scenarios and other skills should be included in the curriculum, and how should the scenarios be executed.
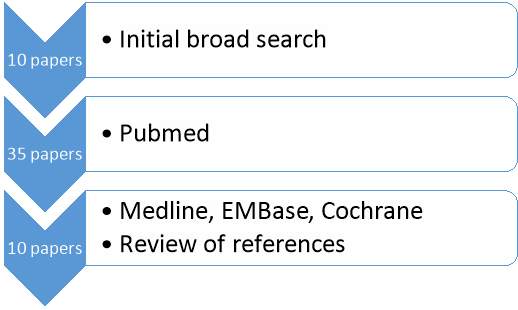
Figure 1. Three stage literature search; search terms: ‘simulation AND emergency medicine AND undergraduate;’ exclusion criteria: ‘postgraduate, preclinical undergraduate, Dentistry, Veterinary, Nursing, computer-based simulation, simulation used solely to assess
Surveys were constructed to pool opinions from medical students in their clinical years of study and foundation doctors anonymously. They were mapped to the University of Manchester curriculum and checked by a consultant for content validity. They were piloted before distribution to medical students at the University of Manchester via OneMedBuzz the official platform and related social media pages, whilst foundation doctors working across the North West received the survey via the Health Education England administrator. All medical students and foundation doctors were sampled to mitigate the anticipated low response rate. Quantitative and qualitative data were collected via Surveymonkey.
The data was analysed in SPSS to create tables of descriptive statistics for numerical summary, as well bar charts for visual comparison of medical student and foundation doctor opinions. The data also underwent chi-square testing to demonstrate independence. Free text answers were included to improve content validity and these underwent content analysis to elicit themes that could be used to contextualise and inform quantitative data.
All methods detailed above were collated to synthesize four practical sessions according to best practice.(42)
Results
Review of curricula
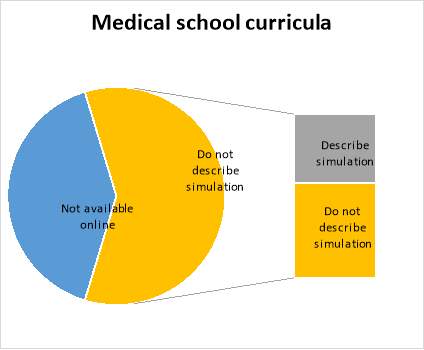
Figure 2. Medical school curricula detailing use of simulation as a teaching and learning method
Medical school curricula and programme specifications were reviewed to delineate the extent and methods by which simulation is currently employed as a teaching tool in the UK and to inform curriculum design. Of 34 medical schools in the UK, 2 were excluded as they do not offer clinical medicine. 19 curricula and/or programme specifications were available for open access via the internet. 13 were not available or had been temporarily removed pending review. Of the 19 accessed on 17th May 2017, 8 (42%) described using simulation as a formal component of the taught course and so a request for further detail was submitted via email. Of these eight, two responded with the below:
- Plymouth and Peninsula Medical Schools: ‘Every 5th year medical student undertakes a programme of eight sessions. Four are inter-professional in nature. Seven look at acute medical/surgical care and the eighth focuses on advanced communication skills around diagnosing brain stem death and conversations about organ donation. They are followed by a 30-minute debrief, which uses a model of non-technical and team-working skills as well as debriefing the clinical component of the scenario. We also use video debrief to show examples of both good and less-good practice. Their non-technical skills are currently evaluated using the ANTS (Anaesthetists’ Non-Technical Skills) framework. In particular, the IPL sessions are particularly highly valued as they seem to feel this better reflects the likely situation after they graduate as doctors.’
- University of Cambridge: ‘All final year students have a one-day simulation course that covers a number of medical emergencies. It is in a high-fidelity simulation suite and there are 5 students with a faculty of 4. We cover such emergencies as acute severe asthma, anaphylaxis, massive GI bleed, etc. We focus on non-technical skills (but obviously also cover the technical stuff)’
Themes in the literature
The literature was analysed to elicit key thematic units which could be correlated with the survey findings to inform curriculum design. The three broad themes entailed learning domains and clinical scenarios for inclusion, as well as how simulation sessions were best executed:
Clinical scenario Learning domain Execution
Figure 3. Thematic units from content analysis of the literature weighted according to frequency
Chest pain and cardiac arrest were the most commonly deployed clinical scenarios (9, 11, 19, 22, 25-27, 36, 41, 43-46), with respiratory,(9, 11, 18, 25, 27, 33, 43, 45, 46) and neurology,(22, 25, 43-47) and surgery(18, 25, 43-46) in tow. The vignettes for each category of clinical scenario were notably diverse, including an overdose of alcohol and prescribed medications presenting with decreased respiratory rate, as well as an agitated postictal head trauma victim presenting then experiencing a further seizure during the scenario.(47) Similarly, the outcomes of the scenarios were intentionally unpredictable,(13, 48) that is, both negative and positive irrespective of the students actions. It is worth noting that cardiac scenarios may be overrepresented as simulation is well established as a tool for teaching ACLS. Simulation was particularly useful for teaching non-technical skills such as team work(9, 13, 16, 19, 22, 23, 25, 33) and clinical reasoning(14, 20, 23, 25, 33, 35, 46) with attention also paid to preparedness for clinical practice in terms of professional communication skills(9, 13, 14, 18, 22, 23, 30, 33, 34, 44, 47) but also affective rehearsal.(9, 31)
There was great innovation and variety in the mode of execution of sessions including students being bleeped unexpectedly to simulation scenarios,(18) simulated night shifts,(35) inter-professional simulation,(22, 32, 33) simulation scenarios integrated within Emergency Medicine placements,(9, 19, 23, 25, 36, 44) and scenarios disrupted by challenging relatives or disgruntled senior staff thus furnishing opportunity to develop advanced communication skills in a controlled environment.(22) There was a discrepancy between simulation used as a discrete event(16, 25, 35, 45, 49) or running longitudinally throughout final year curriculum(9, 19, 20, 23, 25, 36, 44) with learning consolidated by feedback,(24, 25, 27, 42, 50, 51) clinical shifts(19) or subsequent reflection on a real clinical case.(23)
Several papers advocated the importance of simulation as a bridge to preparedness(27) rather than a tool for teaching new information, stressing the value of a flipped classroom to familiarise participants with theoretical material and the manikin itself.(9, 16, 18, 28, 36, 52, 53) There was a tension between whether the task ought to be complex to simulate the demands of the clinical environment or simpler in order to allow the learner to focus on mastering basic skills,(9, 10, 54) with some opting to introduce a programme of increasing complexity.(13, 48) It is encouraging in a climate of limited resources that simulation was repeatedly demonstrated to be an effective teaching tool regardless of group size:(19, 25, 26, 55) not only did observes benefit similarly to active participants but they can be engaged in assessment and feedback.(25)
Surveys
6.53% (96/1471) of clinical medical students and 5% (87/1734) of foundation doctors responded to the surveys. It should be noted that the total population of each group represents a slightly different figure: the total number of medical students in Years 3-5 including 3-4 and 4-5 intercalators is accurate, whereas the total number of foundation doctors will be slightly lower than the total number of foundation posts provided due to vacancies. At the time of writing, the survey of foundation doctors has been open for less time leading to fewer respondents.
The four answers selected with the greatest frequency will be detailed here in accordance with the objective of creating four simulation sessions. Medical students requested learning domains of clinical skills (89.89%), clinical factors (88.76%), human factors (57.3%), and advanced communication skills (40.45%) to be included amongst the simulation sessions. Whereas foundation doctors described feeling most prepared for clinical factors (83.53%), followed by advanced communication skills (76.47%), clinical skills (71.76%), and prescribing (68.24%); and least prepared for human factors (47.76%), clinical skills (41.79%), prescribing (40.30%), and advanced communication skills (29.85%). 71.76% foundation doctors felt prepared for clinical skills and 76.47% foundation doctors felt prepared for advanced communication skills.
One medical student provided a free text answer requesting sessions on: ‘clinical prioritisation and triaging leadership and innovation resource allocation major incident planning and resilience.’ Thirteen foundation doctors utilised the free text box to describe feeling prepared for ‘ALS’ and ‘basic skills only,’ but unprepared for ‘wound care and practical prescribing,’ ‘logistics and paperwork,’ ‘[any] of the above,’ ‘trained to do all [of the above] but not much experience,’ ‘pressure of increased workload due to reduced staff levels,’ ‘time prioritization and referrals to seniors,’ ‘management plan,’ ‘communication with colleagues and prioritization.’
The most requested clinical scenarios by medical students were the unresponsive patient (61.46%), sepsis (57.29%), cardiac arrest (51.04%), and trauma (50%), with two free text answers requesting sessions on all survey options, and one respondent requesting anaphylaxis. Again, the answers selected by the foundation doctors both correlated and did not correlate with these as 40.48% felt prepared to manage an unresponsive patient, 96.43% felt prepared for sepsis, 65.48% felt prepared for cardiac arrest, and only 17.86% felt prepared for trauma.
The foundation doctors felt least prepared to manage burns (69.05%), intoxicated patients (64.29%), trauma (38.33%), and endocrine emergencies (58.33%). In their free text answers the foundation doctors felt that acute kidney injury, falls, major haemorrhage, electrolyte abnormalities, and self-discharge should also be included. Survey respondents were not asked how the simulation scenarios ought to be executed. Survey responses for learning domains and clinical scenarios underwent chi-square testing to yield Yates corrected p-values of
Respondents were provided with a final free text box to provide further input into the curriculum. The most frequent answer was ‘more of the above.’ This was followed by requests for general scenarios where many differentials had to be considered and excluded. The next few themes appeared with equal frequency: common scenarios, nontechnical learning including sessions that incorporated handover to seniors, prioritising and escalating patient care. Violence and prehospital triage were also requested.
Foundation doctors described feeling poorly prepared to manage traumatic and paediatric presentations. These were followed by acute psychiatry and cardiology, as well as cardiac arrest and chest pain. The 95.96% of foundation doctors who had undertaken simulation training as undergraduates were asked to name a scenario in clinical practice that the aforementioned training had prepared them well for: twenty-eight respondents selected cardiac arrest and chest pain, seventeen chose sepsis, fifteen chose shortness of breath, and nine selected shock. Notably, other respondents described nontechnical aspects of acute scenarios such as remaining calm, working in a team, and remaining focused amid distractions and demands from other health care professionals, as well as communication skills.
Foundation doctors fed back that undergraduate simulation should incorporate teaching on altered mental status and common bleeps in a realistic setting i.e. the learner is in role and the scenario is complex, that is, the learner is unaided and the patient does not respond to first line treatment. There were further requests for teamwork and trauma. A small number of respondents suggested that sessions should incorporate prioritisation, handover, and experience of working amid hassle by nurses and real-time impediments including requesting interventions and writing prescriptions.
Descriptive statistics: frequency tables for survey responses
Figure 4. Frequency of answers given by medical students and foundation doctors asked about learning domains to be incorporated in the simulation scenarios
| Scenario | Medical students (%) | Foundation doctors felt prepared by undergraduate studies | Foundation doctors did not feel prepared by undergraduate studies | Yates’ p-value |
| Shortness of Breath | 23 (23.96) | 79 (94.05) | 2 (2.38) | |
| Chest pain | 32 (33.33) | 77 (91.67) | 5 (5.95) | |
| Shock | 44 (45.83) | 61 (72.62) | 15 (17.86) | |
| Cardiac arrest | 49 (51.04) | 55 (65.48) | 24 (28.57) | 0.00002256 |
| Acute abdomen | 32 (33.33) | 62 (73.81) | 17 (20.24) | |
| Sepsis | 55 (57.29) | 81 (96.43) | 3 (3.57) | |
| Endocrine emergencies | 23 (23.96) | 29 (34.52) | 49 (58.33) | 0.00005005 |
| Unresponsive patient | 59 (61.46) | 34 (40.48) | 40 (47.62) | 0.01288102 |
| Trauma | 48 (50) | 15 (17.86) | 49 (58.33) | 0.00000032 |
| Intoxication | 20 (20.83) | 15 (17.86) | 54 (64.29) | 0.00086438 |
| Delirium/psychosis | 20 (20.83) | 30 (35.71) | 42 (50) | |
| Burns | 23 (23.96) | 6 (7.14) | 58 (69.05) | |
| NAI | 9 (9.38) | 15 (17.86) | 47 (55.95) | |
| Sick child | 33 (34.38) | 21 (25) | 48 (57.14) | 0.00019085 |
| Other | 3 (3.13) | 0 (0) | 5 (5.95) | Chi-square test inappropriate for frequency of 0 |
Figure 5. Frequency of answers given by medical students and foundation doctors asked about clinical scenarios for inclusion in the simulation scenarios
Graphical comparison of medical student and foundation year doctor survey responses
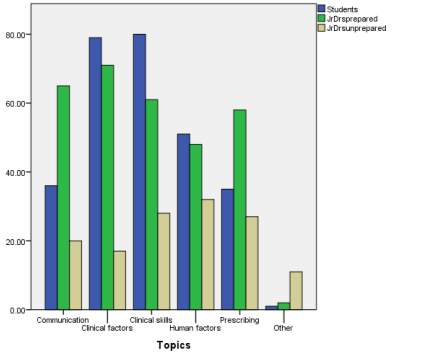
Figure 6. Graphical comparison of survey answers on learning domains to be incorporated in the simulation scenarios
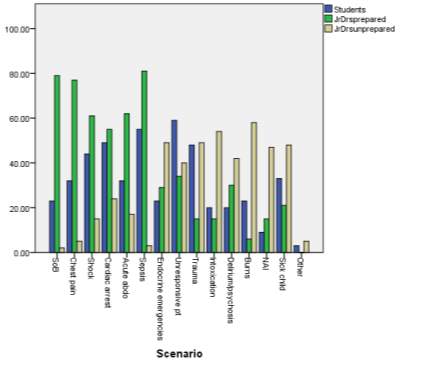
Figure 7. Graphic comparison of survey answers on clinical scenarios for inclusion in the simulation scenarios
Qualitative data: free text responses

Figure 8. Word cloud depicting themes from undergraduate free text feedback on ‘anything else that you think should be included in final year simulation training’ weighted according to frequency

Figure 9. Word cloud depicting free text feedback from foundation doctors on ‘a situation that you felt poorly prepared for as a junior doctor working in Emergency Medicine’ weighted according to frequency

Figure 10. Word cloud depicting free text feedback from foundation doctors on ‘a situation that your simulation prepared you well for’ weighted according to frequency

Figure 11. Word count depicting free text feedback from foundation doctors on ‘anything else that should be included in undergraduate simulation’ weighted according to frequency
Discussion
Curriculum consensus
Regarding learning domains, the differing prioritisation of human factors by medical students and foundation doctors may be attributable to their different experiences: medical students will approach the questionnaire from the perspective of what they do not know, perhaps without the experience to understand what will be important after graduation.
Foundation doctors, on the other hand, will approach the questionnaire with experience of what the job entails and this is reflected in their qualitative answers describing a desire for training that reflects the realities of prioritisation and work-based communication. It is encouraging that most foundation doctors feel prepared for clinical factors, but an arguably significant minority do not. The medical student and foundation doctor responses support clinical vignettes focusing on unresponsive patients and trauma. However, there is less consensus on whether the other two scenarios should be on cardiac arrest and sepsis; or burns, intoxicated patients, and endocrine emergencies.
Here the quantitative data is not able to provide insight into whether medical students chose these answers because they perceived these topics to be important or because they feel underprepared to manage them, or indeed whether this is a product of the relative importance attributed to each topic by those educating them. A combination is likely. The scenarios that the foundation doctors feel less prepared to manage may also be less important to their working reality than cardiac arrest and sepsis and so it would be premature to remove these from the running altogether.
Free text feedback from undergraduates reflects both a desire for more simulation and a perception of simulation as a valid way to help them feel prepared. There is a sense of undergraduates wanting to work through everything in simulation before they encounter it in clinical practice. Foundation doctors’ feedback that they do not feel well prepared to manage trauma and sick children, areas with heavy specialist involvement and the bulk of training occurring at postgraduate level, suggests that there is scope to begin preparing trainees for these high-stakes emergencies earlier in their careers. That three respondents fed back feeling poorly prepared to manage cardiac arrest is at odds with the majority responding that their undergraduate simulation had prepared them well for this. However, this could be explained by the later free text comment that simulated cardiac arrest should have learners in role, arriving as a junior to a busy cardiac arrest site where the team is already at work and the learner needs to use their initiative to involve themselves.
Postgraduate feedback that simulation has enhanced preparedness to manage common emergencies including cardiac arrest, sepsis, and shock, as well as acute presenting complaints such as chest pain and shortness of breath, supports their inclusion in our curriculum. Foundation doctor feedback on clinical and nontechnical components supports the dual potential of simulation to enable trainees to simultaneously develop clinical and nontechnical understanding by implementing management in a realistic environment.
Comparison of the survey results with the curricula review is encouraging although the Plymouth and Peninsula curriculum also included obstetric emergencies. However, these could be incorporated into scenarios focusing on the acute surgical abdomen or shock. The success of inter-professional simulation sessions at Plymouth and Peninsula medical schools lends weight to the foundation doctors’ answers about human factors. It has already been mentioned that the curricula review was not lucrative and so the extent to which it can be used to inform local curriculum design is limited. Future enquiry ought to be via standardised questionnaire to increase yield.
In a similar vein, it is also challenging to compare the survey results with the findings of the literature review as the literary canon largely asked different questions. All of the clinical scenarios are validated by the International Federation for Emergency Medicine.(56) Many studies looked retrospectively at what their simulation sessions had achieved rather than asking what they should ideally include. The review elucidated 9 review articles, 5 best evidence papers, with the remainder being descriptive studies. The majority of papers designed simulation scenarios to represent departmental activity or at random, with the exception of two: one of which conducted focus groups of final year students, foundation year doctors, and relevant resuscitation, critical care and governance staff to produce a consensus on hypovolaemia dehydration, opiate overdose, chronic obstructive pulmonary disease, pneumonia, and sepsis.(18) The other paper conducted a literature review and Delphi study which was then mapped to the Emergency Medicine curriculum for American postgraduate trainees.(57)
The resulting body of core Emergency Medicine competencies for medical students could be used to guide formative assessment of the simulation scenarios. Although the survey respondents were not asked about implementation, reviewing the literature revealed two evidence-based guides (42, 50) that will guide the development of the four sessions.
Limitations
This study’s mixed methodology has provided results with both breadth and context. However, the results of this paper were triangulated concurrently, which meant that the findings of the curricula and literature reviews could not be integrated into subsequent enquiry. It would have been better to explore each component sequentially, but that was beyond the scope of this small project.
The curricula review was limited by access to medical school curricula as the institutions did not consistently provide open access to these documents via their websites. In addition, the curricula appeared quite reticent documents not sufficient to describe the full richness and variety of teaching and learning activities going on at medical school, which made it difficult to conclude whether simulation does or does not comprise a significant part of mainstream medical curricula. Anecdotal enquiry suggests that there is a paucity of simulation in modern undergraduate medical teaching. Two medical schools that did not mention simulation in the curricula did describe simulation elsewhere on their websites, suggesting that simulation is not only underutilised but under-advertised.
The literature review was conducted as a three-stage search with reference checking to make it comprehensive. However, a systematic review was beyond the scope of this project. Further, there was no meta-analysis of the body of literature so different study types are all equally represented by thematic analysis and the findings are without statistical rigour. Content analysis into thematic units was undertaken manually which may have introduced confirmation bias. However, this is generally held to be a reliable method of interpretation and the number of free text respondents was too small to generate usable results from content analysis software. Thematic analysis was limited by what information had been published and as noted above, many studies selected topics to reflect departmental activity rather than by rigorous selection process. It would be valuable to weight the two studies that did employ surveys, focus groups, and the gold-standard Delphi study against the findings of this paper and map the results against IFEM to generate a more informed curriculum.
The sample size to be surveyed was not prospectively decided, rather the author sampled everyone to mitigate an anticipated low response rate. In addition, the survey was not mandatory, and so this may introduce response bias as more motivated students and doctors are more likely to reply and it could be argued that the students who would most benefit from this training will not have contributed. As acknowledged previously, at the time of writing the survey had been sent out to medical students and foundation doctors at different times, leading to a different number of respondents, which may bias the results towards the medical students as 96 of them responded compared with 87 foundation doctors. No demographic or educational data was collected from the respondents. Details of university placements and foundation jobs may have been useful to further inform the areas in which medical students requested teaching and foundation doctors felt underprepared.
Next steps
Findings of this study would ideally be used to generate a working curriculum model that could then undergo Delphi protocol as is the gold standard. There should be more research into how to implement simulation curricula. Further, a more thorough study would comprise enquiry into the weaknesses and limitations of simulation as a teaching tool and indeed the perils of overreliance on simulation so that this could be used to implement a curriculum of the greatest benefit to learners.
Conclusion
This paper contributes to the emerging body of literature on simulation in undergraduate medical education. Its mixed methodology generates key data and context that can form the skeleton for a simulation curriculum that is informed by learners and by theory. The paper has elucidated clinical scenarios and nontechnical learning domains that will underpin the development of final year medical students into prepared foundation doctors, before suggesting where future enquiry would be best undertaken.
References
1. Bird G, Swampillai C, Lacey O, Curran I. Recently graduated doctors’ self-reported preparedness in the management of acutely ill patients. A 5 year review of London deanery’s foundation programme simulation training: a clinical challenge for medical education? 2012;38: S301
2. Mastoiridis S, Shanmugarajah K, Kneebone R. Undergraduate education in trauma medicine: the students’ verdict on current teaching. Med Teach2011.
3. Quality Assurance Agency for Higher Education. Subject Benchmark Statement for Medicine. 2002.
4. General Medical Council. Tomorrow’s Doctors. 2009.
5. General Medical Council. The state of medical education and practice in the UK. 2011.
6. Department of Health. A framework for technology enhanced learning. 2011.
7. Borggreve AS, Meijer JM, Schreuder HW, Ten Cate O. Simulation-based trauma education for medical students: A review of literature. Med Teach. 2017:1-8.
8. Aggarwal R, Mytton OT, Derbrew M, Hananel D, Heydenburg M, Issenberg B, et al. Training and simulation for patient safety. Qual Saf Health Care. 2010;19 Suppl 2:i34-43.
9. Paskins Z, Peile E. Final year medical students’ views on simulation-based teaching: a comparison with the Best Evidence Medical Education Systematic Review. Med Teach. 2010;32(7):569-77.
10. Tallentire VR, Smith SE, Skinner J, Cameron HS. Understanding the behaviour of newly qualified doctors in acute care contexts. Med Educ2011.
11. Couto TB, Farhat SC, Geis GL, Olsen O, Schvartsman C. High-fidelity simulation versus case-based discussion for teaching medical students in Brazil about pediatric emergencies. Clinics (Sao Paulo). 2015;70(6):393-9.
12. Heitz C, Eyck RT, Smith M, Fitch M. Simulation in medical student education: survey of clerkship directors in emergency medicine. West J Emerg Med. 2011;12(4):455-60.
13. Quilici AP, Abrao KC, Timerman S. Simulation in emergency medicine training: A model curriculum for medical undergraduates. Resuscitation. 2010;1):S92.
14. Tews MC, Hamilton GC. Integrating emergency medicine principles and experience throughout the medical school curriculum: Why and how. Academic Emergency Medicine. 2011;18(10):1072-80.
15. Datta R, Upadhyay KK, Jaideep CN. Simulation and its role in medical education. Med J Armed Forces India2012.
16. Goldberg S. Critical actions in common floor emergencies: A multi-disciplinary, multimodality course for incoming first year residents. Annals of Emergency Medicine. 2014;1):S147-S8.
17. Brandao CF, Collares CF, Marin HF. Student perception on high-fidelity simulation during the medical clerkship. Stud Health Technol Inform. 2013;192:960.
18. Watmough S, Box H, Bennett N, Stewart A, Farrell M. Unexpected medical undergraduate simulation training (UMUST): can unexpected medical simulation scenarios help prepare medical students for the transition to foundation year doctor? BMC Med Educ. 2016;16:110.
19. Shepherd L, Chahine S, Klingel M, Zibrowski E, Meiwald A, Lingard L. Reducing length of stay and satisfying learner needs. Perspect Med Educ. 2016;5(3):170-8.
20. Koh J, Dubrowski A. Merging Problem-Based Learning with Simulation-Based Learning in the Medical Undergraduate Curriculum: The PAIRED Framework for Enhancing Lifelong Learning. Cureus. 2016;8(6):e647.
21. Coolen EH, Draaisma JM, Hogeveen M, Antonius TA, Lommen CM, Loeffen JL. Effectiveness of high fidelity video-assisted real-time simulation: a comparison of three training methods for acute pediatric emergencies. Int J Pediatr. 2012;2012:709569.
22. Damon Dagnone J, Takhar A, Lacroix L. The Simulation Olympics: a resuscitation-based simulation competition as an educational intervention. CJEM. 2012;14(6):363-8.
23. Ellison S, Sullivan C, McCullough R. No longer waiting for an accident to happen: Simulation in emergency medicine. Mo Med. 2013;110(2):133-8.
24. Van Heukelom JN, Begaz T, Treat R. Comparison of postsimulation debriefing versus in-simulation debriefing in medical simulation. Simul Healthc. 2010;5(2):91-7.
25. Stroben F, Schröder T, Dannenberg KA, Thomas A, Exadaktylos A, Hautz WE. A simulated night shift in the emergency room increases students’ self-efficacy independent of role taking over during simulation. BMC Med Educ. 2016;16:177.
26. Rezmer J, Begaz T, Treat R, Tews M. Impact of group size on the effectiveness of a resuscitation simulation curriculum for medical students. Teach Learn Med. 2011;23(3):251-5.
27. Muniandy RK, Nyein KK, Felly M. Improving the self-confidence level of medical undergraduates during emergencies using high fidelity simulation. Med J Malaysia. 2015;70(5):300-2.
28. Mohamed-Ahmed R, Daniels A, Goodall J, O’Kelly E, Fisher J. ‘Disaster day’: global health simulation teaching. Clin Teach. 2016;13(1):18-22.
29. Freund Y, Philippon AL, Bokobza J, Carreira S, Riou B, Duguet A. A 1-h simulation-based course on basic life support durably enhances confidence among medical students. Eur J Emerg Med. 2013;20(2):145-6.
30. Cooper D, Wilbur L, Phillips J, Milgrom L, Ellender K, Huffman G. Can interprofessional simulation improve physician – Nurse communication and error reporting confidence? Academic Emergency Medicine. 2012;19:S317-S8.
31. Cole LA, Natal B, Fox A, Cooper A, Kennedy CA, Connell ND, et al. A Course on Terror Medicine: Content and Evaluations. Prehosp Disaster Med. 2016;31(1):98-101.
32. Brown CW, Howard M, Morse J. The use of trauma interprofessional simulated education (TIPSE) to enhance role awareness in the emergency department setting. J Interprof Care. 2016;30(3):388-90.
33. Sigalet E, Donnon T, Grant V. Undergraduate students’ perceptions of and attitudes toward a simulation-based interprofessional curriculum: the KidSIM ATTITUDES questionnaire. Simul Healthc. 2012;7(6):353-8.
34. Henn P, Power D, Smith SD, Power T, Hynes H, Gaffney R, et al. A metric-based analysis of structure and content of telephone consultations of final-year medical students in a high-fidelity emergency medicine simulation. BMJ Open. 2012;2(5).
35. Ruesseler M, Weinlich M, Müller MP, Byhahn C, Marzi I, Walcher F. Simulation training improves ability to manage medical emergencies. Emerg Med J. 2010;27(10):734-8.
36. Ko PY, Scott JM, Mihai A, Grant WD. Comparison of a modified longitudinal simulation-based advanced cardiovascular life support to a traditional advanced cardiovascular life support curriculum in third-year medical students. Teach Learn Med. 2011;23(4):324-30.
37. Association for the Study of Medical Education. Understanding Medical Education: Evidence, Theory, and Practice: Wiley-Blackwell; 2010.
38. McGaghie WC, Issenberg SB, Cohen ER, Barsuk JH, Wayne DB. Does simulation based medical education with deliberate practice yield better results than traditional clinical education? A meta-analytic comparative review of the evidence. Acad Med2011.
39. Cook DA, Hatala R, Brydges R, Zendejas B, Szostek JH, Wang AT, Erwin PJ, Hamstra SJ. Technology-enhanced simulation for health professions education: a systematic review and meta-analysis. JAMA2011.
40. Tengattini M, Ingrassia P, Barra FL, Ragazzoni L, Barra F, Della Corte F. Efficacy of a disaster medicine course for undergraduates. European Journal of Emergency Medicine. 2011;18 (5):297-8.
41. Magee H, Howes D. Exploring the challenges and feasibility of using high-fidelity simulation to train medical students in cardiac arrest management. Canadian Journal of Emergency Medicine. 2012;14:S48-S9.
42. Motola I, Devine LA, Chung HS, Sullivan JE, Issenberg SB. Simulation in healthcare education: a best evidence practical guide. AMEE Guide No. 82. Med Teach. 2013;35(10):e1511-30.
43. Keskinis C, Bafitis V, Karailidou P, Pagonidou C, Pantelidis P, Rampotas A, et al. The use of theatre in medical education in the emergency cases school: an appealing and widely accessible way of learning. Perspect Med Educ. 2017.
44. Carter K, Golden A, Martin S, Donlan S, Hock S, Babcock C, et al. Results from the First Year of Implementation of CONSULT: Consultation with Novel Methods and Simulation for UME Longitudinal Training. West J Emerg Med. 2015;16(6):845-50.
45. Lamba S, Wilson B, Natal B, Nagurka R, Anana M, Sule H. A suggested emergency medicine boot camp curriculum for medical students based on the mapping of Core Entrustable Professional Activities to Emergency Medicine Level 1 milestones. Adv Med Educ Pract. 2016;7:115-24.
46. Manthey DE, Ander DS, Gordon DC, et al. Emergency medicine clerkship curriculum: an update and revision. Acad Emerg Med; 2010.
47. Sperling JD, Clark S, Kang Y. Teaching medical students a clinical approach to altered mental status: simulation enhances traditional curriculum. Med Educ Online. 2013;18:1-8.
48. Zabar B, Dodge K, Safdar B, Moore C, Roman S, Sather J, et al. The perceived stress and appropriateness of simulated death in undergraduate medical education. Academic Emergency Medicine. 2010;17:S66.
49. Luigi Ingrassia P, Ragazzoni L, Carenzo L, Colombo D, Ripoll Gallardo A, Della Corte F. Virtual reality and live simulation: a comparison between two simulation tools for assessing mass casualty triage skills. Eur J Emerg Med. 2015;22(2):121-7.
50. McGaghie WC, Issenberg SB, Petrusa ER, Scalese RJ. A critical review of simulation-based medical education research: 2003-2009. Med Educ2010.
51. Cooper DD, Wilson AB, Huffman GN, Humbert AJ. Medical students’ perception of residents as teachers: comparing effectiveness of residents and faculty during simulation debriefings. J Grad Med Educ. 2012;4(4):486-9.
52. Blackstock U, Munson J, Koziatek C, Szyld D. Bedside ultrasound skills acquisition by medical students on emergency medicine rotation. Academic Emergency Medicine. 2013;1):S85-S6.
53. Cheung JJ, Koh J, Brett C, Bägli DJ, Kapralos B, Dubrowski A. Preparation With Web-Based Observational Practice Improves Efficiency of Simulation-Based Mastery Learning. Simul Healthc. 2016;11(5):316-22.
54. Haji FA, Cheung JJ, Woods N, Regehr G, de Ribaupierre S, Dubrowski A. Thrive or overload? The effect of task complexity on novices’ simulation-based learning. Med Educ. 2016;50(9):955-68.
55. Sande MK. Integration of an audience response system into simulation-based training: An educational technology enhancement. Academic Emergency Medicine. 2014;1):S345.
56. International Federation for Emergency Medicine. Model Curriculum for Emergency Medicine. 2009.
57. Santen SA, Peterson WJ, Khandelwal S, House JB, Manthey DE, Sozener CB. Medical student milestones in emergency medicine. Acad Emerg Med2014.
Cite This Work
To export a reference to this article please select a referencing stye below:
Related Services
View all


Related Content
All TagsContent relating to: "Health and Social Care"
Health and Social Care is the term used to describe care given to vulnerable people and those with medical conditions or suffering from ill health. Health and Social Care can be provided within the community, hospitals, and other related settings such as health centres.
Related Articles

DMCA / Removal Request
If you are the original writer of this dissertation and no longer wish to have your work published on the UKDiss.com website then please: