Literature Review on Health Benefits of Antioxidants in Coffee
Info: 9156 words (37 pages) Example Literature Review
Published: 13th Apr 2021
Tagged: Food and Nutrition
Table of Content
Introduction…………………………………………………………………………………………………………….2
Structure, Properties and Biological Activities of Antioxidant………………………………….3
Caffeine…………………………………………………………………………………………………………..3
Chlorogenic acid…………………………………………………………………………………………..…4
Caffeic acid……………………………………………………………………………………………………..4
Antioxidant and Human Disease……………………………………………………………………………..5
Antioxidant and Cancer…………………………………………………………………………………..6
Liver Cancer…………………………………………………………………………………………………….7
Colon Cancer…………………………………………………………………………………………………..8
Breast Cancer………………………………………………………………………………………………….9
Prostate Cancer………………………………………………………………………………………………10
Antioxidants and Type 2 Diabetes Mellitus……………………………………………………..11
Limitations and Further Research Direction……………………………………………………………13
Conclusion………………………………………………………………………………………………………………14
Reference……………………………………………………………………………………………………………….14
Antioxidants in Coffee and Their Potential Health Benefits
- Introduction
Coffee is a popular drink worldwide, in Australia; it is the second highest type of beverage consumed after water (Australian Bureau of Statistics, 2014). Although coffee consumption has showed some negative health effects, such as increased risk of spontaneous abortion in pregnant women, habitual coffee intake is associated with a range of health benefits due to its rich antioxidant profile (Preedy, 2014). It was found that coffee has more antioxidant activity than green tea, black tea and red wine (Bowden, 2007). Furthermore, coffee ranked eleventh in terms of the antioxidant content of different food by serving size, after several types of berries (Pérez-Jiménez et al., 2010). While eating several servings of berries are rare, drinking a few cups of coffee a day is more common, therefore, coffee is known as the biggest source of dietary antioxidant (Perez-Jimenez et al., 2011; Zujko et al., 2012).
Antioxidants are broadly divided into exogenous and endogenous. While human body is capable of producing antioxidant, it is usually insufficient, thus dietary source of antioxidant is also vital (Zampelas and Micha, 2015). Antioxidants are molecules that inhibit oxidation, which is process characterized as the loss of electrons. Free radicals are produced in oxidation. These free radicals can further initiate chain reaction of oxidizing other molecules, causing cell damage or even cell death (Bagchi, Moriyama and Swaroop, 2016). Nevertheless, antioxidants are capable to protect the body from the detrimental effects brought by free radicals. Caffeine, caffeic acid, chlorogenic acid and hydroxyhydroquinone are antioxidants that can be found in coffee (Butt and Sultan, 2011).
Numerous findings indicate that antioxidants present in coffee play a role in delaying or preventing type 2 diabetes and degenerative conditions, including several types of cancer (Bagchi, Moriyama and Swaroop, 2016; Hoelzl et al., 2010). As a result, it is essential to understand the mechanism and action of antioxidant in preventing the development of chronic disease. This knowledge is vital given that coffee is a highly consumed beverage in Australia. The health authority can educates the general public and raises their awareness regarding the health promoting property of their beloved beverage. For maintaining good health, prevention is better than medical treatment in terms of cost and effectiveness. This review summarises the present understanding of the biological effects of exogenous antioxidant and their role in human health and disease from a range of epidemiological, in vitro and in vivo studies. In particular, colon, liver, breast and prostate cancers and type 2 diabetes mellitus are discussed due to their contribution to mortality of Australians and increasing prevalence in Australia.
- Structure, Properties and Biological Activities of Antioxidant
Coffee contains a range of antioxidants that contributes to its health benefit. As mentioned in the introduction, antioxidants are able to protect the body by inhibiting oxidation. In human, normal metabolism generates free radicals as by-products. Damage caused by free radicals can be serious when the generation of free radicals increases, as it can leads to the development of various pathological and chronic conditions (Herrera et al., 2009). However, antioxidants can mitigate the damage brought by free radicals. Huang, Ou, and Prior (2005) defined dietary antioxidants as “substances which can sacrificially scavenge reactive oxygen/nitrogen species to stop radical chain reactions, or can inhibit the reactive oxidants from being formed in the first place”. In addition to this definition, antioxidants can neutralize free radicals or terminate the chain reaction by being oxidized themselves (Bagchi, Moriyama & Swaroop, 2016).
While cancer, heart disease, diabetes and premature ageing are linked to inadequate antioxidant levels or function in the body, the properties and actions of antioxidants are worth investigating (Siti, Kamisah and Kamsiah, 2015). The main antioxidants found in coffee are described while their chemical structures, concentration in coffee and other biological activities are illustrated in Table 1.
Caffeine
Caffeine, also known as 1,3,7-trimethylxanthine, is a purine alkaloid and a natural occurring substance found in various plants. Coffee is a main source of caffeine where 50% of caffeine intake for Australians comes from coffee (Australian Beverage, 2013). During the coffee bean roasting process, caffeine is not significantly altered in terms of its chemical structure and the amount of caffeine in beans are not remarkably reduces, yet a small amount can be lost due to sublimation (Chu, 2012). Additionally, in the human body, caffeine is rapidly and almost fully digested and absorbed in the stomach and small intestine and then distributed to tissues, including the brain (Ludwig et al., 2014). Liver is the major site of caffeine metabolism where a serious of demethylation occurs. After absorption, caffeine exhibits its physiological function via the antagonism of the A1 and A2 subtypes of the adenosine receptor located in the brain (Frost-Meyer & Logomarsino, 2012). Nevertheless, high level of caffeine is circulating around the body after coffee consumption with a maximum concentration observed one hour after consumption (Ludwig et al., 2014).
Chlorogenic acid
Chlorogenic acid (CGA) is an ester of caffeic acid and (-) quinic acid. Nevertheless, CGA is also known as 3- O-caffeoylquinic acid (3-CGA) or 5-O-caffeoylquinic acid (5-CQA), where the lateral is the most common form (Meng et al., 2013). Unlike caffeine, up to 95% of CGA can be lost during coffee bean roasting process (Clifford, 1985). The proportion lost depends on the degree of roasting, where dark roasting contributes to the greatest loss in CGAs compared to light roasting (Bagchi, Moriyama & Swaroop, 2016). Some of this destroyed CGAs account for quinic acid and caffeic acid. Although CGAs are lost in a significant extent during roasting, it is still the most abundant antioxidant found in coffee, as shown in Table 1. CGAs are not readily absorbed by the human body due to its structure. Approximately one- third of the CGAs are absorbed in the upper gastrointestinal (GI) tract while the remaining passes through the GI tract, reaching the colon and are hydrolysed by the colonic microflora. After absorption, the hydrolysed products of CGAs and a small quantity of intact CGAs are found circulating in the plasma (Watson, Preedy & Zibadi, 2014).
Caffeic acid
Caffeic acid, or 3,4-dihydroxycinnamic acid, is a phenolic acid that derived from chlorogenic acid during roasting (Preedy, 2013). The ingested caffeic acid is absorbed in the alimentary tract, with the absorption rate more than twice higher than that of chlorogenic acid (Bagchi, Moriyama & Swaroop, 2016). The absorption was suggested to be passive non-ionic diffusion in the stomach and active sodium-dependent transport mechanism in the small intestine (Shahidi & Naczk, 2004). Caffeic acid is also found circulating in the plasma in a dose dependent manner, with maximum concentration one hour after coffee consumption (Shahidi & Naczk, 2004).
Table 1: Concentrations, chemical structures and biological activities of antioxidants in coffee
| Antioxidant | Concentration (mg/ml) | Chemical structure | Other biological activity |
| Caffeine | 0.27 – 1.85a | 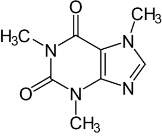 |
CNS stimulationb; increase alertnessb; increase metabolic rate and energy expenditurec; improves performance of the dopaminergic systemd |
| Chlorogenic acid | 0.35 – 1.27a | 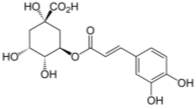 |
Antibacterial and anti- inflammatory activitye; Postprandial reduction in rate of glucose release into bloodstreamf; increase insulin sensitivityg; inhibit oxidation of LDLg |
| Caffeic acid | 0.18 – 0.88a | 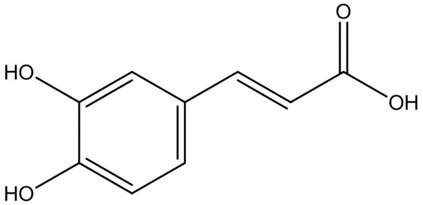 |
DNA methylation inhibitionh; inactivation of pathways involved in tumorigenic processh; carcinogenic inhibiting activityi; |
Reference: Talwar, Hasnain & Sarin (2016)a; Frost-Meyer & Logomarsino (2012)b; Heckman, Weil & de Mejia (2010)c; Trevitt et al. (2009)d; Bowden (2007)e; Bagchi, Moriyama & Swaroop (2016)f; Shearer et al. (2003)g; Vucic, Brown & Lam (2008)h; Antol (2002)i
- Antioxidant and Human Disease
When the body has low levels of antioxidants, damage or death to cells can happen via a process called oxidative stress. Oxidative stress is a state of imbalance between antioxidants and oxidants, in favour of the lateral, which results in damaging effects (Siti, Kamisah and Kamsiah, 2015). Oxidants are also known as reactive oxygen species (ROS), which includes free radicals such as O2 − (superoxide) and OH (hydroxyl) (Siti, Kamisah and Kamsiah, 2015). Generally, human body is capable of dealing with this imbalance due to the presence of the antioxidant defense system. However, when the production of ROS exceeds the limit of antioxidants’ defense, a number of pathophysiological conditions could occur (Siti, Kamisah and Kamsiah, 2015). Thus, oxidative stress is a known contributor to the onset of many diseases.
− (superoxide) and OH (hydroxyl) (Siti, Kamisah and Kamsiah, 2015). Generally, human body is capable of dealing with this imbalance due to the presence of the antioxidant defense system. However, when the production of ROS exceeds the limit of antioxidants’ defense, a number of pathophysiological conditions could occur (Siti, Kamisah and Kamsiah, 2015). Thus, oxidative stress is a known contributor to the onset of many diseases.
On the other hand, there are increasing evidence showing the protective property of antioxidants against oxidative damage, therefore they may have the potential to prevent diseases associated with oxidative stress (Bravo et al., 2013).
Antioxidant and Cancer
Cancer is a genetic disease that is characterized as the uncontrolled division of abnormal cells (National Cancer Institute, 2015). Although cancer causing genetic changes can be inherited, for most people, cancer arises as a result of DNA damage (National Cancer Institute, 2015). Chemical substances including nicotine from cigarette smoking, free radicals from metabolism as well as physical exposure to radiation such as ultraviolet rays from the sun are factors that contribute to DNA damage (Lodish, Berk & Zipursky, 2000).
In the last decade, there were increasing studies demonstrated the relationship between coffee and cancer, where a high coffee consumption may reduce the risk of some types of human cancer, and this risk reduction is mainly associated with its antioxidant activities (Nkondjock, 2009). In particular, antioxidants were found to have genoprotective properties. A vivo study carried out by Bakuradze et al. (2010) demonstrated the potential of antioxidant found in coffee in protecting DNA from damage. Furthermore, a vitro study illustrated the presence of caffeic acid or chlorogenic acid inhibited the cancer causing DNA methylation in a concentration-dependent manner (Lee, 2006). Bravo et al. (2013) studied the genoprotective effect of caffeine in human cells. It was indicated that caffeine significantly reduced the increase of ROS level and DNA strand breaks induced by a reactive oxygen species – hydrogen peroxide. This study also suggested pretreatment of cell with caffeine can reduce oxidative DNA damage. Another research also investigated the effect of chlorogenic acid on human health. Biomarkers of both treatment and placebo group were analysed and it was concluded that chlorogenic acid can protect human against oxidative damage of DNA, membrane lipids and proteins (Hoelzl et al., 2010).
Based on these evidences, it was certain that antioxidants in coffee had a close association with cancer. However, this relationship was not seen in all types of cancer. Results of recent in vitro, in vivo and epidemiological studies of several cancers in relation to coffee consumption were summarized.
Liver Cancer
Liver cancer is not a very common condition in Australia; however, it is a growing cause of cancer death in Australia, given that the incidence to death ratio is close to 1 (Cancer Australia, 2017). On the other hand, many studies had consistently demonstrated the inverse relationship between coffee intake and liver cancer. This could be due to the protective properties of coffee against oxidative stress-induced liver cell damage (Nkondjock, 2009).
Ohishi et al. (2008) conducted a study that involved 224 liver cancer subjects and 644 controls and it was concluded that daily coffee consumption was associated with decreased risk for liver cancer. A study in Singapore examined 63,257 middle-aged and elderly Chinese men and women, a population (age group) that had higher risk of developing liver cancer (Johnson et al., 2011). It illustrated that high levels of coffee consumption were associated with reduced risk of liver cancer. Results also showed individuals who consumed three or more cups of coffee per day experienced a statistically significant 44% reduction in risk of compared with non-coffee drinkers. Another study in Finland showed a similar finding. This study evaluated 27,037 Finnish men aged 50–69 in terms of coffee intake and liver cancer incidence and mortality. The inverse association was suggested and relative risk (RR) of incidence per cup per day was 0.82 while RR was 0.55 for mortality (Lai et al., 2013). In addition, a case-control study in Japan found a decreased risk in liver cancer mortality in daily coffee drinkers compared to non-drinkers, given that OR was 0.49 (Wakai et al., 2007).
Moreover, there were studies that related the relative risk of liver cancer development to the amount of coffee intake per day or per week. A Finnish study on 60,323 participants, followed-up for 19 years, showed an RR of 0.32 for coffee drinkers of at least 8 cups a day as compared with 1 cup or less (Hu et al., 2008). A Japanese study that involved a 13 years follow up on 18,815 subjects demonstrated a RR of 0.54 for drinkers of 3 or more cups per day compared to rare or non-drinkers (Inoue et al., 2009). A hospital-based case-control study in Italy included 185 liver cancer subjects and 418 controls. It was found the risk decreased with increasing levels of consumption (OR = 0.4) as compared to people who drank more than 14 cups per week (Montella et al., 2007).
Colon Cancer
In Australia, colon cancer is third most commonly diagnosed cancer in 2013 and the second leading cause of cancer deaths in 2014 (Cancer Australia, 2017). In the report published by World Cancer Research Fund in 2007, the association between coffee consumption and the risk of developing colon cancer was not clear. Although there were studies focusing on this field back then, the result from limited number of studies were insufficient to conclude the relationship between the two. Nevertheless, during the past five to ten years, more clinical and epidemiological studies were conducted and there was increasing evidence showing the positive effect of coffee to prevent development of colon cancer. In particular, polyphenols present in coffee protect against colon tumor formation was demonstrated in animal studies, possibly through their antioxidant properties (Higdon & Frei, 2006). Furthermore, a more recent research suggested chlorogenic acid had the ability to inhibit the viability of human colon cancer cells, thus contributed to a lowered risk of colon cancer (Hou et al., 2017).
Sugiyama et al. (2010) studied 37,742 subjects, followed up for ten years and found decreased risk of colon cancer with a moderate coffee intake in women. A Japanese community based case-control study explored the association between coffee intake and risk of colon cancer by conducting computer-assisted interview and collecting food intake data from 816 colon cancer subjects and 815 community-based controls. Result indicated a significantly decreased risk in individuals who consume up to three cups of coffee per day (Wang et al., 2013). Similarly, a study in Singapore assessed food consumption data in over 60,000 subjects for ten years through in-person interviews and questionnaires showed regular coffee drinkers (two or more cups daily) were at lower risk in developing advanced colon cancer than rare or non-coffee drinkers, given the hazard ratio was 0.56 (Peterson et al., 2009). Sinha et al. (2012) evaluated coffee intake habits in 489,706 subjects via self-administered questionnaire and followed up for ten years. Compared with non-coffee drinkers, habitual coffee consumed individuals had a lower risk of developing colon cancer. Statically, subjects consumed 4–5 cups coffee per day had a hazard ratio (HR) of 0.85 while consumption of more than 6 cups per day had a HR of 0.74.
A more recent clinical study focused on influence of coffee on cancer recurrence and mortality in 953 patients with stage III colon cancer. Compared to non-coffee drinkers, patients consuming four or more cups of coffee per day had a HR of 0.58 for colon cancer recurrence or mortality (Guercio et al., 2015).
Breast Cancer
Breast cancer is the second most commonly diagnosed cancer while it is the fourth leading cause of cancer death in Australia in 2014 (Cancer Australia, 2017). In the last decade, there were numerous studies carried out trying to link coffee consumption to the risk of developing breast cancer. Similar to the situation of liver cancer, the association between coffee and the risk of cancer was not well established a decade ago due to inconclusive findings among epidemiological studies. However, more studies conducted recently illustrated there was an inverse relationship between coffee consumption and the development certain type of breast cancer. A major mechanism of this is that antioxidant, mainly caffeic acid and caffeine, has the ability to inhibit DNA methylation in breast cancer cells (Gierach et al., 2012). This was supported by a clinical research based on live breast cancer cell culture, where the inhibitory effects of caffeine and caffeic acid on breast cancer cell growth was evident (Rosendahl et al., 2015).
Ganmaa et al. (2008) evaluated coffee consumption and risk of breast cancer in 85,987 female participants for 22 years, where follow up took place every two to four years. This long term and large scale study showed a significant inverse relationship between coffee intake and breast cancers in postmenopausal women. In addition, a Swedish study demonstrated that increased coffee consumption was associated in a reduced risk in breast cancer. Heavy coffee drinkers (more than five cups a day) has a significant lower risk in developing non-hormone-responsive type of breast cancer, known as estrogen receptor negative (ER-) breast cancer, than light coffee drinkers (Li et al., 2011). Similarly, a case-control study including 3062 cases and 3427 controls illustrated a remarkable reduction in risk in individuals who consumed more than five cups of coffee per day compared to non-drinkers. Furthermore, this study also suggested a high coffee intake was associated with reduced risk of ER- and postmenopausal breast cancer (Lowcock et al., 2013).
Kotsopoulos et al. (2007) also reported a strong inverse relationship between coffee intake and breast cancer risk for BRCA1 mutation carriers. A Swedish study assessed 634 tamoxifen-treated breast cancer patients through questionnaires and reviewing clinical reports demonstrated moderate (2-4 cups per day) to high (more than 5 cups per day) coffee consumption was associated with significantly reduced risk in developing breast cancer (Simonsson et al., 2013).
Furthermore, two more studies conducted in 2015 indicated the association of coffee consumption with more types of breast cancer. Oh et al. (2015) studied 42,009 subjects aged 30–49 years found an inverse association between coffee intake with the risk of overall and estrogen receptor negative and progesterone receptor negative (ER+ PR-) breast cancer. Statistically, relative risk was reported to be 0.87 and 0.81 for subjects with daily consumption of three to four cups and more than five cups respectively, compared to daily consumption of one to two cups. Similarly, a questionnaire based study assessed dietary intake of 335,060 women and depicted a decreased risk of breast cancer development with increased coffee intake in estrogen and progesterone receptor negative (ER-PR-) and postmenopausal breast cancer. In particular, the risk of ER-PR- breast cancer was lower by 4% for every 100 ml increase in coffee intake (Bhoo-Pathy et al., 2015).
Prostate Cancer
Prostate cancer was the most commonly diagnosed cancer in Australia in 2013 and the third most common cause of cancer deaths in Australia in 2014 (Cancer Australia, 2017). Although the investigation between coffee consumption and risk of prostate cancer was started since 1960s, the association in between remained inconclusive. The possible protective effect of coffee could be due to the antioxidant activity against oxidative stress and inhibition of DNA methylation or other biological activity of antioxidants (Butt & Sultan, 2011).
A Japanese population based study used self-administered questionnaire to assess the association between coffee intake and risk of prostate cancer in 18,853 subjects. A significant inverse relationship was reported where coffee consumers had HR of 0.81 (occasion drinker), 0.73 (one to two cups per day) and 0.63 (more than three cups a day) compared to non-coffee consumers (Li et al., 2013). In a Health Professional Follow-up Study, 47,911 men who took part in the study reported their level coffee intake every four years, for duration of twenty years. Results indicated regular and heavy coffee drinkers (six or more cups per day) had a lower adjusted relative risk for overall prostate cancer compared with nondrinkers, given that RR = 0.82. The association was more remarkable for lethal prostate cancer, where regular and heavy drinkers had the relative risk of 0.40 (Wilson et al., 2011). However, this was not in agreement with the case-control study conducted by Geybels, Neuhouser & Stanford (2013), which illustrated the non-association between coffee consumption and risk of overall prostate cancer. A health study involved 288,391 subjects demonstrated a non-statistical significant inverse association between coffee consumption and the risk of either overall, advanced, or fatal prostate cancer (Bosire et al., 2013). Similarly, epidemiological studies carried out by Nilsson et al. (2010), Ganesh et al. (2011) and Arab et al. (2012) reported no significant relation between coffee intake and risk of prostate cancer.
While the result of studies remained inconclusive, two recently conducted in vitro and in vitro studies provided another insight into this field. Kolberg et al. (2016) explored whether coffee constituent can modify NF-κB activity in human prostate cancer cell line (PC3). In particular, nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB) is a protein complex that plays an important role in regulating cellular signaling pathway involved in chronic inflammation. Results indicated coffee can reduced NF-κB activity up to 66% in PC3 compared to control cells. Additionally, this study also conducted in vivo imaging on xenograft mice to examine NF-κB activity. The mice were divided into coffee group and control group where all animals were given a western diet ad libitumwhile coffee and water was given to the two groups respectively. A significant 31.3% lower NF-κB activity in the xenografts of the coffee group compared with the control group was observed. Moreover, another in vitro study explored the potential anti-proliferative and anti-metastatic activity of caffeine on human prostate cancer cell lines, PC3 and DU145. Both types of cell culture treated with caffeine exhibited a significant reduction in their proliferative and metastatic behaviours in a dose and time dependent manner (Pounis et al., 2017).
Although there are new evidence suggesting the inverse relationship between coffee intake and the risk of prostate cancer, the limited number of study may not be adequate to conclude the association, given that several epidemiological studies in the last decade found no association between the two parameters.
Antioxidants and Type 2 Diabetes Mellitus
Diabetes mellitus is a chronic condition where the body does not produce any or enough insulin to control blood glucose level. It is a prevalent illness in many developed countries, including Australia. According to the report published by the Australian Bureau of Statistics, 4.4% of Australians suffered from Type 2 diabetes in 2014-2015, which is an increase from 3.8% in 2011-2012. In addition, although lack of physical activities and being obese pose an increased risk in developing diabetes, dietary habit and pattern also play an important role.
Similar to cancer, oxidative stress arises from insufficient antioxidant defense against ROS can lead to the development of Type 2 diabetes. Also, elevated blood glucose level due to impaired glucose uptake ability by adipose and peripheral tissue can contributes to the development of hyperglycemia, which is a direct risk factor to Type 2 diabetes (Manders et al., 2009). Coffee consumption has been found to have a negative correlation with incidence of diabetes, mainly due to its rich antioxidant profile. Despite the typical ROS scavenging activity of antioxidants, other biological activities of antioxidants has contributed to the preventative mechanism of coffee consumption in developing diabetes.
Antioxidant activity of coffee was examined by Chu et al. (2011) by conducting cellular antioxidant activity (CAA) assay. In particular, this cell-based assay measures an antioxidant’s capability to protect cell from oxidative damage by the alkylperoxyl radical, which is a common contributor of oxidative stress. Interestingly, despite the different antioxidant content in coffee, this study found that regular and decaffeinated coffee had a similar CAA value. On the other hand, Chu et al. (2011) also investigated the effect of antioxidant on pro-inflammatory cellular signaling pathway. It was suggested that continuation of NF-κB activation can lead to reduced insulin sensitivity (Zhang et al., 2009). Nevertheless, based on the experiment on cultured cell, it was shown that chlorogenic acid exhibits a strong ability in inhibiting this protein complex, thus has a positive effect on preventing diabetes (Chu et al., 2011).
Moreover, coffee and its constituent are known to have an impact on glucose metabolism, which may contribute to their anti-diabetic potential. Chu et al. (2011) studied the effect of coffee on glucose uptake in cultures of human subcutaneous adipocytes. This demonstrated that coffee, either regular or decaffeinated, can increased glucose uptake by adipocytes by at least two fold compared to the non-treated control cells. Alonso-Castro et al. (2008) explored and compared the ability of CGA and rosiglitazone, a commonly used anti-diabetic drug, in stimulating glucose uptake in murine adipocytes. Results indicated CGA is a potent stimulator of glucose uptake in both insulin sensitive and insulin resistant adipocytes, with the potency comparable to rosiglitazone. In addition, there are recent evidence showing CGA also plays a key role in improving glucose tolerance and insulin resistance. Liang et al. (2013) investigated the effect of CGA against insulin resistance in mice. Thirty mice were divided into three groups where all groups are assessable to normal diet and water. The control, model and CGA interference groups received saline, high fat emulsion and the combination of high fat emulsion and CGA (20mg per kilogram body weight) through gastric perfusion respectively. Results show the CGA interference group mice had better glucose tolerance and higher insulin sensitivity index compared to the other two groups.
Additionally, protective mechanisms in preventing Type 2 diabetes given by coffee consumption are also associated with other biological activities of antioxidants. Despite the activities of chlorogenic acid aforementioned, it was also demonstrated that CGA can inhibit glucose-6-phosphatase to delay glucose absorption, stimulate insulin secretion and reduce the postprandial blood glucose concentration (Zheng et al., 2007; Tousch et al., 2008; Akash, Rehman & Chen, 2014). Furthermore, caffeine was also showed to improve glucose tolerance, insulin sensitivity and stimulate insulin secretion from beta-cells of pancreatic islets (Akash, Rehman & Chen, 2014).
Based on the well-studied anti-diuretic activities of antioxidants, several animal and epidemiological studies were conducted to illustrate the relationship between coffee intake and the risk of developing Type 2 diabetes. A study showed coffee intake was inversely associated with the risk of diabetes mellitus in a dose-response manner (Ding et al., 2014). Comparing to individuals that did not consume coffee in a regular basis, the relative risk of diabetes were 0.92, 0.85, 0.79, 0.75, 0.71 and 0.67 for individuals who consumed one to six cups per day, respectively. The consumption of six cups of coffee per day was also demonstrated to have a 33% lower risk of type 2 diabetes. On the other hand, adiponectin is a hormone responsible for regulating catabolism of glucose and insulin sensitivity, however, adiponectin levels are reduced in diabetics, thus higher levels of adiponectin is considered as protective against diabetes (Ziemke & Mantzoros, 2010). Imatoh et al. (2011) conducted an epidemiological study to investigate the association between coffee consumption and adiponectin level in Japanese males with an aid of coffee consumption and frequency questionnaires. Results indicated habitual coffee consumption is associated with higher adiponectin levels in in subjects while a dose-dependent association between the two parameters was observed. A clinical study also demonstrated coffee consumption increases serum concentration of adiponectin through analysing blood samples of habitual coffee drinkers. Statistically, individuals who consumed eight cups of coffee per day have an 8% increased concentration of adiponectin in serum compared to non-coffee drinkers (Kempf et al., 2010). Nevertheless, Rustenbeck et al. (2014) studied the effect of coffee intake on glucose tolerance in induced Type 2 diabetic mice over 35 weeks. This research suggested coffee consumption improved glucose tolerance in diabetic mice, which again prove the preventative effect of coffee on Type 2 diabetes.
Limitations and Further Research Direction
A major limitation in relating antioxidants to health conditions is the lack of information regarding the type of coffee. Methods of brewing, degree of roasting coffee beans, size of cups and strength of coffee can varies among countries to a significant extent, thus the antioxidant content in the coffee may not be consistent. Also, most studies in this field are epidemiological based. Although many researchers based their study in large population to draw representative and reliable conclusions, questionnaires or self-reported data are widely used and there could be possible errors due to misreporting, under or over-reporting by the participating subjects. Furthermore, in vitro and in vivo studies are very rare in terms of the actual action of antioxidants on human cells. Therefore, further research is recommended to base on current evidence and findings that proven the protective effect of antioxidant to design experiments on cellular or human models.
Conclusion
This review summarizes current findings regarding the potential health benefits brought by antioxidants of coffee. There are strong epidemiological evidence indicating the benefits of antioxidants in coffee to the decreased risk of liver, colon and certain types of breast cancer. There are new evidence suggesting the inverse relationship between coffee intake and the risk of prostate cancer, yet the limited number of studies may not be adequate to conclude the association. Nevertheless, several animal and epidemiological studies illustrated the protective effective effect of coffee antioxidants in preventing type 2 diabetes mellitus. On the other hand, further in vitro and in vivo studies are recommended in order to better understand the action and protective effect of antioxidants in coffee.
Reference
Akash, M., Rehman, K. and Chen, S. (2014). Effects of coffee on type 2 diabetes mellitus. Nutrition, 30(7-8), pp.755-763.
Alonso-Castro, A., Miranda-Torres, A., González-Chávez, M. and Salazar-Olivo, L. (2008). Cecropia obtusifolia Bertol and its active compound, chlorogenic acid, stimulate 2-NBDglucose uptake in both insulin-sensitive and insulin-resistant 3T3 adipocytes. Journal of Ethnopharmacology, 120(3), pp.458-464.
Antol, M. (2002). Confessions of a coffee bean. 1st ed. Garden City Park, N.Y.: Square One Publishers, pp.64-70.
Arab, L., Su, L., Steck, S., Ang, A., Fontham, E., Bensen, J. and Mohler, J. (2012). Coffee Consumption and Prostate Cancer Aggressiveness Among African and Caucasian Americans in a Population-Based Study. Nutrition and Cancer, 64(5), pp.637-642.
Australian Beverages. (2013). Caffeine – The Facts. [online] Available at: http://www.australianbeverages.org/for-consumers/caffeine-facts/ [Accessed 23 Apr. 2017].
Australian Bureau of Statistics. (2014). 4364.0.55.007 – Australian Health Survey: Nutrition First Results – Foods and Nutrients, 2011-12. [online] Available at: http://www.abs.gov.au/ausstats/abs@.nsf/Lookup/by%20Subject/4364.0.55.007~2011-12~Main%20Features~Non-alcoholic%20beverages~701 [Accessed 19 Apr. 2017].
Australian Bureau of Statistics. (2015). 4364.0.55.001 – National Health Survey: First Results, 2014-15. [online] Available at: http://www.abs.gov.au/ausstats/abs@.nsf/Lookup/by%20Subject/4364.0.55.001~2014-15~Main%20Features~Diabetes%20mellitus~12 [Accessed 22 Apr. 2017].
Bagchi, D., Moriyama, H. and Swaroop, A. (2016). Green coffee bean extract in human health. 1st ed. Boca Raton: CRC Press.
Bakuradze, T., Lang, R., Hofmann, T., Stiebitz, H., Bytof, G., Lantz, I., Baum, M., Eisenbrand, G. and Janzowski, C. (2010). Antioxidant effectiveness of coffee extracts and selected constituents in cell-free systems and human colon cell lines. Molecular Nutrition & Food Research, 54(12), pp.1734-1743.
Bhoo-Pathy, N., Peeters, P. H., Uiterwaal, C. S., Bueno-de-Mesquita, H. B., Bulgiba, A. M., Bech, B. H. & Fagherazzi, G. (2015). Coffee and tea consumption and risk of pre-and postmenopausal breast cancer in the European Prospective Investigation into Cancer and Nutrition (EPIC) cohort study. Breast Cancer Research, 17(1), 15.
Bosire, C., Stampfer, M., Subar, A., Wilson, K., Park, Y. and Sinha, R. (2013). Coffee consumption and the risk of overall and fatal prostate cancer in the NIH-AARP Diet and Health Study. Cancer Causes & Control, 24(8), pp.1527-1534.
Bowden, J. (2007). The 150 healthiest foods on earth. 1st ed. Gloucester, Mass.: Fair Winds Press, pp.250-252.
Bravo, J., Arbillaga, L., de Peña, M. and Cid, C. (2013). Antioxidant and genoprotective effects of spent coffee extracts in human cells.
Butt, M. and Sultan, M. (2011). Coffee and its Consumption: Benefits and Risks. Critical Reviews in Food Science and Nutrition, 51(4), pp.363-373.
Cancer Australia. (2017). Breast cancer statistics | Cancer Australia. [online] Available at: https://canceraustralia.gov.au/affected-cancer/cancer-types/breast-cancer/breast-cancer-statistics [Accessed 22 Apr. 2017].
Cancer Australia (2017). Bowel cancer statistics | Bowel Cancer. [online] Available at: https://bowel-cancer.canceraustralia.gov.au/statistics [Accessed 29 Apr. 2017].
Cancer Australia (2017). Liver cancer statistics | Cancer Australia. [online] Available at: https://canceraustralia.gov.au/affected-cancer/cancer-types/liver-cancer/liver-cancer-statistics [Accessed 28 Apr. 2017].
Cancer Australia (2017). Prostate cancer statistics | Prostate Cancer. [online] Available at: https://prostate-cancer.canceraustralia.gov.au/statistics [Accessed 14 May 2017].
Chu, Y. (2012). Coffee: Emerging Health Effects and Disease Prevention. 1st ed. Ames, Iowa: IFT Press, pp.36-37.
Chu, Y., Chen, Y., Black, R., Brown, P., Lyle, B., Liu, R. and Ou, B. (2011). Type 2 diabetes-related bioactivities of coffee: Assessment of antioxidant activity, NF-κB inhibition, and stimulation of glucose uptake. Food Chemistry, 124(3), pp.914-920.
Clifford, M. (1985). Coffee: Botany, Biochemistry and Production of Beans and Beverage. 1st ed. The United States: The AVI Publishing Company, p.340.
Ding, M., Bhupathiraju, S., Chen, M., van Dam, R. and Hu, F. (2014). Caffeinated and Decaffeinated Coffee Consumption and Risk of Type 2 Diabetes: A Systematic Review and a Dose-Response Meta-analysis. Diabetes Care, 37(2), pp.569-586.
Frost-Meyer, N. and Logomarsino, J. (2012). Impact of coffee components on inflammatory markers: A review. Journal of Functional Foods, 4(4), pp.819-830.
Gierach GL, et al. (2012) Coffee intake and breast cancer risk in the NIH-AARP diet and health study cohort. Int J Cancer, 131(2), pp.452-460.
Ganesh, B., Sarade, M., Saoba, S. and Pinjari, S. (2011). Risk factors for prostate cancer: An hospital-based case-control study from Mumbai, India. Indian Journal of Urology, 27(3), p.345.
Ganmaa, D., Willett, W. C., Li, T. Y., Feskanich, D., van Dam, R.M., Lopez-Garcia, E., Hunter, D. J. and Holmes, M. D. (2008). Coffee, tea, caffeine and risk of breast cancer: A 22-year follow-up. Int. J. Cancer., 122, pp.2071–2076.
Geybels, M., Neuhouser, M. and Stanford, J. (2013). Associations of tea and coffee consumption with prostate cancer risk. Cancer Causes & Control, 24(5), pp.941-948.
Guercio, B., Sato, K., Niedzwiecki, D., Ye, X., Saltz, L., Mayer, R., Mowat, R., Whittom, R., Hantel, A., Benson, A., Atienza, D., Messino, M., Kindler, H., Venook, A., Hu, F., Ogino, S., Wu, K., Willett, W., Giovannucci, E., Meyerhardt, J. and Fuchs, C. (2015). Coffee Intake, Recurrence, and Mortality in Stage III Colon Cancer: Results From CALGB 89803 (Alliance). Journal of Clinical Oncology, 33(31), pp.3598-3607.
Heckman, M., Weil, J. and de Mejia, E. (2010). Caffeine (1, 3, 7-trimethylxanthine) in Foods: A Comprehensive Review on Consumption, Functionality, Safety, and Regulatory Matters. Journal of Food Science, 75(3), pp.R77-R87.
Herrera, E., Jiménez, R., Aruoma, O., Hercberg, S., Sánchez-García, I. and Fraga, C. (2009). Aspects of antioxidant foods and supplements in health and disease. Nutrition Reviews, 67, pp.S140-S144.
Higdon, J. and Frei, B. (2006). Coffee and Health: A Review of Recent Human Research. Critical Reviews in Food Science and Nutrition, 46(2), pp.101-123.
Hoelzl, C., Knasmüller, S., Wagner, K., Elbling, L., Huber, W., Kager, N., Ferk, F., Ehrlich, V., Nersesyan, A., Neubauer, O., Desmarchelier, A., Marin-Kuan, M., Delatour, T., Verguet, C., Bezençon, C., Besson, A., Grathwohl, D., Simic, T., Kundi, M., Schilter, B. and Cavin, C. (2010). Instant coffee with high chlorogenic acid levels protects humans against oxidative damage of macromolecules. Molecular Nutrition & Food Research, 54(12), pp.1722-1733.
Hou, N., Liu, N., Han, J., Yan, Y. and Li, J. (2017). Chlorogenic acid induces reactive oxygen species generation and inhibits the viability of human colon cancer cells. Anti-Cancer Drugs, 28(1), pp.59-65.
Hu, G., Tuomilehto, J., Pukkala, E., Hakulinen, T., Antikainen, R., Vartiainen, E. and Jousilahti, P. (2008). Joint effects of coffee consumption and serum gamma‐glutamyltransferase on the risk of liver cancer. Hepatology, 48(1), pp.129-136.
Huang, D., Ou, B. and Prior, R. (2005). The Chemistry behind Antioxidant Capacity Assays. Journal of Agricultural and Food Chemistry, 53(6), pp.1841-1856.
Imatoh, T., Tanihara, S., Miyazaki, M., Momose, Y., Uryu, Y. and Une, H. (2011). Coffee consumption but not green tea consumption is associated with adiponectin levels in Japanese males. European Journal of Nutrition, 50(4), pp.279-284.
Inoue, M., Kurahashi, N., Iwasaki, M., Shimazu, T., Tanaka, Y., Mizokami, M. and Tsugane, S. (2009). Effect of Coffee and Green Tea Consumption on the Risk of Liver Cancer: Cohort Analysis by Hepatitis Virus Infection Status. Cancer Epidemiology Biomarkers & Prevention, 18(6), pp.1746-1753.
Johnson, S., Koh, W., Wang, R., Govindarajan, S., Yu, M. and Yuan, J. (2011). Coffee consumption and reduced risk of hepatocellular carcinoma: findings from the Singapore Chinese Health Study. Cancer Causes & Control, 22(3), pp.503-510.
Kempf, K., Herder, C., Erlund, I., Kolb, H., Martin, S., Carstensen, M., Koenig, W., Sundvall, J., Bidel, S., Kuha, S. and Jaakko, T. (2010). Effects of coffee consumption on subclinical inflammation and other risk factors for type 2 diabetes: a clinical trial. American Journal of Clinical Nutrition, 91(4), pp.950-957.
Kolberg, M., Pedersen, S., Mitake, M., Holm, K., Bøhn, S., Blomhoff, H., Carlsen, H., Blomhoff, R. and Paur, I. (2016). Coffee inhibits nuclear factor-kappa B in prostate cancer cells and xenografts. The Journal of Nutritional Biochemistry, 27, pp.153-163.
Kotsopoulos, J., Ghadirian, P., El-Sohemy, A., Lynch, H., Snyder, C., Daly, M., Domchek, S., Randall, S., Karlan, B., Zhang, P., Zhang, S., Sun, P. and Narod, S. (2007). The CYP1A2 Genotype Modifies the Association Between Coffee Consumption and Breast Cancer Risk Among BRCA1 Mutation Carriers. Cancer Epidemiology Biomarkers & Prevention, 16(5), pp.912-916.
Lai, G., Weinstein, S., Albanes, D., Taylor, P., McGlynn, K., Virtamo, J., Sinha, R. and Freedman, N. (2013). The association of coffee intake with liver cancer incidence and chronic liver disease mortality in male smokers. British Journal of Cancer, 109(5), pp.1344-1351.
Lee, W. (2006). Inhibition of DNA methylation by caffeic acid and chlorogenic acid, two common catechol-containing coffee polyphenols. Carcinogenesis, 27(2), pp.269-277.
Li, J., Seibold, P., Chang-Claude, J., Flesch-Janys, D., Liu, J., Czene, K., Humphreys, K. and Hall, P. (2011). Coffee consumption modifies risk of estrogen-receptor negative breast cancer. Breast Cancer Research, 13(3).
Li, Q., Kakizaki, M., Sugawara, Y., Tomata, Y., Watanabe, T., Nishino, Y. and Tsuji, I. (2013). Coffee consumption and the risk of prostate cancer: the Ohsaki Cohort Study. British Journal of Cancer, 108(11), pp.2381-2389.
Liang, X., Zhong, Y., Meng, W. and Wang, Z. (2013). Effects of chlorogenic acid on mouse insulin resistance development induced by high fat emulsion. Chinese Pharmacological Bulletin, 29(5), pp.654–658.
Lodish, H., Berk, A. and Zipursky, S. (2000). Molecular Cell Biology. 4th edition. 4th ed. New York: W. H. Freeman.
Lowcock, E., Cotterchio, M., Anderson, L., Boucher, B. and El-Sohemy, A. (2013). High Coffee Intake, but Not Caffeine, is Associated with Reduced Estrogen Receptor Negative and Postmenopausal Breast Cancer Risk with No Effect Modification by CYP1A2 Genotype. Nutrition and Cancer, 65(3), pp.398-409.
Ludwig, I., Clifford, M., Lean, M., Ashihara, H. and Crozier, A. (2014). Coffee: biochemistry and potential impact on health. Food & Function, 5(8), pp.1695-1709.
Manders, R., Pennings, B., Beckers, C., Aipassa, T. and van Loon, L. (2009). Prevalence of daily hyperglycemia in obese type 2 diabetic men compared with that in lean and obese normoglycemic men: effect of consumption of a sucrose-containing beverage. American Journal of Clinical Nutrition, 90(3), pp.511-518.
Meng, S., Cao, J., Feng, Q., Peng, J. and Hu, Y. (2013). Roles of Chlorogenic Acid on Regulating Glucose and Lipids Metabolism: A Review. Evidence-Based Complementary and Alternative Medicine, 2013, pp.1-11.
Montella, M., Polesel, J., La Vecchia, C., Maso, L., Crispo, A., Crovatto, M., Casarin, P., Izzo, F., Tommasi, L., Talamini, R. and Franceschi, S. (2007). Coffee and tea consumption and risk of hepatocellular carcinoma in Italy. International Journal of Cancer, 120(7), pp.1555-1559.
National Cancer Institute. (2015). What Is Cancer?. [online] Available at: https://www.cancer.gov/about-cancer/understanding/what-is-cancer [Accessed 28 Apr. 2017].
Nilsson, L., Johansson, I., Lenner, P., Lindahl, B. and Van Guelpen, B. (2010). Consumption of filtered and boiled coffee and the risk of incident cancer: a prospective cohort study. Cancer Causes & Control, 21(10), pp.1533-1544.
Nkondjock, A. (2009). Coffee consumption and the risk of cancer: An overview. Cancer Letters, 2(277), pp.121-125.
Oh, J., Sandin, S., Ström, P., Löf, M., Adami, H. and Weiderpass, E. (2015). International Journal of Cancer, 8(137), pp.1979–1989.
Ohishi, W., Fujiwara, S., Cologne, J., Suzuki, G., Akahoshi, M., Nishi, N., Takahashi, I. and Chayama, K. (2008). Risk Factors for Hepatocellular Carcinoma in a Japanese Population: A Nested Case-Control Study. Cancer Epidemiology Biomarkers & Prevention, 17(4), pp.846-854.
Pérez-Jiménez, J., Neveu, V., Vos, F. and Scalbert, A. (2010). Identification of the 100 richest dietary sources of polyphenols: an application of the Phenol-Explorer database. European Journal of Clinical Nutrition, 64, pp.S112-S120.
Perez-Jimenez, J., Fezeu, L., Touvier, M., Arnault, N., Manach, C., Hercberg, S., Galan, P. and Scalbert, A. (2011). Dietary intake of 337 polyphenols in French adults. American Journal of Clinical Nutrition, 93(6), pp.1220-1228.
Peterson, S., Yuan, J., Koh, W., Sun, C., Wang, R., Turesky, R. and Yu, M. (2009). Coffee Intake and Risk of Colorectal Cancer Among Chinese in Singapore: The Singapore Chinese Health Study. Nutrition and Cancer, 62(1), pp.21-29.
Pounis, G., Tabolacci, C., Costanzo, S., Cordella, M., Bonaccio, M., Rago, L., D’Arcangelo, D., Filippo Di Castelnuovo, A., de Gaetano, G., Donati, M., Iacoviello, L. and Facchiano, F. (2017). Reduction by coffee consumption of prostate cancer risk: Evidence from the Moli-sani cohort and cellular models. International Journal of Cancer, 141(1), pp.72-82.
Preedy, V. (2013). Tea in health and disease prevention. 1st ed. Amsterdam: Elsevier/Academic Press, pp.1548-1549.
Preedy, V. (2014). Coffee in health and disease prevention. 1st ed, pp.493-494.
Rosendahl, A., Perks, C., Zeng, L., Markkula, A., Simonsson, M., Rose, C., Ingvar, C., Holly, J. and Jernstrom, H. (2015). Caffeine and Caffeic Acid Inhibit Growth and Modify Estrogen Receptor and Insulin-like Growth Factor I Receptor Levels in Human Breast Cancer. Clinical Cancer Research, 21(8), pp.1877-1887.
Rustenbeck, I., Lier-Glaubitz, V., Willenborg, M., Eggert, F., Engelhardt, U. and Jörns, A. (2014). Effect of chronic coffee consumption on weight gain and glycaemia in a mouse model of obesity and type 2 diabetes. Nutrition & Diabetes, 4(6), pp.123.
Shahidi, F. and Naczk, M. (2004). Phenolics in food and nutraceuticals. 1st ed. Boca Raton, Fla: CRC, pp.333-334.
Shearer, J., Farah, A., de Paulis, T., Bracy, D. P., Pencek, R. R., Graham, T. E., & Wasserman, D. H. (2003). Quinides of roasted coffee enhance insulin action in conscious rats. The Journal of nutrition, 133(11), pp.3529-3532.
Simonsson, M., Söderlind, V., Henningson, M., Hjertberg, M., Rose, C., Ingvar, C. and Jernström, H. (2013). Coffee prevents early events in tamoxifen-treated breast cancer patients and modulates hormone receptor status. Cancer Causes & Control, 24(5), pp.929-940.
Sinha, R., Cross, A., Daniel, C., Graubard, B., Wu, J., Hollenbeck, A., Gunter, M., Park, Y. and Freedman, N. (2012). Caffeinated and decaffeinated coffee and tea intakes and risk of colorectal cancer in a large prospective study. American Journal of Clinical Nutrition, 96(2), pp.374-381.
Siti, H., Kamisah, Y. and Kamsiah, J. (2015). The role of oxidative stress, antioxidants and vascular inflammation in cardiovascular disease (a review). Vascular Pharmacology, 71, pp.40-56.
Sugiyama, K., Kuriyama, S., Akhter, M., Kakizaki, M., Nakaya, N., Ohmori-Matsuda, K., Shimazu, T., Nagai, M., Sugawara, Y., Hozawa, A., Fukao, A. and Tsuji, I. (2010). Coffee Consumption and Mortality Due to All Causes, Cardiovascular Disease, and Cancer in Japanese Women. Journal of Nutrition, 140(5), pp.1007-1013.
Talwar, G., Hasnain, S. and Sarin, S. (2016). Textbook of biochemistry, biotechnology, allied and molecular medicine. 1st ed. Prentice-Hall Of India, pp.547-551.
Tousch, D., Lajoix, A., Hosy, E., Azay-Milhau, J., Ferrare, K., Jahannault, C., Cros, G. and Petit, P. (2008). Chicoric acid, a new compound able to enhance insulin release and glucose uptake. Biochemical and Biophysical Research Communications, 377(1), pp.131-135.
Trevitt, J., Kawa, K., Jalali, A. and Larsen, C. (2009). Differential effects of adenosine antagonists in two models of parkinsonian tremor. Pharmacology Biochemistry and Behavior, 94(1), pp.24-29.
Vucic, E., Brown, C. and Lam, W. (2008). Epigenetics of cancer progression. Pharmacogenomics, 9(2), pp.215-234.
Wakai, K., Kurozawa, Y., Shibata, A., Fujita, Y., Kotani, K., Ogimoto, I., Naito, M., Nishio, K., Suzuki, H., Yoshimura, T. and Tamakoshi, A. (2007). Liver cancer risk, coffee, and hepatitis C virus infection: a nested case–control study in Japan. British Journal of Cancer, 97(3), pp.426-428.
Wang, Z. J., Ohnaka, K., Morita, M., Toyomura, K., Kono, S., Ueki, T., Tanaka, M., Kakeji, Y., Maehara, Y., Okamura, T., Ikejiri, K., Futami, K., Maekawa, T., Yasunami, Y., Takenaka, K., Ichimiya, H., Terasaka, R., and Ikejiri, K. (2013). Dietary polyphenols and colorectal cancer risk: the Fukuoka colorectal cancer study. World J Gastroenterology, 19(17), pp.2683-90.
Watson, R., Preedy, V. and Zibadi, S. (2014). Polyphenols in human health and disease. 1st ed. The United States of America: Academic press, pp.571-573.
Wilson, K., Kasperzyk, J., Rider, J., Kenfield, S., van Dam, R., Stampfer, M., Giovannucci, E. and Mucci, L. (2011). Coffee Consumption and Prostate Cancer Risk and Progression in the Health Professionals Follow-up Study. JNCI Journal of the National Cancer Institute, 103(11), pp.876-884.
World Cancer Research Fund. (2007). Food, Nutrition, Physical Activity and the Prevention of Cancer: A Global Perspective. AICR, Washington, DC.
Zampelas, A., & Micha, R. (Eds.). (2015). Antioxidants in health and disease. CRC Press, pp.89-90.
Zhang, J., Wu, W., Li, D., Guo, Y. and Ding, H. (2009). Overactivation of NF-κB impairs insulin sensitivity and mediates palmitate-induced insulin resistance in C2C12 skeletal muscle cells. Endocrine, 37(1), pp.157-166.
Zheng, Y., Liu, K. and Jia, G. (2007). Effect of a Hot-water Extract from Coffee Beans on the Postprandial Blood Glucose Concentration in Rats. Chinese Pharmaceutical Journal, 42(1), pp.32-35.
Ziemke, F. and Mantzoros, C. (2010). Adiponectin in insulin resistance: lessons from translational research. American Journal of Clinical Nutrition, 91(1), pp.258S-261S.
Zujko, M., Witkowska, A., Waśkiewicz, A. and Sygnowska, E. (2012). Estimation of dietary intake and patterns of polyphenol consumption in Polish adult population. Advances in Medical Sciences, 57(2), pp.375-384.
Cite This Work
To export a reference to this article please select a referencing stye below:
Related Services
View all


Related Content
All TagsContent relating to: "Food and Nutrition"
Food and Nutrition studies deal with the food necessary for health and growth, the different components of food, and interpreting how nutrients and other food substances affect health and wellbeing.
Related Articles

DMCA / Removal Request
If you are the original writer of this literature review and no longer wish to have your work published on the UKDiss.com website then please: