Assessment of the Structural Quality of Primary Health Care Centres in Obio-Akpor
Info: 11551 words (46 pages) Example Dissertation Proposal
Published: 27th Oct 2021
Tagged: HealthHealthcare
TABLE OF CONTENTS
BACKGROUND…………………………………………………………………………3
RATIONALE FOR SETTING STANDARDS/CONCEPT OF QUALITY………7
STATEMENT OF PROBLEM……………………………………………………………8
JUSTIFICATION OF STUDY…………………………………………………………10
PUBLIC HEALTH BENEFITS…………………………………………………………..11
OBJECTIVES OF STUDY…………………………………………………………..11
RESEARCH QUESTIONS……………………………………………………………..12
MATERIALS AND METHODS………………………………………………………..13
CHAPTER ONE: INTRODUCTION
1.1 BACKGROUND
The preamble of the 1946 World Health Organization (WHO) constitution defines health as “a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity. The constitution defines the right to health as enjoyment of “the highest attainable standard of health”, and this is a fundamental right of every human being. The right to health includes: access to timely, acceptable and affordable health care of appropriate quality. [1]
Due to the widespread inequalities in health and health services all over the world and the growing realization of the need for an alternative approach to hospital-based and vertical approach to health services, methods of promoting the development of basic health services and alternative approaches to meeting basic health needs in developing countries were sought.[2]
In 1977 the World Health Assembly (WHA) specified that the “main target of government and WHO in the coming decades should be the attainment by all citizens of the world by the year 2000 a level of health that would make them live a socially and economically productive life” and so in 1978 the concept of Primary Health Care was developed at Alma- Ata.[3]
The essential elements for enhancing the health of the community as a whole are encompassed in the concept of Primary Health Care. It elaborates the need to improve the quality of health in the most rural settings by bringing health services as close as possible to the individuals and families in the community. The recognition and adoption of this method of health care delivery has greatly improved the outcome of the health status of rural communities.
Primary Health Care as conceptualised by the Alma-Ata declaration of 1978 is a grass-root approach towards universal and equitable health care for all.[4] The strategy is meant to address the main health problems in the community providing promotive, preventive, curative and rehabilitative services. [5]. It is defined as essential health care based on practical, scientifically-sound and socially-acceptable methods and technology made universally accessible to individuals and families in the community by means acceptable to them through their full participation and at a cost they can afford to maintain at every stage of their development in a spirit of self-reliance and self-determination.[6]
The ultimate goal of Primary Health Care is health for all. The World Health Organisation has identified five key elements to achieving this goal.
1. Reducing exclusion and social disparities in health (universal coverage forms).
2. Organising health services around people’s needs and expectations (service delivery reforms).
3. Integrating health into all sectors (public policy reforms).
4. Pursuing collaborative models of policy dialogue (leadership reforms)
5. Increasing stakeholder participation.[7]
As defined, primary health care spans seven important features which include:
1. It is an element of the health system: It forms an integral part of the country’s health system. It is the first level of contact of individuals, the family and community with the national health system, bringing health care as close as possible to where people live and work and constitutes the first element of a continuing health care process.
2. Focuses on priorities: It is essential health care
3. Scientific basis.
4. Culture sensitivity: Socially acceptable methods and technology.
5. Equity: It is made universally accessible to individuals and families in the community.
6. Community participation: Through their full participation
7. Sustainability and self-reliance: At a cost that the community and the country can afford to maintain at every stage of their development in a spirit of self-reliance and self-determination. [8]
The salient features are highlighted below:
The Primary Health Care concept is not intended to represent second best medicine only acceptable to the rural poor or the dwellers of urban slums. It is not a stop gap solution to be replaced by something better at a later stage; rather the Primary Health Care approach is intended to be a permanent feature of all health care services. The quality of care should steadily improve and at all times it should be appropriate to the resources and the needs of the community. Primary Health Care is not intended to function in isolation but in collaboration with the referral and specialist services. These various services should be mutually supportive.[9]
Primary Health Care as a level of care is a community-oriented care approach that should be structured in a way that it attends to a well-defined population with the use of epidemiology to determine the health needs of that population. Good collaboration with the community to identify priorities, resources and plan activities. A multidisciplinary cooperation to plan and carry out interventions, use of effective health information system, appropriate health teams, good management support and regular assessment of the outcome of the program.
The items that form the structure of Primary Health Care centres can be grouped into three:
- INFRASTRUCTURE: Essential infrastructure for a Primary Health Care facility according to the Minimum Standards for Primary Health Care facilities in Nigeria include: land with a minimum area of 4,200 square meters, a detached building with at least 13 rooms, clean water source, regular power supply, sanitary waste collection point and waste disposal site and staff accommodation within the premises. Also, there should be 2 consulting rooms, adolescent health servicing room, 2 delivery rooms, pharmacy/dispensing unit, laboratory, in-patient section, maternity/lying-in section, medical records area, procedure room, kitchen and toilets.[10]
- ORGANISATION: They are involved with overall direction and enable an environment for integrated Primary Health Care service delivery, planning and management of services, manpower development, resource mobilization and provision of an operational guideline. This is usually done by the Primary Health Care facility management committee.[11]
- SERVICE PROVISION: It includes availability and access to healthcare service, working hours (24-hour service) and staffing across all departments with the following recommended services such as: health education/promotion, health management information system, routine home visits and community outreach, maternal, new born and child care, family planning, immunization, essential drugs, water and sanitation, 2-way referral system, records maintenance, monitoring services, waste disposal, adolescent health services, laboratory services and promotion of proper nutrition/food education.[12]
1.2 RATIONALE FOR SETTING STANDARDS/CONCEPT OF QUALITY
According to the World Health Organisation, the purpose for setting health standards as a tool in health service management is to strive to achieve the highest quality of care possible within the resources available. [13] They provide the basis for monitoring, comparison, supervision, and regulation of the given services.[14]
In the health care industry, quality of life is more than a concept. It has become essential to patient well-being and financial survival according to Phill Buttel et al.
The most durable and widely cited definition of health care quality was formulated by the Institute of Medicine (IOM) in 1990. According to IOM, quality consists of the ‘degree’ to which health services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge.[15]
Campbell et all described the dimensions of quality in general practice as:
(a) Being a component of quality for individual patients by evaluating access, clinical effectiveness and inter-personal effectiveness.
(b) Additional components for the population which include equity and efficiency.
Patient’s evaluation of quality which is their views or judgements on aspects or entire care is one of other ways they can participate in health care delivery (Donabedian: Wensing & Elwing).
Structural and capacity analysis offers the advantage of at least dealing in part, with fairly concrete and accessible information. Structural or capacity assessment considers quality and quantity of health care resources and the organisation of these resources. [16]
1.3 STATEMENT OF PROBLEM
The Primary Health Care system should be able to resolve the health problems of at least 70% of the people compared to the less than 20% of the population that it currently attends to. [17]
The standard has not been obtainable due to several factors such as:
1. The high cost of service delivery in health centres limits the ability of the community to seek medical attention.
The concept of Primary Health Care is health service delivered to the community at a cost that they can afford. Due to poor funding of the Primary Health Care centres, the drug revolving fund was initiated with a cost recovery system and a recommended minimal mark-up (10% or any approved by the Honourable Commissioner for Health is added to the cost of the drugs). [18] This low level of public funding leads to an over-reliance on cost recovery mechanisms such as drug revolving funds which shifts the burden of financing healthcare onto the poor and results in a reduction of access for those who need it the most.[19]
2. Poor health worker performance including high absenteeism, low competence and low productivity.
This may be due to low level of supervision from levels above. Service Delivery Indicator (SDI) surveys show that 23% of facilities received supervision infrequently (9% received visits 1-2 times in a year or not at all, 14% received no visits at all)[20]. This has resulted in absence from duty posts from respective health service providers, lateness to work and a punctuated 24 hour service delivery. Nigeria produces a large number of Community Health Extension Workers (CHEW) and Junior Community Health Extension Workers (JCHEW) each year. Unfortunately many CHEWs are either unemployed or working in a private sector and the Primary Health Care system is not getting full value out of the investment the government of Nigeria makes in developing health workers, and even when CHEWs make it into the public sector, it is often the case that the CHEWs are found in the health facilities and do not spend enough time in community.[21] The standing order distributes their daily working time as follows: 60% in the facility and 40% in the community for Junior Community Health Extension Workers and 20% of their time in the community and 80% in the health facility for Senior Community Health Extension Workers.[22] According to Professor Eyitayo Lambo, low confidence of the population in Primary Health Care services has led to low utilization leading to the by-passing of Primary Health Care facilities to secondary and tertiary health care facilities. Also, many facilities do not offer comprehensive healthcare services and are not open 24/7.
3. Lack of infrastructure, drugs, equipment and vaccines at the facility level. There is general shortage of drugs and supplies available in the Primary Health Care system. Overall availability for vaccines (76%) is better than that for essential drugs (49%) but far from universally available. Only 20% of facilities have all the all required minimum equipment.[23]
1.4 JUSTIFICATION OF THE STUDY
Primary health Care system has contributed to some progress made in Nigeria’s health status indicators. Though the mortality decline has not been as rapid as expected in Nigeria. Daniel H. Kress used two indicators (infant mortality rate and under-five mortality rate) for cross validation and found that infant mortality has declined by 21% from 1990 to 2013, and under-five mortality declined by 34% over the same period.
Effective Primary Health Care plays a major role in the achievement of the Millennium Development Goals as relates to health and universal health coverage, most of the 13 targets of the 3rd Sustainable Development Goal (i.e., to ensure healthy lives and promote wellbeing for all at all ages) can contribute to many of the 16 other Sustainable Development Goals.[24]
In the recent World Bank rating one of the cottage hospitals in Rivers State, the Obio Cottage Hospital in Obio-Akpor Local Government Area, was rated as a model in health care delivery not only in Nigeria but the world at large. Out of concern for the high cost of health services especially in the oil-rich Niger-Delta communities under its 1A cluster, Shell Petroleum Development Company of Nigeria in collaboration with the Rivers state Government sought a more effective healthcare delivery for the people and residents of the 1A cluster and came up with Community Health Insurance Scheme (CHIS) and signed an operational memorandum of understanding. [25]
However, poverty limits accessibility to basic services like health. It influences negatively the ability to utilize modern health facilities, such limitations tend to cause high mortality especially among the poor (Audu 2009). Hence the need for the Primary Health Care to assess the average affordable cost for the community as described in community participation.
The quality of service delivered by the Primary Health Care centre greatly depends on the organisational structure of the facility as well as the standing order of events and method of supervision over the activities in addition to availability of essential infrastructure, drugs and supplies.
1.5 PUBLIC HEALTH BENEFITS
A study on the structural quality of Primary Health Care delivery in Obio-Akpor L.G.A would compare what is obtainable in the health care facilities with the recommended Minimum Standards for Operation and identify facilities that meet up with the several requirements while elucidating the pitfalls.
It would also highlight the gap between information and implementation of information and knowledge of the practicable methods for improving health care delivery.
1.6 OBJECTIVES OF STUDY
General Objective
To determine the structural quality of Primary Health Care facilities in Obio-Akpor Local Government Area according to the Minimum Standard for Primary Health Care in Nigeria.
Specific Objectives
- To assess the quality of the infrastructure in the Primary Health Care facilities in Obio-Akpor L.G.A, Rivers State.
- To assess the organisational structure of the Primary Health Care facilities in Obio-Akpor L.G.A, Rivers State.
- To assess the level of service delivery in the Primary Health Care facilities in Obio-Akpor L.G.A in comparison with the recommended minimum standards.
1.7 RESEARCH QUESTIONS
1.) Does the quality of infrastructure in the Primary Health Care centres in Obio-Akpor LGA meet up with the Minimum Standard for Primary Health Care centres in Nigeria?
2.) Does the organisational structure in the Primary Health Care centres in Obio-Akpor LGA meet up with the Minimum Standard for Primary Health Care centres in Nigeria?
3.) What is the quality of services provided by the Primary Health Care facilities in Obio-Akpor LGA?
4.) What is the quality and strength of the members staff in the Primary Health Care facilities in Obio-Akpor LGA, including the staff mix?
CHAPTER 2: LITERATURE REVIEW
The Alma-Ata declaration on Primary Health Care (PHC) which was made in 1978 is meant to address the main health problems in communities by providing promotive, preventive, curative and rehabilitative services. [26]
Primary health care as conceptualized by the Alma-Ata declaration of 1978 is a grass-root approach towards universal and equitable health care for all (World Health Organisation – United Nations Children Fund, WHO-UNICEF, 1978). [27]
According to Byrant, large numbers of the world’s people, perhaps more than half, have no access to health care at all, and for many of the rest, the care they receive doesn’t answer the problems they have.
Another important inspiration for primary health care was the global popularity that the massive expansion of rural medical services in communist China, experienced, especially the “bare foot doctors”.
This visibility coincided with China’s entrance into the UN (system) including the World Health Organisation. The bare foot doctors whose numbers increased dramatically between the early 1960s and cultural revolution (1964 -1976), where a diverse array of village health workers who lived in the community they served, stressed rural rather than urban health care and prevention rather than curative service, and combined western and traditional medicines.
The Alma-Ata declaration linked health and development. They saw health work was as part of a process of improving health condition. Primary health care was designed to be the new focus of the public health system.
This required cooperative approach and several institutions (public and private) working together on health issues (especially on health education, adequate housing, safe water and basic sanitation.
The 32nd World Health Assembly that took place in Geneva in 1979 endorsed the conference’s declaration. The assembly approved a resolution stating that primary health care was “the key to attaining an acceptable level of health for all”. However, despite the initial enthusiasm, it was difficult to implement primary health care after Alma-Ata. About a year after the conference took place, a different interpretation of primary health care appeared.
Concerned about the identification of the most cost-effective health strategies, the Rockefeller foundation sponsored in 1979, a small conference entitled “Health and Population in Development, at its Bellagio conference in Italy.
The conference was based on a published paper by Julia Walsh and Kenneth S. Waren entitled “Selective Primary Health Care, an Interim Strategy for Disease Control in Developing Countries.
The paper sought specific causes of death, paying special attention to the most common diseases of infants in developing countries such as diarrhoea and diseases produced by lack of immunization.
At first, the contents of its package were not completely clear. However, in the following years, these interventions were reduced to 4 and were best known as GOBI, which stood for growth monitoring, oral rehydration techniques, breastfeeding and immunization.
However, a debate between the 2 versions of primary health care was inevitable. Some supporters of complementary primary health care, as the holistic or original idea of primary health care began to be called, considered selective primary health care to be complementary of Alma-Ata declaration, while others thought of it as contradictory. [28]
Comprehensive primary health care was developed as a health plan with the aim to meet the needs of all the population beginning with some groups. [29] Its major focus is health through equity and community empowerment.
Inadequacies in the quality of child health services in primary health care facilities is a product of failures in a range of quality measures – structural (lack) of equipment and essential drugs ), process failure (non-use of national case management including management algorithm) and lack of a protocol of systematic supervision of health workers.
Primary health care facilities were adequately equipped to the extent of providing immunisation services and management of diarrhoea but not other aspects of care expected of a primary health care centre, including management of acute respiratory infections, a common problem in the region.
Supply of essential drugs was inadequate in all centres and facilities for emerging care were lacking. [30]
Most health-care systems in Africa are not designed from the ground up to respond to local health needs, but were either copied or adopted from colonialist governments (Kaseje, 2006; Ityavyar, 1987). Such health systems are inherently irresponsive to changing health needs of the adopting countries. For instance, the foundations of modern health systems in Nigeria (Ityavyar, 1987; Adeyemo, 2005), Tanzania (Kopoka, 2000), and Ghana (Baidoo, 2009) were the legacies of colonization and Christian missions [31]
The colonial healthcare model was not intended to develop a system from the ground up. The intent was to introduce European model of care that will replace whatever health system was available in Africa. [32]
Nigeria is one of the signatories to the Alma-Ata declaration of Primary Health care in 1978. But it is interesting to note that prior to the 1978 Alma-Ata declaration, the country had set the ball rolling with the implementation of the Basic Health Services Scheme (1975 – 1980), which was Nigeria’s first serious attempt at the implementation of Primary Health Care. This scheme concentrated on the provision of health facilities, training of health workers and paying little attention to community participation, intersectoral cooperation or use of local technology (Obionu, 2007). [33]
In 1988, the National health policy of Nigeria was launched and is seen as a collective will of the government and people of Nigeria to provide comprehensive health care system that is based on primary health care.
In 1992, Primary Health Care implementation started with the commencement of primary health care programmes in the Local Government Areas. Nigeria therefore became one the few countries in the developing world to have systematically decentralized the delivery of basic health services through local government administration. (Obionu, 2007; Cueto, 2005) [34]
According to the World Health Organization (2006), there is a shortage of 4.3 million doctors, nurses, midwives, and support staff worldwide, and that 36 of the 57 countries with severe shortages are in Africa. Also, Rawat (2012) identified shortage of health labour force as a major obstacle to prevention and treatment for the 5.7 million people currently living with HIV/AIDS in South Africa. [35]
Many of the health care workers (68.3%) have adequate training in immunisation and their knowledge cores on immunisation issues (62%) were higher than other aspects of primary health care.
Management of primary health care systems in less developed countries is often impeded by factors such as poorly trained personnel, limited financial resources and poor worker morale. [36]
Sub Saharan Africa, with about 11% of the world’s population bears over 24% of the global disease burden, is home to only 35% of the global workforce, and spends less than 1% of the world’s financial resources on health. In most developing countries, the health workforce is concentrated in the major towns and cities, while rural areas can only boast of about 23% and 38% of the countries doctors and nurses respectively. The imbalances exist not only in the total numbers and geographical distribution of health workers, but also in the skills mix of available health workers. [37]
A study in Ghana Dovlo (2005) observed that inadequate supply of basic equipments, lack of accommodation, especially for newly qualified skilled health professionals at start of work, and poor remuneration are some of the factors that force skilled health professionals, including nurses to leave the country.
This research also shows that Ghana loses many of its health professionals due to old age (Dovlo 2005, Donkor and Andrews, 2011). Those aged nurses are not economically motivated to continue in services if their skills are still needed because at retirement, their benefits, gratuity and pension paid to them are inadequate to meet their basic needs. [38]
A descriptive cross-sectional study done by A. S Mohammed, I. E Idowu, Y. A Kuyin in Ikoji Ejirim Local Council Development Area (LCDA) Lagos, which had 9 primary health care facilities catering for a population of about 100,000, showed that 77.8% had inadequate water and supply, 44.4% lacked basic equipment and none had a maintenance plan.
Ambulance service was available only in 11.1% of the facilities. Only 33% could be accessed easily by public transportation and only 22.7% of the facilities enjoy community participation in planning and management. It also showed that the workers comprised nurses/midwives (57.9%), senior and junior community health extension workers 21.4% and 15.8% respectively, a pharmacy technician (5.2%). None of the workers had gone for any in-service training within the two previous years and none of the facilities had a functional 2-way referral system in place. [39]
A Papua New Guinea review of health service features such as physical facilities, staff performance, levels of supervision and availability of basic drugs and equipment suggested that management weakness and wide variation in supervision visits were contributing to the poor quality of care of the rural facilities. [40]
ESSENTIAL ELEMENTS OF PRIMARY HEALTH CARE (PHC)
There are 8 elements of primary-health care (PHC) listed below:
1. Education concerning prevailing health problems and the methods of identifying, preventing and controlling them.
2. Locally endemic disease prevention and control.
3. Expanded programme on immunization against major infectious diseases.
4. Maternal and child health care including family planning.
5. Essential drugs arrangement.
6. Nutritional food supplement, an adequate supply of safe and basic nutrition.
7. Treatment of communicable and non-communicable disease and promotion of mental health.
8. Safe water and sanitation.
Extended Elements in 21st Century include:
1. Expanded options of immunizations.
2. Reproductive health needs.
3. Provision of essential technologies for health.
4. Health promotion.
5. Prevention and control of non-communicable diseases.
6. Food safety and provision of selected food supplements.[41]
STRATEGIES FOR IMPLEMENTATION
As it is in other parts of the world, Nigeria has its own peculiarities characterizing the health care system. These peculiarities are related to her cultural, religious, and sociopolitical diversities. Thus, strategies to implement primary health care must be evolved to meet the challenges associated with these diversities. These strategies include community mobilization and advocacy, service integration, health research, capacity building, and international and non-governmental collaborations.
Community mobilization and advocacy: Community mobilization is the process of arousing the interest of the people and encouraging them to participate actively in finding solutions to their problems (Olise, 2007). It is the gateway to providing effective healthcare services to individuals, families and groups within the communities concerned. Community mobilization engenders community participation and community ownership, and ultimately guarantees sustainability of health programmes (Magawa, 2012). In addition, it enhances resource mobilization, cost minimization and appropriate utilization of health services. Adequate resource mobilization and usage is particularly crucial in resource-poor settings for the implementation of primary health care.
Service integration: Service integration in primary health care has been described as the process of including either the elements of one service or an entire service into the regular functioning of another service (NPHCDA, 2012). It implies providing two or more primary health care services on the same platform by the same team and often simultaneously. This strategy enhances efficiency, prevents duplicity and wastage of resources, and improves availability and accessibility of a wide range of health care services. Service integration is the principle that underlies the Integrated Management of Childhood Illness (IMCI), Integrated Maternal Newborn and Child Health (IMNCH), Maternal Newborn and Child Health Week (MNCHW) and the Immunization Plus Days (IPDs) (Federal Government of Nigeria, FGN, 2007).
Health research: Health research provides a means of systematically identifying health related problems and their determinants so as to evolve ways to solve them. It entails identifying community health needs and their areas of strengths and weakness in order to appropriately deploy and utilize available resources. Efforts have been initiated globally to emphasize the importance of evidence based programming through the application of research findings in policy making processes (Uneke et al, 2010).
International Journal of Community Research http://www.arpjournals.com ISSN: 2315 – 6562 E-ISSN: 2384 – 6828 Alenoghena et al., IJCR 2014; 3(3): 74-79. 76 Nigeria’s National Strategic Health Development Plan (NSHDP 2010-2015) identified Research for Health as a priority area aiming to utilize research for informed policy making and programming, as well as improve health, achieve nationally/international health-related development goals, and contribute to the global knowledge platform.
Capacity building: Manpower development is crucial to quality health care delivery. It is required to be a continuous process in order to effectively deal with the constantly evolving health care needs of the people. Primary health care workers and managers need to be trained and retrained on regular basis through workshops, seminars, special courses, and in some cases, in higher degrees. The essence is to maintain a vibrant workforce. Health care workers offering PHC services are no second-class practitioners, and thus must receive government’s attention in the area of capacity building.
Non-governmental and international collaborations: The burden of providing health care services to the grass roots need not be borne by government alone. The role of non-governmental organizations (NGOs) has long been recognized in promoting primary health care as noted by the World Federation of Public Health associations (WFPHA, 1978) and continues to be advocated to fill up important gaps (Health Systems Trust, 2013). NGOs and international partners are relevant in supporting PHC programmes with funding, capacity building, operational research and technical assistance. Prominent NGOs and international partners currently supporting PHC services in Nigeria include the Society for Family Heath, United Nations Children Fund (UNICEF), Achieving Health Nigeria Initiative (AHNI), and Pathfinders International among others. These organizations should be encouraged to do more in enhancing primary health care. [42]
CHAPTER THREE: MATERIALS AND METHODS
3.1 STUDY AREA
Obio-Akpor is a Local Government Area in the metropolis of Port-Harcourt, one of the major centres of economic activities in Nigeria, and one of the major cities of the Niger Delta, located in Rivers State. The Local Government Area covers 260km2 and at the 2006 census held a population of 464,789. Its postal code or ZIP code is 500102.
Obio-Akpor is located between latitudes 4º45’N and 4º60’N and longitudes 6º50’E and 8º00’E. It is bounded by Port Harcourt LGA to the South, Oyigbo LGA to the East, Ikwerre LGA to the North and Emohua LGA to the West. Obio-Akpor is one of the 8 local government areas that formed the Rivers East Senatorial District. It consists of 17 electoral wards administered by the Obio-Akpor Local Government Council.
Obio-Akpor has its headquarters at Rumuodomaya. Covering around 100 square miles, Obio-Akpor is generally a lowland area with average elevation below 30 metres above sea level. Its geology comprises basically of alluvial sedimentary basin and basement complex. The thick mangrove forest, raffia palms and light rainforest are the major types of vegetation. Due to rainfall, the soil in the area is usually sandy or sandy loam. It is always leached, underlain by a layer of impervious pan.
The indigenous people of the area are the Ikwerres. The occupation of its members ranges from civil servants to transport workers, business owners, students, white-collar job holders, manual labourers and several others. The predominant religion is Christianity. The educational status of most members of this community is at least secondary school qualification, due to the presence of numerous government-owned primary and secondary schools in the area.[43]
The Obio-Akpor Local Government Area has 20 Primary Health Care centers. 12 are comprehensive health care centers, 3 are primary health care clinics and 5 are basic health clinics of which 3 are health posts. Also, there are a few secondary health care facilities and 1 tertiary hospital which is the University of Port Harcourt Teaching Hospital.
3.2 STUDY DESIGN
A descriptive cross-sectional study will be used to determine the structural quality of the Primary Health Care facilities in Obio-Akpor Local Government Area according to the Minimum Standard for Primary Health Care in Nigeria.
3.3 STUDY POPULATION
The unit for the study are the Primary Health Care facilities in Obio-Akpor. A detailed facility survey would be done using a checklist and questionnaires.
3.4 ELIGIBILITY CRITERIA
Inclusion Criteria
All Primary Health Care facilities within Obio-Akpor LGA.
Exclusion Criteria
Any Primary Health Care facility that has not been functional in the past six months.
3.5 STUDY INSTRUMENT
A checklist and an interviewer-administered questionnaire would be used for this study.
3.6 DATA COLLECTION
The data collection will be done on weekdays in the month of August within working hours which is between 8am to 4pm. These days have been selected because it affords us the opportunity to meet the heads of these facilities whom the questionnaires are to be administered to as they will more likely to be available within this time frame. This time frame also fits our academic calendar when we will be relatively free that can afford us the opportunity to be present at the health facilities at the said time without much compromise in our regular academic engagements.
We will address the heads of these facilities explaining to them the aim of our coming and obtain a verbal consent before proceeding to administer the questionnaires or use the check lists.
3.7 DATA ANALYSIS
The questionnaires would be cross-checked and the data entered into the computer using 2016 Microsoft EXCEL spread sheet. The analysis of the data would be done using Statistical Package for Social Sciences (SPSS) version 22.
3.8 ETHICAL CONSIDERATIONS
The study will be conducted in accordance with proper ethical principles guiding the use of human participants in research. The approval for this study will be obtained from the Ethics Committee of University of Port-Harcourt Teaching Hospital (UPTH). The verbal consent will be obtained from all participants. They will be informed that the information obtained will be strictly used for research purposes.
3.9 TIME FRAME
This study is expected to run between June 2017 and November 2017.
CHAPTER FOUR: RESULTS
This study was carried out on all primary health care facilities in Obio-Akpor Local Government Area of Rivers state, Nigeria. There are 20 primary health care facilities, 19 questionnaires were retrieved from the functional 14 primary health care centres and 5 primary health posts.
4.1 INFRASTRUCTURAL ASSESSMENT
Table 4.1 below illustrates the percentage distribution of the infrastructure of primary health care centres. 100% of the centres were a fenced compound with gate, had a consultation room, a delivery room and a medical records area. 92.9% had a maternity/lying in section and injection/dressing area, 35.7% had a food demonstration area, 21.4% had a kitchen and 85.7% had good access roads.
100% facilities had essential drugs list. 92.9% had sanitary toilet facilities and sanitary waste collection points, 85.7% had regular water, alternative power sources and waste disposal, 64.3% had a maintenance plan, 57.1% had sign posts visible from both sides and 7.1% had a centre phone line.
100% of the primary health posts had good accessible roads, 80% had a sanitary waste collection point, 60% had a waiting area, water supply inside the facility and a sanitary toilet facility, 40% had regular water supply, waste disposal and sign posts visible from both sides. No (0%) primary health post had a delivery room, maternity/lying in section, medical records area, procedure room, food demonstration area, kitchen, regular power supply, alternate power sources, centre phone line, maintenance plan, essential drugs list and a functional ambulance.
Table 4.1 showing infrastructural assessment of primary health care centres.
| Attribute | Frequency | Percent |
| Fenced compound with gate | 14 | 100 |
| Consultation room | 14 | 100 |
| Waiting area | 14 | 100 |
| Delivery room | 14 | 100 |
| Maternity/lying in section | 14 | 100 |
| Medical records area | 14 | 100 |
| Injection/dressing area | 13 | 92.9 |
| Procedure room | 11 | 85.7 |
| Food demonstration area | 5 | 35.7 |
| Availability of kitchen | 3 | 21.4 |
| Access road to facility | 12 | 85.7 |
| Regular water supply | 12 | 85.7 |
| Source of water inside the facility | 14 | 100 |
| Regular power supply | 3 | 21.4 |
| Alternate power sources | 12 | 85.7 |
| Sanitary toilet facility | 13 | 92.9 |
| Sanitary waste collection point | 12 | 85.7 |
| Waste disposal site | 12 | 85.7 |
| Signposts visible from both sides | 8 | 57.1 |
| Centre phone line | 1 | 7.1 |
| Maintenance plan | 9 | 64.3 |
| Essential drugs list | 14 | 100 |
| Functional ambulance | 7 | 50 |
Table 4.2 showing the infrastructural assessment of the primary health posts in Obio-Akpor LGA
| Attribute | Frequency | Percent |
| Fenced compound with gate | 2 | 40 |
| Consultation room | 2 | 40 |
| Waiting area | 3 | 60 |
| Delivery room | 0 | 0 |
| Maternity/lying in section | 0 | 0 |
| Medical records area | 0 | 0 |
| Injection/dressing area | 2 | 40 |
| Procedure room | 0 | 0 |
| Food demonstration area | 0 | 0 |
| Availability of kitchen | 0 | 0 |
| Access road to facility | 5 | 100 |
| Regular water supply | 2 | 40 |
| Source of water inside the facility | 3 | 60 |
| Regular power supply | 2 | 40 |
| Alternate power sources | 0 | 0 |
| Sanitary toilet facility | 3 | 60 |
| Sanitary waste collection point | 4 | 80 |
| Waste disposal site | 2 | 40 |
| Signposts visible from both sides | 2 | 40 |
| Centre phone line | 0 | 0 |
| Maintenance plan | 0 | 0 |
| Essential drugs list | 0 | 0 |
| Functional ambulance | 0 | 0 |
Table 4.3 Comparison of attributes between PHC and Health Post.
| Attributes | Frequency(Percent) | Chi-square | p-value | |
| PHC | HC | |||
| Fenced compound with gate | 14 (100) | 1 (20) | 14.187 | 0.000 |
| Consultation room | 14 (100) | 2 (40 | 14.187 | 0.000 |
| Waiting area | 14 (100) | 3 (60) | 6.259 | 0.012 |
| Delivery room | 14 (100) | 0 (0) | 19.000 | 0.000 |
| Maternity/lying in section | 14 (100) | 0 (0) | 14.702 | 0.000 |
| Medical records area | 14 (100) | 0 (0) | 19.000 | 0.000 |
| Injection/dressing area | 13 (92.9) | 1 (20) | 10.086 | 0.001 |
| Procedure room | 12 (85.7) | 0 (0) | 9.330 | 0.002 |
| Food demonstration area | 5 (35.7) | 0 (0) | 2.423 | 0.120 |
| Availability of kitchen | 3 (21.4) | 0 (0) | 1.272 | 0.259 |
| Access road | 12 (85.7) | 5 (100) | 0.798 | 0.372 |
| Regular water supply | 12 (85.7) | 2 (40) | 3.971 | 0.046 |
| Water supply inside facility | 14 (100) | 3 (60) | 6.259 | 0.012 |
| Regular power supply | 3 (21.4) | 2 (40) | 1.272 | 0.259 |
| Alternate power sources | 12 (85.7) | 0 (0) | 11.633 | 0.001 |
| Sanitary toilet facility | 13 (92.9) | 3 (60) | 2.991 | 0.084 |
| Sanitary waste collection point | 13 (92.9) | 4 (80) | 0.647 | 0.421 |
| Waste disposal site | 12 (85.7) | 2 (40) | 3.971 | 0.046 |
| Signposts visible from both sides | 8 (57.1) | 2 (40) | 0.434 | 0.510 |
| Centre phone line | 1 (7.1) | 0 (0) | 0.377 | 0.539 |
| Maintenance plan | 9 (64.3) | 0 (0) | 6.107 | 0.013 |
| Essential drugs list | 14 (100) | 0 (0) | 19.000 | 0.000 |
| Functional ambulance | 7 (50) | 0 (0) | 3.958 | 0.047 |
4.2 ORGANISATIONAL STRUCTURE
Figure 4.4 below represents the organisational assessment of the primary health care centres
100% of the facilities had a management committee and regular management committee meetings,
92.9% of the facilities had members of community served as part of the management committee and also 92.9% had the community served partaking in the planning and management. 92.9% had work schedule for staff.
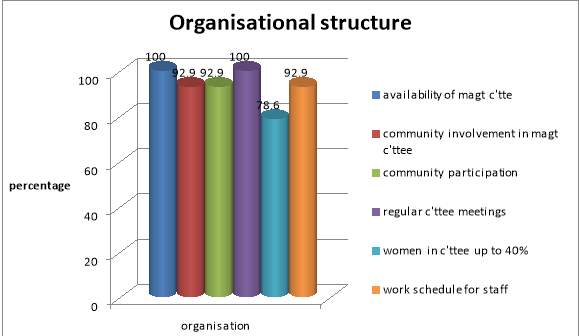
Figure 4.1 Organisational structure of primary health care centres in Obio-Akpor Local Government Area.
4.3 SERVICES ASSESSMENT
From figure 4.6 below, 100% of primary health care centres render out-patient , ante-natal family planning and delivery services. 100% all offer minor surgical services like incision and drainage. 92.9% give immunisation services.
100% of facilities had laboratory and pharmacy services, 100% had essential drugs, supervision and maintenance of records services. 92.9% had available guidelines for management of common conditions like diarrhoea and 35.7% had nutrition/catering services.
100% had counselling/health promotion and water and sanitation services, 92.9% had infant welfare, out-reach and a functional 2-way referral system services, 85.7% had 24/7 health services and 35.7% had adolescent health services.
100% of the primary health posts render out-patient and counselling/health promotion services, 80% render out-patient, family planning and infant welfare services, 40% have supervision services and have guidelines for the management of common conditions, 20% have a pharmacy and essential drugs
Table 4.4 showing services provided by the primary health care facilities.
| Services | Frequency | Percent |
| Out-patient | 14 | 100 |
| Ante-natal | 14 | 100 |
| Family planning | 14 | 100 |
| Immunization | 13 | 92.9 |
| Counselling/Health promotion | 14 | 100 |
| Laboratory | 14 | 100 |
| Pharmacy | 14 | 100 |
| Nutrition/catering | 5 | 35.7 |
| Delivery | 14 | 100 |
| Infant welfare | 13 | 92.9 |
| Outreach services | 13 | 92.9 |
| Essential drugs | 14 | 100 |
| Water and sanitation | 14 | 100 |
| Functional 2-way referral system | 13 | 92.9 |
| Maintenance of records | 14 | 100 |
| Supervision | 14 | 100 |
| Waste disposal | 14 | 100 |
| Adolescent health services | 5 | 35.7 |
| 24/7 services | 12 | 85.7 |
| Surgical services (incision & drainage) | 14 | 100 |
| Availability of guidelines for management of common conditions | 13 | 92.9 |
Table 4.5 showing services delivered by primary health posts.
| Services | Frequency | Percent |
| Out-patient | 4 | 80 |
| Ante-natal | 3 | 60 |
| Family planning | 4 | 80 |
| Immunization | 5 | 100 |
| Counselling/Health promotion | 5 | 100 |
| Laboratory | 0 | 0 |
| Pharmacy | 1 | 20 |
| Nutrition/catering | 1 | 20 |
| Delivery | 0 | 0 |
| Infant welfare | 4 | 80 |
| Outreach services | 0 | 0 |
| Essential drugs | 1 | 20 |
| Water and sanitation | 0 | 0 |
| Functional 2-way referral system | 0 | 0 |
| Maintenance of records | 0 | 0 |
| Supervision | 2 | 40 |
| Waste disposal | 0 | 0 |
| Adolescent health services | 0 | 0 |
| 24/7 services | 0 | 0 |
| Surgical services (incision & drainage) | 0 | 0 |
| Availability of guidelines for management of common conditions | 2 | 40 |
Table 4.6 Comparison between services delivered by primary health care centres and primary health posts.
| Attributes | Frequency(Percent) | Chi-square | p-value | |
| PHC | HC | |||
| Out-patient | 14 (100) | 4 (80) | 2.956 | 0.086 |
| Ante-natal | 14 (100) | 3 (60) | 6.259 | 0.012 |
| Family planning | 14 (100) | 4 (80) | 2.956 | 0.086 |
| Immunization | 13 (92.9) | 5 (100) | ||
| Counselling/Health promotion | 14 (100) | 5 (100) | 14.702 | 0.000 |
| Laboratory | 14 (100) | 0 (0) | 19.000 | 0.000 |
| Pharmacy | 14 (100) | 1 (20) | 14.187 | 0.000 |
| Nutrition/catering | 5 (35.7) | 1 (20) | 0.421 | 0.516 |
| Delivery | 14 (100) | 0 (0) | 19.000 | 0.000 |
| Infant welfare | 13 (92.9) | 4 (80) | 0.647 | 0.421 |
| Outreach services | 13 (92.9) | 0 (0) | 14.702 | 0.000 |
| Essential drugs | 14 (100) | 1 (20) | 14.187 | 0.000 |
| Water and sanitation | 14 (100) | 0 (0) | 19.000 | 0.000 |
| Functional 2-way referral system | 13 (92.9) | 0 (0) | 14.702 | 0.000 |
| Maintenance of records | 14 (100) | 0 (0) | 19.000 | 0.000 |
| Supervision | 14 (100) | 2 (40) | 9.975 | 0.002 |
| Waste disposal | 14 (100) | 0 (0) | 19.000 | 0.000 |
| Adolescent health services | 5 (35.7) | 0 (0) | 2.423 | 0.120 |
| 24/7 services | 12 (85.7) | 0 (0) | 11.633 | 0.001 |
| Surgical services (incision & drainage) | 14 (100) | 0 (0) | 19.000 | 0.000 |
| Availability of guidelines for management of common conditions | 13 (92.9) | 2 (40) | 6.193 | 0.013 |
4.4 ESSENTIAL DRUGS
Table 4.7 below shows that 100% of the primary health care centres and primary health posts have antimalarials, ORS, hematinics, analgesics and anticonvulsants.
Table 4.7 representing essential drugs available at the primary health care facilities.
| ESSENTIAL DRUGS | PHC | HP | |||
| FREQUENCY | PERCENT | FREQUENCY | PERCENT | ||
| ANTI MALARIAL (ACTs) | 14 | 100 | 5 | 100 | |
| ORS | 14 | 100 | 5 | 100 | |
| HEMATINICS | 14 | 100 | 5 | 100 | |
| ANALGESICS | 14 | 100 | 5 | 100 | |
| ANTICONVULSANTS | 14 | 100 | 5 | 100 | |
4.5 ESSENTIAL EQUIPMENTS
Table 4.8 shows that 100% of primary health care centres had a sphygmomanometer, stethoscope, weighing scale, growth chart, partograph, malaria kits, HIV kits, thermometer, gloves and gauzes. 92.9% had delivery couch and ice pack.
100% had a weighing scale and a growth chart, 80% had a sphygmomanometer, a stethoscope and a thermometer, 60% had malaria kits, 40% had HIV kits and fetoscope, and 0% had a delivery couch and a partograph.
Table 4.8 Essential Equipments
| PRIMARY HEALTH CENTRE | PRIMARY HEALTH POST | |||
| FRQUENCY | PERCENT | FREQUENCY | PERCENT | |
| SPHYMOMANOMETER | 14 | 100 | 4 | 80 |
| STETHOSCOPE | 14 | 100 | 4 | 80 |
| WEIGHING SCALE | 14 | 100 | 5 | 100 |
| DELIVERY COUCH | 13 | 92.9 | 0 | 0 |
| GROWTH CHART | 14 | 100 | 5 | 100 |
| PARTOGRAPH | 14 | 100 | 0 | 0 |
| MALARIA KITS | 14 | 100 | 3 | 60 |
| HIV KITS | 14 | 100 | 2 | 40 |
| FETOSCOPE | 14 | 100 | 2 | 40 |
| THERMOMETER | 14 | 100 | 4 | 80 |
| GLOVES | 14 | 100 | 4 | 80 |
| GAUZES | 13 | 92.9 | 3 | 60 |
| ICE PACK | 13 | 92.9 | 4 | 80 |
4.6 STAFF QUALITY
Assessment of the staff strength of the primary health care facilities was done through the administration of questionnaires to the available members of staff on the spot. 68 members of staff were encountered during this study.
The mean age of the staff members is 35.9 years
Table 4.9 Staff mix at the Primary Health Care Facilities
| Staff | Frequency | Percent | |
| Doctor | 7 | 10.3 | |
| Nurse | 21 | 30.9 | |
| Pharmacist | 2 | 2.9 | |
| Lab Scientist | 5 | 7.4 | |
| Pharm tech | 9 | 13.2 | |
| JCHEW | 13 | 19.1 | |
| SCHEW | 4 | 5.9 | |
| CHO | 2 | 2.9 | |
| VHW | 1 | 1.5 | |
| OTHERS | 4 | 5.9 | |
| Total | 68 | 100 |
Figure 4.2 shows that 73.5% of the members of staff are full time workers while 26.5% are part-time workers.

Figure 4.2 A graphical representation of job status of primary health care facility workers.
Figure 4.3 shows that 60.3% of the primary health care staff have had a job related training, while 39.7% have not.
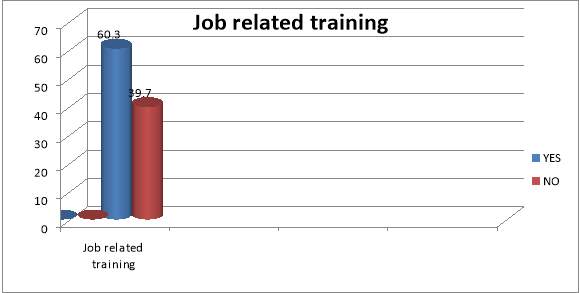
Figure 4.3 A graphical representation of the percentage of primary health care workers with 0job related training in the last one year.
Figure 4.4 shows that 89.7% of staff members receive supervisory support, 7.4% do not receive supervisory support, 2.9% do not know.
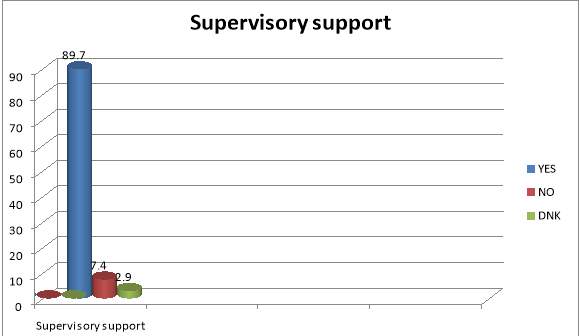
Figure 4.4 A graphical representation of the primary health care workers who receive supervisory support.
CHAPTER 5: DISCUSSION
The study was carried out to assess the structural quality of Primary Health Facilities using Obio-Akpor LGA, Rivers State, Nigeria as a case study.
Assessment of the infrastructure, organisation and the quality of services delivered were the objectives of the study, as these parameters form the framework and bedrock for the effective functioning of these facilities as well as the staff integrity.
From the study conducted it was shown that 100% of the primary health care facilities were a fenced compound with gate and 57.1% had signposts visible from both sides, as opposed to 20% and 40% respectively of the primary health posts which were a fenced compound and had a signpost visible from both sides. 85.7% of the primary health facilities had accessible roads. A study done by A. S Mohammed, I. E idowu and Y. A Kuyin in Ikoji Ejirim, Lagos, showed that only 33% of the facilities could be accessed through public transportation.
From this study it was shown that 85.7% of the primary health centres and 40% of the primary health posts had regular water supply. As compared to the study done by S. Mohammed et al study which showed that 77.7% of the primary health centres had inadequate water supply.
In this study only 7.1% of the facilities had a centre phone line, which includes no primary health posts.
64.3% of the primary health care facilities had a maintenance plan. This is in discordance with the A. S Mohammed study where none of the facilities had a maintenance plan.
In this study, none of the health posts and 50% of the primary health centres had a functional ambulance. Also 92.9% of the health centres had a functional 2-way referral system. The Ikoji Ejirim study showed that only 11.1% had a functional ambulance and none had a functional 2-way referral system.
All primary health care facilities had a management committee and 92.9% of the facilities had the community served participate in planning and management. None of the health posts had this privilege. This is also in disagreement with the A. S Mohammed study where only 22.7% of the facilities enjoy community participation in planning and management
Essential drugs were available in all primary health care centres and 20% of primary health posts. Phill Buttel’s evaluation Using Service Delivery Indicator showed that 46% of service centres had essential drugs. Hence there is disparity with the study.
There is a wide discrepancy between the quality assessment values for the primary health care centres and the primary health posts, due to lesser requirements from the minimum standard in part, although none of the facilities had regular power supply and alternate power sources.
Junior Community Health Extension Workers (JCHEW) comprised 19.1% of the staff mix, 5.9% were Senior Community Health Extension Workers (SCHEW) and 30.9% were nurse/midwives. This is in relative disagreement with the Ijoji Ejirim study which showed that the workers comprised nurses/midwives (57.9%), senior and junior community health extension workers 21.4% and 15.8% respectively, a pharmacy technician (5.2%).
In most developing countries, the health workforce is concentrated in the major towns and cities, while rural areas can only boast of about 23% and 38% of the countries doctors and nurses respectively according to Anyangwe SC and Mtonga C.
In this study, 60.3% of the staff members have had a job related training in the past one year and 73.5% were full time workers in the facility. None of the health workers had gone for any training in the two previous years in the A. S Mohammed et al study.
From the study, 89.7% of members of both primary health care and health posts’ staff receive supervisory support. Phil Buttel’s evaluation using Service Delivery Indicator (SDI) surveys show that 23% of facilities received supervision infrequently (9% received visits 1-2 times in a year or not at all, 14% received no visits at all). This has resulted in absence from duty posts from respective health service providers, lateness to work and a punctuated 24 hour service delivery.
LIMITATIONS
A major limitation to this study is the paucity of similar relevant studies to validate the results obtained.
Also, it is entirely impossible to evaluate all the minimum requirements required for both primary health posts and health centres due to logistics and feasibility reasons. For example, assessing the recommended perimeters for building.
The study evaluated the presence or absence of a required infrastructure or service rather than the quantity and quality of it.
This study was based on a one-stop evaluation of the facilities and does not put into account members of staff that were not around as at the time of assessment.
Locating some of the health centres was a challenge, even for residents of the location, as they lacked visible signposts from both sides.
IMPLICATIONS
This study has highlighted the deficient areas in primary health care facilities. In infrastructure, organisation and service delivery. Particular areas of deficiency of interest include accessible roads, regular and alternative power supply, centre phone lines for emergencies and a functional ambulance.
Also, this study showcased the enormous inadequacy of the primary health posts especially.
Only 68 members of staff were encountered on this one-stop evaluation process. This is a subjective evaluation of the staff strength of the health care centres.
CONCLUSION
Primary health care is the framework for enhancing the health care delivery system of any country. Most developed countries with better indices and indicators of health adopted this grass-root method of health care delivery.
Since the inception of primary health care in Nigeria, there has been a decline in infant mortality rate by 21% from 1990 to 2013 and under-5 mortality rate by 34% over the same period.
However it is important to note that the same force and energy used to initiate the system is equally required to maintain it.
The primary health care system in Obio-Akpor local government area of Rivers State is of good standard according to the assessment scores of this study.
This may be due to a recent primary health care purpose-driven refurbishment of the health system in Obio-Akpor Local Government Area by the Rivers State government.
This could account for the up to date infrastructure in the primary health centres especially and the wide discrepancy with that of the primary health posts.
RECOMMENDATIONS
- The government and non-governmental organisations (NGOs) can sponsor the study of other primary health care centres in other local government areas who have not received the attention given to Obio-Akpor LGA.
- A study on the quality and quantity of infrastructure/equipments should be done.
- Primary health posts in Obio-Akpor LGA should be upgraded to quality first contact health systems as recommended.
We hope this example dissertation proposal has helped you with your studies. See our guide on How to Write a Dissertation Proposal for guidance on writing your own proposal.
Cite This Work
To export a reference to this article please select a referencing stye below:
Related Services
View all


Related Content
All TagsContent relating to: "Healthcare"
Healthcare is defined as providing medical services in order to maintain or improve health through preventing, diagnosing, or treating diseases, illnesses or injuries.
Related Articles

DMCA / Removal Request
If you are the original writer of this dissertation proposal and no longer wish to have your work published on the UKDiss.com website then please: