Comparison Between Underwater Aerobic Exercises and Manual Knee Exercises in Rehabilitation of Knee Osteoarthritis
Info: 3947 words (16 pages) Example Dissertation Proposal
Published: 19th Mar 2021
Tagged: MedicinePhysiotherapy
Comparison between underwater aerobic exercises and manual knee exercises in rehabilitation of knee osteoarthritis in middle age athletes.
Introduction
Osteoarthritis (OA) is the most common cause of joint disease worldwide, with a tremendous impact both due to the number of people affected and the disabling consequences for those who develop symptomatic disease. The lifetime risk of developing knee OA is around 46 % and it is estimated that symptomatic disease occurs in 10 % of men and 13 % of women aged 60 years or over [1].
It is more common in women than men. Among 1 per 100,000 world standard population in 2000 the prevalence for males was 1,770 and for females were 2,693. As it is an irreversible disease its prevalence increases radically with age. OA is the 4th leading cause of Year lives with disability (YLDs) at a global level; accounting for 3.0% [2]. In the United States the prevalence of radiographic knee OA in adults of age 60 and above is 42.1% in women and 31.2% in men [3].
In a prospective study in which data were provided by radiographs, physical performance assessment, and interviews in 1996 and again (with the addition of magnetic resonance imaging assessment) in the follow-up visit during the years 2007, 2008. The prevalence of moderate-to-severe knee osteoarthritis changed from 3.7% at the baseline assessment to 26.7% in the follow-up visit eleven years later. Middle-aged women had a high prevalence of moderate-to-severe knee osteoarthritis [4].
Middle age can be defined as “the period between early adulthood and old age, usually considered as the years from about 45 to 65.” According to the Oxford English Dictionary [5].
Osteoarthritis is the most common condition affecting synovial joints. Osteoarthritis of the knee causes substantial pain and disability, especially in the elderly, resulting in a significant burden on health care provision. The majority of patients with osteoarthritis are managed in primary care, and the prevalence of knee osteoarthritis is such that simple interventions which are effective in a community setting are necessary. Treatment of osteoarthritis aims to reduce pain and disability [6].
Patients with knee OA typically present with reduced force-generating ability in the quadriceps that can be attributed to muscular atrophy as well as muscular inhibition, which is the inability to fully and volitionally activate the muscle [7-9]. In addition to Subjects with knee OA have significant muscle impairments regarding quadriceps, hamstrings, and hip muscles [10]. Furthermore, Muscle power is an independent determinant of pain and quality of life in knee OA. Compared to strength, muscle power may be a more clinically important measure of muscle function within this population [11].
Postural stability could be defined as control over body’s position in space for orientation and balance purpose [12]. Static and dynamic balance is an essential part during activities of daily living (ADLs) and ambulation. Impaired postural stability is one of the main reasons of falls in older adults [13], and which is one of the main causes of fatalities and hospital [14].
Loss of proprioception, which may affect postural stability, is a major problem in people with knee OA. Bilateral knee osteoarthritis impaired the balance and increased the risk of fall, particularly in people with moderate knee osteoarthritis. Also, knee OA results in progressive loss of function including: gait, stair climbing and other physical activities which involve lower limb. In fact, it reduces the quality of life [15].
Recent guideline for the management of knee osteoarthritis emphasise the central role of exercise. Aerobic walking exercises have been shown to reduce pain and disability in subjects with knee osteoarthritis [16].
The necessity of this study will be to add a new knowledge in the rehabilitation research field about the efficacy of Aquatic therapy comparison to manual starching and strengthening exercises, as rehabilitation modalities, in the rehabilitation of chronic knee OA through improving isokinetic muscle power, increase balance, allow higher functional level and improve their patients’ quality of life.
Therefore, the aim of this study will be to compare between underwater aerobic exercises and manual knee exercises in rehabilitation of knee osteoarthritis.
The null hypothesis of this study will be that:
There will be no statistical significant difference between underwater aerobic exercises and manual knee exercises in rehabilitation of knee osteoarthritis regarding isokinetic muscle power, balance, functional ability level.
Subjects and Methods
Study Design
This study will be randomized, pre-test and post-test design study. Patients who would meet the selection criteria will be divided randomly into two equal groups, (Group A) or (Group B). Randomization will be allocated using the numbered envelops method. Subjects will be blinded about which group they will be allocated.
Subjects
The study will be conducted in the period between Jan and Dec 2018. Male participants diagnosed as OA of the knee with grade II and III based on the Kellgren & Lawrence radiological classification and age ranged from 45- 65 years will be selected for this study from Hospitals.
Inclusion criteria will be as follows:
– age between 45 and 65 years;
– Knee OA will be diagnosed according to the American College of Rheumatology criteria (Figure 1) using history and physical examination [17, 18];
Knee OA classified as grade II and III (Figure 2) based on the Kellgren & Lawrence radiological classification [19];
– old athlete performing exercises in a regular basis
The exclusion criteria will be as follows:
-pacemaker use;
-unstable heart conditions;
– participate in another physical activity program;
– inability to walk on a treadmill;
– previous knee or hip arthroplasty;
-subjects receive pain killer or other OA medications;
– obese participants with BIM more than 30 (calculated by the equations: BMI=
WeightHeight in meter square
) [20].
– diagnosis of fibromyalgia; epilepsy; and presence of a tumor or cutaneous lesion that could interfere with the procedure.
All patients were given a full explanation of the treatment protocol and a written informed consent form giving agreement to participation and publication of results was signed by the patients.

Figure (1): ACR Clinical Classification Criteria for Osteoarthritis of the knee (Using history and physical examination) (Adopted from jhrheumatology [21]).
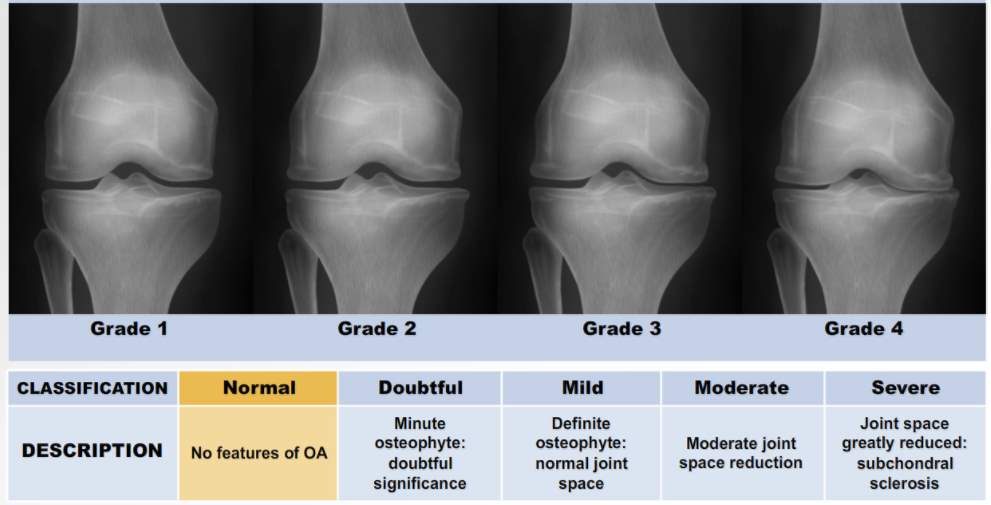
Figure (2): Kellgren & Lawrence radiological classification of knee OA (Adopted from A.D.A.M. [22]).
Randomization and blinding
The participants who agree to participate in the study will be randomly allocated into one of two groups: group A (underwater aerobic training); or group B (manual exercises). A computer-generated randomization schedule will be used to generate the randomization lists using blocks of four. A research coordinator not involved in the randomization will prepare the envelopes for the randomization procedure. The envelopes will be opened by the patients after the baseline test. The study will be single-blinded such that the assessors will be blinded to group allocation.
Outcome measures
All medical and demographic data of subjects will be collected (appendix 1) and the role of physical fitness importance in improving their condition will be explained.
Outcome measures will be assessment of muscle power and active range of motion (aROM) using Biodex Isokinetic Dynamometer (primary outcomes), assessment of balance by Biodex Balance System and the self-reported WOMAC aspects of functionality, pain, and stiffness (secondary outcomes). The assessment will be carried out before start of training and after 4 weeks at the end of training program.
Biodex Isokinetic Dynamometer
The lower extremity muscle power test will be performed using the Biodex III (Biodex Medical Systems, Shirley, NY, USA). The Biodex Isokinetic Dynamometer has been widely used in research, clinical settings and rehabilitation to objectively assess factors of muscle performance that is otherwise difficult to obtain using the manual testing technique [23].
It offers concentric, eccentric, isometric and passive modes for all joints. It measures the internal torque produced by the muscles while the bony segment is maintaining a constant angular velocity and range of motion. It is provided with many attachments and isolation straps for the trunk, shoulder, knee…etc. Performance measures are being automatically recorded by the system’s custom software at different angular velocities. The Biodex Isokinetic Dynamometer used in the current study consists of a dynamometer head, a closed chain attachment, a seat and a control unit (Figure 3) [24].
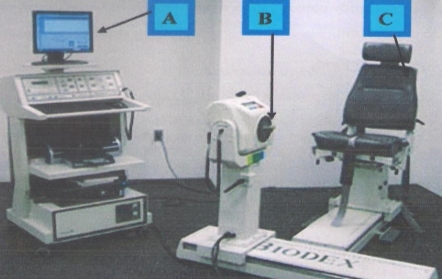
Figure (3): Biodex isokinetic dynamometer (system 3) and its component, A-The computer unit, B-The dynamometer, and C-The seat.
Knee flexor and extensors muscle power assessment and aROM procedure:
Assessment of knee flexor and extensors muscle power will be cared out using the Biodex Isokinetic Dynamometer (Biodex system III). The subjects sat in the Biodex chair with the hip joint at 90° and the motion axis of the knee joint straight with that of the machine. The trunk, hip, and thigh were fixed with waist and thigh belts. The medial ankle, its straight upper bone, and a lever were strapped with a belt. The test angles were limited to 0°–90° to prevent any injury during the test. A pre-exercise was done as practice once before the test was conducted. To test muscle function of the knee joint, maximum away and toward isometric strength of the subjects were measured for 5 sec at knee joint flexion of 30° and 60°, with a 1-min rest between the tests at each angle [25]. Also, aROM of knee extension and knee flexion will be recorded with the isokinetic device.
Biodex Balance System
The Biodex Balance system (Figure 4) (Biodex Medical System, Shirky Nyl 1967). provide reliable and repeatable objective measures of participants ability to balance. The Biodex Balance System allows accurate test and quickly generate a printed report. The system offers a choice of comprehensive, predictive values, bilateral comparison, these can be used to objectively measure and record the patient’s ability to maintain balance under dynamic stress. Dynamic balance testing will be performed on unlocked platform to allow free movement simultaneously in both the medial/lateral (ML) and anterior/posterior (AP) directions. The platform allows varying levels of resistance to perturbation of movement ranging from 1 to 8. The device measures the degree of tilt about each axis giving balance indices for AP and ML stability, and overall stability (OAS) based on tilt variance, whereby a large variance indicates reduced balance [26].
Balance assessment procedure:
Dynamic balance ability will be measured using the Balance System SD (Biodex Medical Systems).
- The position of the support handles and its height will be adjusted
- The display height and tilt will be adjusted for patient comfort.
- The weight, height and age of the patient will be entered to the control screen display located in front of the patient’s eyes.
- The platform firmness will be adjusted at level 6 with closed eyes and level 3 with open eyes [15].
- The foot position and angle for each patient will be recorded on the control display using the numeric grid on the platform (Heel co- ordinates will be measured from the center of the back of the heel and foot angle will be determined by finding a parallel line on the platform to the center line of the foot). The stance type will be adjusted at two leg stance.
- When a moving cursor at the center of a circle displayed on the screen leaned to one side, the subject will be balanced to maintain the most stable position possible without taking their feet off a footplate.
- The balance index will show the ability to control the unstable circular footplate, which divided into A, B, C, and D ranges as it moved away from the center of the circle to the perimeter and sectioned I, II, III, and IV along the X and Y axes. The circular footplate had a 5° incline interval for each range, and the total incline from the stable position to range D was 20° [25].
- Prior to the testing, all the participants underwent a familiarization session.
During postural stability testing, the patient’s ability to control the platform’s angel of tilt is quantified as variance from center. A large variance is indicative of poor neuromuscular control.

Figure (4): BIODEX Balance System.
Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC)
The WOMAC questionnaire (appendix 2) contains 17 questions regarding the degree of difficulty to perform daily activities, such as stair use, to assess the physical function of patients. Patients are asked to rank the degree of difficulty in the last 72 hours in a scale from 0 (none) to 4 (severe). The individual score for the 17 questions is added up to a score that can range from 0-68. The greater the score, the worse the function. The WOMAC questionnaire also includes questions about pain, stiffness and difficulty performing daily activities (ADL). In this study, the WOMAC scores of pain, stiffness, and difficulty performing ADL activities were analyzed separately [27].
Treatment
Group A will include 20 knee OA participants, they will receive moderate intensity underwater aerobic exercises training (with intensity of maximum heart rate 50% to 70% [28]) and massage program, 3 sessions per week for 4 weeks and Group B will include 20 knee OA participants, they will receive manual starching exercises, manual strengthening exercise and massage program, 3 sessions per week for 4 weeks. Both groups will participate in a core strengthening program. For more clarification of some exercises and massage techniques, farther discerption are attached in appendix 4.
Preparatory procedures
Each patient will be informed about experimental process as well as the significance of study and write a consent (appendix 3) will be obtained from each participant. All equipment will be checked up, calibrated and prepared before application.
Determine resting heart rate (HRrest) and maximum heart rate (HRmax) to determine the target heart rate will be used for underwater aerobic exercise in group A subjects. HRmax=220-age Target heart rate can be calculated as a range of 50%–70% intensity (moderate aerobic training intensity) according to Karvonen method. THR = ((HRmax − HRrest) × % intensity) + HRrest [29]. Maximal heart rate will adjusted on the basis of the observation that the maximal heart rate during swimming is 10–13 beats lower compared with land based activities.
Hart rate will be determined using wearable underwater pulse oximeter.
Active exercise Phase
- Group A:
The water level was fixed at xiphoid or near xiphoid level, with the water temperature at 34°C. After warming up, continuous running with moderate intensity (65% to 75% of the heart rate reserve) for 45 min, will be performed on underwater 3 days/ week for 4 weeks as following.
Underwater Warm-up (5 minutes)
Walk, march and sidestep with variations in movement directions, arm movements, and by alternatively lifting the bent knee or lifting the straight leg like a toy soldier.
Flexibility training (10 minutes)
Twenty-four sets of stretching and flexibility exercises in neck, trunk, shoulders, pelvic area, thighs and legs, with 10–15 repetitions for each exercise.
Aerobic training (10 minutes)
Repeat walk moves, as done in the warm-up section, for 5 minutes and then move in place for another 5 minutes, including alternatively moving heels, feet and legs in side steps, forwards and backwards, concurrent with arm movements.
Lower body training (10 minutes)
Exercise by using the wall for support, including 17 sets of exercises in hips, knees, ankles and toes, with 10–15 repetitions of each exercise. Examples of the 17 sets of the exercises include forward kick, side leg lift, hamstring curl, buttocks squeeze, kick out, leg lift, small squats, toes in and toes out, Flamingo, crossovers, leg circles, side to side weight shift, front lunge weight shift, push away, point/flex toes, heel-toe lift, ankle circles, inversion/ eversion and toe curls.
Upper body training (10 minutes)
Twelve sets of exercises for arms, elbows, wrists, hands and fingers, with 10–15 repetitions of each exercise.
Because of the physical characteristics of water, the resistance increases with the velocity of movement. Thus, the individuals were instructed to move through the full range of motion for each repetition, without exceeding the exercise intensity stipulated [30].
- Group B:
Subjects of this group will participate in 45 min session of land based manual stretching and strengthening exercise 3 times per week for 4 weeks as following:
Warm-up (5 minutes)
The subjects in this group will start the exercise session with warming up exercise at 10% to 20% of their heart rate reserve in form of gentle muscle stretches, as well as gentle endurance exercises including walk, march and sidestep, with variations in moving directions, arm movements associated with deep breathing instruction for 5 mins to allow for conditioning of the body for the exercises [31].
Manual stretching exercises (20 minutes)
Lowe intensity, prolonged stretch will be applied for hamstrings, the gastrocnemius, knee extensors and iliopsoas muscles in which stretch is held by the therapist for 60 second and repeated three times for each muscle with 60 second rest time in between [32].
Lower limbs strengthening exercises (20 minutes)
Manual resisted exercise against moderate leading resistance will be applied for improving strength of manly quadriceps, hamstring, hip abductor and hip external rotator with each exercise will be performed in a controlled manner, two sets of 10 repetitions for the first 2 weeks, and 3 sets of 10 repetitions thereafter. Also, quadriceps specific exercises will be performed are for the inner range of knee extension using ankle weight over fulcrum in supine lying or long sitting position from 30 degrees to 0 degrees knee flexion. In addition, straight leg raise using ankle weight or manual resistance will be performed in supine lying [33].
Core exercises for both groups (10 min)
Subjects of both groups will perform strengthening exercises fro lower back, abdominal, and pelvic floor muscles using ball, such as marching on the ball, half crunch on the ball and oblique crunch on the ball. Also, floor based core strengthening exercises will be performed, for example, pelvic tilt, lying march, bridging, and planking exercises. These core exercises targeted specific muscle groups, because they may not get much use during daily activities. Each exercise will be performed for 2 sets of 10 repetition in the first 2 weeks then 3 sets of 10 repetitions will be performed thereafter.
Cool down exercises:
At the end of each session, there was a cool-down period consisting of slow running and stretching for 5 mins to avoid postural hypotension and venous pooling of blood [34].
Recovery and massage:
For improving recovery, relaxation of the muscles and more improving of the circulation an additional 20 min. of massage of lower extremities including Effleurage, Petrissage of Hamstring, Quadriceps and Calf muscles and Myofascial release of lower limb facia that applied by an expert massage therapist.
Sample size estimation
After a pilot study on four patient in each group, the sample size will be estimated with a two-tailed α value of 0.05 (type I error) and β of 0.2 (type II error).
Statistical Analysis
Statistical analysis will conducted using SPSS for windows, version 22 (SPSS, Inc., Chicago, IL). The current test involved two independent variables. The first one was the (tested group); between subject factor which had two levels (group A and group B). The second one was the (training periods); within subject factor which had two levels (before treatment, after treatment). In addition, this test involved eleven tested dependent variables as following:
Dynamic balance testing:
- Medial/lateral stability index (ML) with eye open
- Medial/lateral stability index (ML) with eye closed
- Anterior/posterior stability index (AP) with eye open
- Anterior/posterior stability index (AP) with eye closed
- Overall stability index (OAS) with eye open
- Overall stability index (OAS) with eye closed
Isokinetic muscle power and aROM assessment
- Knee extensors peak torque
- Knee flexor peak torque
- Knee flexion aROM
- Knee extension aROM
Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC)
Descriptive statistics will be expressed as mean ± standard deviation (SD). Comparison of different variables within and between groups will be performed using paired and unpaired t test in normally distributed data or Wilcoxon Sign Rank test and Mann Whitney U test in not normally distributed data respectively. The alpha level was set at 0.05. Data analyzed according to the intention to treat principle, in which the study groups are compared in terms of the treatment to which they were randomly allocated.
We hope this example dissertation proposal has helped you with your studies. See our guide on How to Write a Dissertation Proposal for guidance on writing your own proposal.
Cite This Work
To export a reference to this article please select a referencing stye below:
Related Services
View all


Related Content
All TagsContent relating to: "Physiotherapy"
Physiotherapy is the practice of targeted exercise and movement to provide rehabilitation and restore or improve function and correct movement following injury, illness, or disability. Physiotherapy can also help to maintain health and prevent future debilitation.
Related Articles

DMCA / Removal Request
If you are the original writer of this dissertation proposal and no longer wish to have your work published on the UKDiss.com website then please: