Available Standards for Cancer Registry Systems: A Systematic Review
Info: 10421 words (42 pages) Dissertation
Published: 9th Dec 2019
Tagged: Public HealthCancer
AVAILABLE STANDARDS FOR CANCER REGISTRY SYSTEMS: A SYSTEMATIC REVIEW
A SYSTEMATIC REVIEW OF AVAILABLE STANDARDS FOR CANCER REGISTRY SYSTEMS: ANALYSIS OF OBSERVED STANDARDS IN CONTINIENT AND COUNTRY LEVELS
Introduction:
Cancer is the generic term for the category of chronic diseases that make cells in human body grows, and spread to other part of body outside their normal limit. While the weight of these disease are noticeably increasing, and it has more morbidity and mortality cases than any other chronic diseases [1-6], yet burden and incidence knowledge are yet to be known [7-9].
Cancer registry is an information system designed for the organization of collected cancer data, storage, management, analysis and interpretation of cancer incidence [10-11]. Cancer registries system remains the rich source of information for a wide diversity of public health and other important cancer surveillance systems [12-14]. It is an important tool that is used to determine and understand cancer burden in a particular settings, and inform the authority about the current trend in order to establish an appropriate cancer control plan at all level of care [15-16]. They have been playing a crucial role in cancer management, measuring outcome, resource allocation, and enabling decision-making process [5, 17-18].
Over the past five decades, cancer incident data have gradually become available for more cancer types, data quality gauge have become more in-depth and mixed, and comparisons between registries have increasingly included descriptions of the registration techniques used[19-20].
Lack of quality patient data is one of the major contributions to poor management of cancer incidence [12]. The need for data quality and reliability of cancer incidence data for case management is an important aspect in understanding the occurrence for effective control planning [3, 12, 21-22].
Standardized cancer registry data remains one of the most efficient ways to plan the evaluation of epidemiological research on all aspects of cancer control [23-26]. Cancer registries system collects as complete meaningful and accurate information as possible. This includes clinical report of the disease, as well as demographic patient data, tumour, hospital, and relevant physician details. When this data is put together with the additional information relating to treatment and follow-up, metastases as well as date and cause of death if available, a complete and invaluable cancer registry database is created [12, 27-31]. This data may possibly be used in many fields: aetiological and epidemiological investigation, care planning, primary and secondary prevention, benefiting both patients and society [5, 10, 12, 27-28, 32]. Data collected for the purpose of a registry in the absence of standards contribute little beyond unreliable results toward subject management and control plan [33-34]
Since the establishment of the Cancer Incidence in five Continent series (CI5), the number of cancer registry populations for which data are obtainable as the contributor has improved noticeably from just 34 populations in Volume I to 424 populations in Volume X [35]. As a result, the data accessible from cancer registry populations, which lead to the amount of available information about each cancer registries, has also increased [29].
An urgent need for more standard cancer registries especially in developing countries are required, as only about 2% of population are covered from Africa, 6% from Asia, and 8% from Central and South America, where cancer burden are doubling and already recognized as a major health problem [3-4, 36-40].
Although there are many available review articles regarding information system standards [41-44], however, none of them are directly on cancer registry standards. Loane M., et al. reviewed the guidelines and standards for telemedicine [41]. Awaysheh A., et al. reviewed medical terminology standards and structured reporting [43]. Schreiner-Karoussou A., reviewed the image quality standards to control digital x-ray system [42]. And, Lena Stromback, et al. reviewed the standards for data exchange within system biology [44]. In order to ensure synchronization in the way in which we collect, validate and guarantee a baseline level of data quality in registries, standards are normally needed to determine and implement common rules. Especially within the divest environment, where excessive varieties generate inefficiencies or hinder effectiveness [45-46].
Even though, diverse standards may have been beneficial in different cancer registries, which are there to ensure accuracy and promote the use of registries’ data[14], four quality indicators (Completeness; Comparability; Timeliness; and Validity) have been described for Population Based-Cancer Registries (PBCR) by IARC [5, 47], and there is lack of comprehensive list of those standards in the literature.
This study intends to identify, assess, and itemize all the available standards related to cancer registry and their popularity in their development within different regions and countries where they are observed. We describe each standard according to their disparity and correlation between different countries from the most to the least observed standards in regard to available cancer data.
METHODOLOGY
Source of information
Electronic journals and databases were used as sources for identified study materials. The databases incorporated PubMed, Proquest and Web of Science. Gray literatures were identified for published and unpublished works using Google search engine and manual search which includes professional bodies’ web sites. The journals included are European Journal of Cancer, Journal of Registry Management, and other related journals [48]. Literatures were assessed for relevance by reading their titles. Relevant titles were accessed and summarized by reading their abstracts. References in the retrieved articles were reviewed to discover any additional sources of information. All the information sourced was then compacted and combined under the key topics to identify and remove duplicates [49].
Strategy for literature search
Online systematic search was conducted between the periods of 4th July, 2017 to 31stJuly, 2017 to identify literatures that described any beneficial standards for cancer registries; standards for disease reporting; and standards for developing disease registry or cancer reporting system [50-51]. Topics of particular concern includes; standards for disease reporting system, cancer registry system standards, best practice on cancer registration, data quality services, and registries performance indicators [49].
Search strategy keywords includes: “cancer registr*”, “cancer reporting”, “cancer reporting system”, “cancer registr* system”, “disease registr*”, “disease reporting”, “disease registr* system”, “registr* standards”, “data quality indicator”, and “Cancer registry development”. Search terms combinations were used according to the research theme and question. The Boolean operators and Medical Subject Heading (MeSH) was used in PubMed to identify relevant studies. A title/abstract advance search was performed using the above keywords term with the “AND” operator. Filter for study design, date, or Language restriction was not applied. A total record of 2,613 was retrieved; result searches where joint and duplicates were removed. [48-49, 51]. References were managed using Endnote software.
Selection criteria
For this study, articles were assessed and identified for relevancy by reading their titles first, then followed by reading the abstracts [49]. Articles describing standard cancer registry system development, population based cancer registries system, hospital based cancer registries system, cancer management system, cancer monitoring system, cancer registration information system, history of cancer registration, structured of disease registry system, data quality indicator, evaluation of cancer registration, and any relevant public health registry data standards were included in the review [51]. Exclusion criteria included registry systems studies that are only on cancer incidence, burden of cancer for specific site (i.e. lung cancer), cross sectional studies of different cancer types, registry report for cancer morbidity and mortality, cancer survivors, and cancer care reported outcomes were not eligible for inclusion [50].
Data extraction and study selection
A total of 2,613 citations were identified through the Pub Med, Proquest, and Web of Science database searches. Google search engine are used to identify for standards setters documents and other potential gray literatures.1,362 unique search results remained after duplicates were removed [51]. Subsequent to reviewing the titles, 1,170 articles were unwanted and 192 articles remained for abstracts screening. 138 records that are not related to standards cancer registry were set aside, 13 articles were also excluded because full-texts were not available, and 4 articles were in German language. 37 relevance articles full-text were retrieved for more specific inspection and eligibility [48].
37 articles that finally met the inclusion criteria were included in the study (figure 1: shows the PRISMA flowchart). The literatures included in this study has defined the standards for cancer registration and those explained the variability among different cancer registry standards setters, which enhance quality of cancer data for better management planning [48]. Information identified in this study includes standards for cancer registry systems, and data quality indicators observed, are presented in table 1.
Figure 1
Additional records identified through other sources
Records identified through database searching
(n = 2,613)
Identification
Screening
Eligibility
Included

Duplicates removed
(n = 1,251 )
Records after duplicates removed
(n = 1,362 )


Records excluded (n = 1,308). Where 1,170 excluded on title screening and 138 no relevance standards information
Records screened
(n = 1,362)


Potential Full-text articles assessed for eligibility
(n = 54)
Full-text articles excluded
(n = 17), 13 full text not available, and 4 excluded were in German language

Studies included in qualitative synthesis
(n = 37)
Fig 1: PRISMA Flowchart for study selection.
RESULTS
Description of selected studies
Thirty seven (37) articles that finally met the inclusion criteria were included in this study. Information included regarding identified studies, includes: the authors, reference, published year, Country/region and the indicators observed, are presented in table 1. Those literatures included in this study details different standards for cancer registration system and the variability among different cancer registry standard setters, which are used to enhance quality of cancer data for better management [48]. The articles included represent different regions, and aspect of quality registration techniques (table 1).
Objectives and Specifications for cancer reporting system standards
Numerous items for developing and supporting cancer registries were evaluated in the studies which we have found. Thirty three studies (89.1%) are of Cancer Registration, that they discussed different standards for cancer registry system. Four studies (10.8%) had presented features, standards, and comments on cancer biobanks; and tissue banks systems integration with cancer registries [52].
Several standards are currently presented by different institutes from different countries. Nineteen countries are represented in this review, six countries from Europe, four from Asia, four from Caribbean, Central and South America, two from North America, two from Oceanic, and one from Africa. US is the most frequent country with highest number of publications (9); followed by France with 5; Germany, Sweden and Japan each has 3 publications; Canada, Switzerland, and Australia each appeared in 2 papers; then, 1 article each appeared from New Zealand, Iran, Mexico, Nigeria, Cuba, Colombia, Martinique, and Pakistan.
In total, 19 standards have been observed, striving to assure quality data are produce in various registries. The US has the highest number of standards observed 18; followed by 16 in Canada and Japan. France observed 15 standards and 13 in Australia. 12 quality indicators observed in Germany and Norway; 10 from Sweden, Cuba and Mexico. 9 standards are observed in Switzerland and the UK; 8 in New Zealand; 7 in Iran and Martinique; 6 in Pakistan; and 4 standards in Nigeria and Colombia.
As can be seen in table 2; comparability is the most commonness among all the 19 standards observed, is reported by 33 articles (89.1%) in all the countries under this review. Accuracy is the second most frequent standards indicator, reported by 30 articles (81%) in 17 countries, followed by data quality in 29 articles from 14 countries. 27 articles (72.9%) from 12 countries reported: minimum dataset, standardized definition and availability of information. Completeness is observed in 25 publications (67.5%) in 15 countries; consistency and data management from 22 articles (59.4%) in 12 countries. Timeliness and security observed from 19 articles (51.3%) in 12 countries; reliability 18 articles (48.6%) in 10 countries. Validity observed in 15 articles (40.5%) in 12 Countries, compatibility from 12 papers (32.4%) in 6 countries. Confidentiality is from 10 articles (27%) in 5 countries, privacy from 6 articles (16.2%) from 2 countries. Comprehensive is reported by 4 articles (10.8%) from 3 countries, then integrity in 3 articles (8.1%), and strict in 2 articles (5.4%) from 2 countries.
As least virtue among the standards indicators, strict is only been observed in Japan and the EU; integrity is observed in Germany, EU and the US; followed by Comprehensiveness which is practically in Australia, Canada, EU and the US; then privacy which is also noticed only in Japan, EU and the US.
Table 1: List of the Papers standards observed
| S/N | Authors & Reference | Country / Year | Types of system | Standard observed | ||||||||||||||||||
| S1 | S2 | S3 | S4 | S5 | S6 | S7 | S8 | S9 | S10 | S11 | S12 | S13 | S14 | S15 | S16 | S17 | S18 | S19 | ||||
| 1 | Phyllis A. Wingo et al. [53] | US / 2005 | Chronic & Communicable diseases/ Active & Passive | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | |||||||||
| 2 | Oregon State Cancer Registry[54] | US / 2009 | Cancer registry
Web based |
√ | √ | √ | √ | √ | √ | √ | √ | √ | √ | |||||||||
| 3 | Herman Menck et al. [55] | US / 1994 | Cancer registries | √ | √ | √ | √ | √ | √ | √ | √ | |||||||||||
| 4 | Commission on Cancer. [56] | US / 2016 | Cancer registry | √ | √ | √ | √ | √ | √ | |||||||||||||
| 5 | ME McCuskey et al. [57] | US / 2012 | PBCR | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | |||||
| 6 | Laura A. McClure et al. [58] | US / 2016 | Cancer registry | √ | √ | √ | √ | √ | √ | √ | √ | √ | ||||||||||
| 7 | SK. Mohanty et al. [25] | US / 2008 | Cancer biobank | √ | √ | √ | √ | √ | √ | √ | √ | √ | ||||||||||
| 8 | AM. Marchevsky et al. [59] | US / 2005 | Thoracic
Mesothelioma Malignant |
√ | √ | √ | √ | √ | ||||||||||||||
| 9 | Jim Hofferkamp. [60] | US & Canada / 2008 | Cancer registries | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | |||||
| 10 | Bartha M. Knoppers et al. [61] | Canada / 2000 | Cancer surveillance | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | |||
| 11 | Paul Henry Yerrell et al. [62] | Australia / 2016 | Cancer registration
Integration Advanced Cancer Data System; (ACaDs) |
√ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | ||||||
| 12 | Graham G. Giles & Vicky Thursfield. [63] | Australia & New Zealand / 2004 | Cancer registries | √ | √ | √ | √ | √ | √ | √ | √ | |||||||||||
| 13 | Jerzy E. Tyczynski et al. [64] | EU / 2003 | European network of Cancer registries | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | |||||||
| 14 | Freddie Bray et al. [65] | France & Switzerland / 2015 | Population based Cancer registry | √ | √ | √ | √ | √ | √ | √ | √ | √ | ||||||||||
| 15 | Jacques Ferlay et al. [19] | France / 2014 | Cancer registry | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | ||||||
| 16 | O.M. Jensen et al. [66] | France / 1991 | Cancer registries | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | |||||||
| 17 | Joakim Dillner. [67] | Sweden / 2015 | Biobanks and cancer registries | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | |||||||||
| 18 | Hilde Langseth et al. [68] | Nordic / 2010 | Cancer registry & biobank. Web based | √ | √ | √ | √ | √ | √ | √ | √ | |||||||||||
| 19 | Holleczek Bernd and Alexander Katalinic. [69] | Germany / 2017 | Cancer registries
Web based / automated |
√ | √ | √ | √ | √ | √ | √ | √ | √ | ||||||||||
| 20 | A.G. Tafazzoli et al. [70] | Germany / 2002 | Cancer registry / decision support. Automated | √ | √ | √ | √ | √ | √ | √ | √ | |||||||||||
| 21 | ||||||||||||||||||||||
| 22 | ||||||||||||||||||||||
| 23 | ||||||||||||||||||||||
| 24 | ||||||||||||||||||||||
| 25 | ||||||||||||||||||||||
| 26 | ||||||||||||||||||||||
| 27 | Japanese Association of Cancer registries. [71] | Japan / 2010 | Cancer registry | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | |||||||
| 28 | Naoyuki Okamoto. [72] | Japan / 2008 | PBCR
Paper, system based |
√ | √ | √ | √ | √ | √ | √ | √ | √ | √ | |||||||||
| 29 | Takahiro Higashi et al. [73] | Japan / 2014 | HBCR | √ | √ | √ | √ | √ | √ | √ | √ | √ | ||||||||||
| 30 | Hamideh Salimzadeh et al. [47] | Iran / 2014 | Cancer Registry | √ | √ | √ | √ | √ | √ | √ | ||||||||||||
| 31 | Bhurgri Yasmin et al. [74] | Pakistan / 2002 | PBCR | √ | √ | √ | √ | √ | √ | |||||||||||||
| 32 | Rishika Banydeen et al. [4] | Caribbean / 2015 | Cancer registry | √ | √ | √ | √ | √ | √ | √ | ||||||||||||
| 33 | Yelda A. Leal et al. [5] | Cuba & Mexico / 2016 | Cancer registry | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | |||||||||
| 34 | Monica S. Sierra & David Forman. [75] | Central and South America / 2016 | Cancer registries | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | |||||||||
| 35 | Monica S. Sierra, et al. [76] | Colombia / 2016 | Cancer registry | √ | √ | √ | √ | |||||||||||||||
| 36 | Okabia M. N. [10] | Nigeria. / 2003 | Population Based Cancer registry | √ | √ | √ | √ | |||||||||||||||
| 37 | D. Maxwell Parkin, et al. [77] | Africa / 2014 | Cancer registries | √ | √ | √ | √ | √ | ||||||||||||||
| Key note: S1 = Basic data items; S2 = Standardized definition; S3 = Availability of information; S4 = Strictness; S5 = Accuracy; S6 = Timeliness; S7 = Completeness; S8 = Reliability; S9 = Data quality;
S10 = Integrity; S11 = Security; S12 = Confidentiality; S13 = Comprehensive; S14 = Privacy; S15 = Consistency; S16 = Data management; S17 = Comparability; S18 = Compatibility; S19 = Validity |
||||||||||||||||||||||
Table 2: Distribution of standards observed by countries
| s/n | List of Standards | Sweden | Australia | US | France | Japan | Nordic | EU | Canada | France /Switzerland | Germany | Pakistan | Martique | Cuba / Mexico | Iran | Nigeria | Africa | Central and South America | Colombia | New Zealand |
| 1 | Common basic set of data items | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | ||||||
| 2 | Standardized definition | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | |||||
| 3 | Availability of information | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | ||||
| 4 | Strictness | √ | √ | |||||||||||||||||
| 5 | Accuracy | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | ||
| 6 | Timeliness | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | ||||||||
| 7 | Completeness | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | ||||
| 8 | Reliability | √ | √ | √ | √ | √ | √ | √ | √ | √ | ||||||||||
| 9 | Data quality | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | |||
| 10 | Integrity | √ | √ | |||||||||||||||||
| 11 | Security & protection | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | |||||||||
| 12 | Confidentiality | √ | √ | √ | √ | √ | √ | |||||||||||||
| 13 | Comprehensive | √ | √ | √ | ||||||||||||||||
| 14 | Privacy | √ | √ | |||||||||||||||||
| 15 | Consistency | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | |||||||
| 16 | Data management | √ | √ | √ | √ | √ | √ | √ | √ | |||||||||||
| 17 | Comparability | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ |
| 18 | Compatibility | √ | √ | √ | √ | √ | ||||||||||||||
| 19 | Validity | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ |
DISCUSSION
With the establishment and development of information and computer technology, data accessibility has increased and can now be made available online in much more detail than was possible. However, data of cancer burden are yet to be fully accessible [12, 78-79].
On this review, we focus on the standards indicators found available striving to ensure quality and availability of reliable cancer data. The available standards indicator we focused on, are those we found in the literature. Many of the countries in which standards are found in this research are developed nations. We categorized the observed standards into five different levels: poor, low, middle, good, and very good. One to four standards observed represent poor category, five to eight represent low category, nine to twelve as middle level category, thirteen through sixteen symbolize good category, and seventeen to nineteen stand for very good category level.
Standards for cancer registry among the review registry in this study was relatively high, the proportion range from 2 publications (5.4%) under poor category, 9 publications (24.3%) under low category, 21 articles (56.7%) in middle level, and 5 publications (13.5%) within the good level category. Though, no single reviewed article reported under very good category level; merging the articles published from similar country permit the US into the very good category level (Figure 2).
The disparities among regions on the basis of percentages are explained. North America shows high, which have 16 standards observed (84.2%) in single article. 13 standards (68.4%) are observed from Oceanic region in single publication, as well as from the European Union. 12 standards (63.1%) are observed from Asia. 10 standards (52.6%) from Central and South America, including Caribbean region. And 5 standards (26.3%) are in operative in Africa (Figure 3). Although the indices vary among registries [34, 80-81], little variation is in reality between the North American countries. Reason might be due to long standing registry organization and the effort of North American Association of Central Cancer Registries (NAACCR) coordination’s for cancer registry standards setters; that has been in existence since 1987 [15]. In Europe, European Network of Cancer Registries (ENCR) and the Association of Nordic Cancer Registries are working to ensure uniformity of standards and promote best practice within the member states [11, 82], although there is call on European cancer registries to reduce the erroneous by reaching the consensus on combine standards [83].
Partial variation among Oceanic countries was noticed, in Australia and New Zealand (ANZ) entire populations are covered as registration for cancer is mandatory by law for the past 30 years [63]. In recent years, just French Polynesia cancer data has not been included in CI5 volume X from the region [19].
In Asia, although two supra national organizations are in operation in Western Asia: the Middle East Cancer Consortium (MECC) which established Cancer Registry Project (CRP), and the Gulf Center for Cancer Registration [16]. There has been no similar supra-national body yet in South Asia, South East Asia, and North East Asia. Malcolm A. Moore et al., report that, progress to establish Asian Cancer Information Network in North-East Asia by Japan is in place, and similarly, Thai Cancer institute provides various program to support cancer registries within the South and the South-East Asian countries[16]. Major variability among Asian registries was noticed, where registries from Japan show significant data quality and several publications on cancer as stated by [16, 84]. This should be as a result of having strong policy and Japanese Association of Cancer Registries[71].
In Iran and Pakistan, publications about quality evaluation of national cancer registry system [47], and implications of registry data for the national plan along with reports on quality control have appeared in literature. Many nations are making effort to lunch national program for cancer registry. Iran Center for Disease Control and Prevention, Ministry of Health and Medical Education established passive registration since around 1999 [47], and National Program of Cancer Registry by Ministry of Health of China established 2008 [85]; several countries in the same region such as Armenia, Azerbaijan, Georgia, Tajikistan, Turkmenistan, Kazakhstan, and Uzbekistan has no data or publications related to cancer registry [16] and need for health care reform are explored [36, 86].
Caribbean, Central and South American region experience huge variation of standards among registries and data quality, and differences in completeness cannot be taking into account [4, 76]. Despite the fact that efforts are in place to promote and enhance the number of registries, as Jamaica, Puerto Rico, Martinique, Cuba, and Colombia have contributed quality data for World Health Organization (WHO) publications [4-5], most of the countries in this region are lacking cancer data at national level, even the quality data are classified based on three level (low, medium & high), and some registries depend on using ENCR recommendations [75].
Like other developing nations, it is similar in Africa. With all the efforts of WHO to develop and promote National Cancer Control Programmes, yet standards for cancer registration cannot be determined where registries operate at different levels (local, regional and national), and policy on cancer control is lacking [10, 77]. The available cancer data within the African countries were rated to be at low quality in some countries (i.e. Egypt and South Africa) and medium quality in other part, as only about 1% registries cancer data out of 11% population covered by population-based cancer registries met the IARC quality criteria for inclusion in CI5 [10, 87], and the variation of coverage vary between 2% to about 90% with serious bias on rural to urban [13].
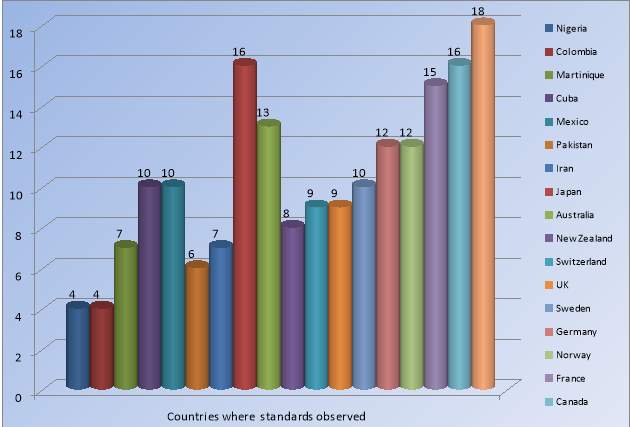
Figure 2: The disparity of standards observed among different countries
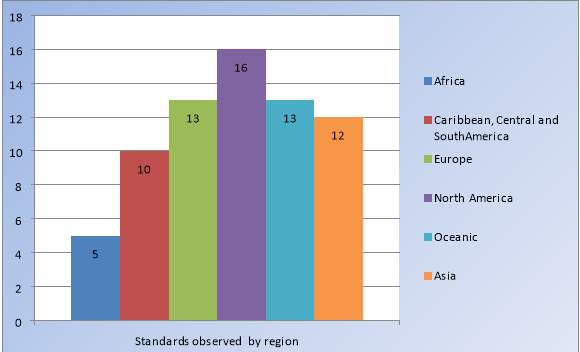
Figure 3: The disparity of standards observed under the different regions
Those countries with higher standards are more of developed. By law, reporting cancer cases is mandatory in North America, and most part of Europe, including Oceanic. Consensus by network among different registries nearly promotes uniform standards from those regions with high standards observed. NAACCR activities show numerous organization in promoting uniform data standards, and other related registry program [16, 18].
Looking at this fact, when compared with the proportion of registry population coverage, it demonstrate huge disparity among countries in Africa, Asia, and Central and South American regions [35] where government policy on cancer registration is yet to be mature in some countries [16]. Our review discovered that this disparity is as a result of lack of multi-partner overseeing organization [88] that can promotes, coordinates and ensure uniform standards for maintaining cancer registry activity. This proves the finding of Crocker-Buque et al,[13] where 19 (73%) of 26 registries identified, failed to meet above five of the fifteen quality criteria in sub-Sahara Africa [13].
CONCLUSION
Without observing standards at registry level, National Control Program cannot access quality data from the registry for cancer control plan. While admitting that the most improved countries on cancer registration such as Canada and the US haven’t observed all the standards under this review, those countries that don’t have central coordinator, have less standardization rather than those that has, and high prevalence of cancer has been predicted from those countries. In order to facilitate the standards at different level of cancer registry, the justification of NAACCR and that of ENCR analogy as umbrella body is clearly desired especially in developing countries, political willingness will not be overemphasize in ensuring legislative patronage for central management.
The purpose of this research was to identify, access, and details any available standards that can improve the cancer registration process, as well as other disease registries, and data quality. These were achieved. The study goals were to figure countries where high and low standards are observed and the proportion between the standards and quality of data under the ascertain spot; these were also achieved. Quality data allows for monitoring change in incidence over time. Our conclusion features the need for common multi-partner consensus organization at sub-national, national and regional level among public and private health agencies. More research are needed in order to explored additional data quality indicators, so as availability and quality of cancer data will improve.
Suggestions
It is recommended that, the following suggestions should be considered to adhere to standards and data quality in the cancer registries:
- Multidisciplinary committee on cancer (at local registry operational and national level)
- National Association of Cancer Registries
- Transnational Committee on Cancer
- Regional Network for Cancer Registration
- Periodic meeting to revise the procedures
- Cancer Registrars training programs
- Conferences on Cancer quality management program
- Establishment and review of quality control program to checkmate the registration procedure and develop reward for best registrar and or registry
- Regional guideline in line with national or local registration guidelines
- Ensure registry data are published to guarantee success
REFERENCES
1. Hadji, M., et al., Challenges to promoting population-based cancer registration in Iran: a workshop report. Asian Pac J Cancer Prev, 2013. Vol 14(10): p. Pages: 6189-93.
2. Strasser-Weippl, K., et al., Progress and remaining challenges for cancer control in Latin America and the Caribbean. The Lancet Oncology, 2015. Vol 16(14): p. Pages 1405-1438.
3. Jedy-Agba, E., et al., Cancer incidence in Nigeria: a report from population-based cancer registries. Cancer Epidemiology, 2012. Vol. 36(5): p. e271-e278.
4. Banydeen, R., et al., Advancing cancer control through research and cancer registry collaborations in the Caribbean. Cancer control: journal of the Moffitt Cancer Center, 2015. Vol. 22(4): p. Pages. 520.
5. Leal, Y.A., et al., The importance of registries in cancer control. salud pública de méxico, 2016. 58(Vol. 2): p. Pages 309-316.
6. Anwar, W. and D.N. Boulos, Cancer registries in Africa: an emerging need. Journal africain du cancer/African Journal of Cancer, 2012: p. 1-2.
7. Bah, E., et al., 20-years of population-based cancer registration in hepatitis B and liver cancer prevention in the Gambia, West Africa. PLoS One, 2013. 8(9): p. e75775.
8. Garba, S.M., et al., P0190Colorectal cancer in Niger: An analysis of the Niger Cancer Registry Data. European journal of cancer, 2014. Vol. 50(4): p. e63.
9. Steliarova-Foucher, E., et al., The European Cancer Observatory: A new data resource. Eur J Cancer, 2015. 51(9): p. 1131-43.
10. Okobia, M.N., Cancer Care in sub-Saharan Africa–Urgent Need for Population–based Cancer Registries. Ethiopian Journal of Health Development, 2003. 17(2): p. 89-98.
11. Registries, E.N.o.C., et al., Standards and guidelines for cancer registration in Europe: the ENCR recommendations. 2003: International Agency for Research on Cancer.
12. Jedy-Agba, E.E., et al., Developing national cancer registration in developing countries – case study of the Nigerian National System of Cancer Registries. Frontiers in public health, 2015. Vol 3.
13. Crocker-Buque, T. and A.M. Pollock, Appraising the quality of sub-Saharan African cancer registration systems that contributed to GLOBOCAN 2008: a review of the literature and critical appraisal. Journal of the Royal Society of Medicine, 2015. 108(2): p. 57-67.
14. Bray, F. and D.M. Parkin, Evaluation of data quality in the cancer registry: principles and methods. Part I: comparability, validity and timeliness. European journal of cancer, 2009. 45(5): p. 747-755.
15. Thornton, M., Standards for Cancer Registries Volume II: Data Standards and Data Dictionary,
Sixteen Edition, Version 12.2 Springfield, IL: North American Association of Central Cancer Registries. North American Association of Central Cancer Registries, Inc. (NAACCR), 2012. II(Version 12): p. 540.
16. Moore, M.A., et al., Establishment of an Asian Cancer Registry Network: problems and perspectives. Asian Pac J Cancer Prev, 2008. 9(4): p. 815-832.
17. Anttila, A., et al., Towards better implementation of cancer screening in Europe through improved monitoring and evaluation and greater engagement of cancer registries. Eur J Cancer, 2015. 51(2): p. 241-51.
18. White, M.C., et al., The history and use of cancer registry data by public health cancer control programs in the United States. Cancer, 2017. 123(S24): p. 4969-4976.
19. Forman, D., et al., Cancer Incidence in 5 Continents (CIV) Vol X. IARC WHO IARC Scientific Publications No. 164. Lyon: International Agency for Research on Cancer, 2014. Vol. X(No. 164): p. 1436.
20. Andersen, M.R. and H.H. Storm, Cancer registration, public health and the reform of the European data protection framework: Abandoning or improving European public health research? Eur J Cancer, 2015. 51(9): p. 1028-38.
21. Makinde, O.A., A. Azeez, and W. Adebayo, Potential use cases for the development of an electronic health facility registry in Nigeria: Key informant’s perspectives. Online J Public Health Inform, 2016. 8(2): p. e191.
22. Dimitrova, E., et al., Trends and patterns in cancer incidence in Czechoslovakia, 1968-1985. Neoplasma, 1989. 36(2): p. 245-255.
23. Alshammari, A.O. and N.F. Abernethy. Variability among public health systems informs data standards for electronic case reporting. in In Informatics, Health & Technology (ICIHT), International Conference on. 2017: IEEE.
24. Sariyar, M., et al., A practical framework for data management processes and their evaluation in population-based medical registries. Inform Health Soc Care, 2013. Vol. 38(2): p. 104-19.
25. Mohanty, S.K., et al., The development and deployment of Common Data Elements for tissue banks for translational research in cancer – an emerging standard based approach for the Mesothelioma Virtual Tissue Bank. BMC Cancer, 2008. Vol. 8: p. 91.
26. Silcocks, P., P. Needham, and F. Hemsley, Audit of prostate cancer: lessons learnt for current clinical practice, surrogates for quality of care and standardisation and quality assurance. Public health, 1999. Vol. 113(4): p. 161-164.
27. David Berz, M., K.E. Faricy-Anderson, and A. Birnbaum, Do race and ethnicity predict survival in metastatic non-small cell lung cancer? Medicine and Health Rhode Island, 2010. 93(10): p. 299.
28. Navarro, C., et al., Population-based cancer registries in Spain and their role in cancer control. Ann Oncol, 2010. 21 Suppl 3: p. iii3-13.
29. Bianconi, F., et al. Cancer registry and information technology: a new management system for integrating cancer registry and oncology departments. in Health Care Management (WHCM), IEEE Workshop on 18 February, 2010. 2010: IEEE 2010.
30. Nnebue, C.C., et al., Awareness and knowledge of disease surveillance and notification by health-care workers and availability of facility records in Anambra state, Nigeria. Nigerian medical journal: journal of the Nigeria Medical Association, 2012. 53(4): p. 220.
31. McLaughlin, J.R., et al., Cancer incidence registration and trends in Ontario. European Journal of Cancer and Clinical Oncology, 1991. 27(11): p. 1520-1524.
32. Jayant, K., et al., Rural cancer registry at Barshi, Maharashtra and its impact on cancer control. Natl Med J India, 2010. 23(5): p. 274-7.
33. Gliklich, R.E. and N.A. Dreyer, Registries for Evaluating Patient Outcomes: Developing Evidence to Inform Decisions about Effectiveness (DEcIDE). Agency for Healthcare Research and Quality, 2010.
34. Zanetti, R., et al., Completeness and timeliness: Cancer registries could/should improve their performance. Eur J Cancer, 2015. 51(9): p. 1091-8.
35. Bray, F., et al., Cancer Incidence in Five Continents: Inclusion criteria, highlights from Volume X and the global status of cancer registration. International Journal of Cancer, 2015. 137(9): p. 2060-2071.
36. Adambekov, S., et al., Health challenges in Kazakhstan and Central Asia. Journal of Epidemiology and Community Health, 2015: p. Pages: 206 – 251.
37. Corley, B., et al., Measuring the Effect of Improved Medical Facilities and Focused Training on Data Quality and Completeness: An Example from the Gharbiah Population-Based Cancer Registry, Egypt. J Registry Manag, 2015. 42(3): p. 86-90.
38. Cuervo, L.G., et al., Evaluation of institutional cancer registries in Colombia. Revista Panamericana de Salud Pública, 1999. 6(3): p. 202-206.
39. ASCP, A.M., Abstracts from the Society for Clinical Trials Annual Meeting, Miami, May 21-23, 2012, in Clinical Trials. 2012, Sage Publications Ltd.: London. p. 450-554.
40. Orem, J. and H. Wabinga, The roles of national cancer research institutions in evolving a comprehensive cancer control program in a developing country: experience from Uganda. Oncology, 2009. 77(5): p. 272-280.
41. Loane, M. and R. Wootton, A review of guidelines and standards for telemedicine. Journal of telemedicine and telecare, 2002. 8(2): p. 63-71.
42. Schreiner-Karoussou, A., Review of image quality standards to control digital X-ray systems. Radiation protection dosimetry, 2005. Vol. 117(1-3): p. Pg 23-25.
43. Awaysheh, A., et al., A review of medical terminology standards and structured reporting. Journal of Veterinary Diagnostic Investigation, 2017: p. Pages 9.
44. Strömbäck, L., D. Hall, and P. Lambrix, A review of standards for data exchange within systems biology. Proteomics, 2007. 7(6): p. 857-867.
45. Shortliffe, E.H. and J.J. Cimino, Biomedical informatics: computer applications in health care and biomedicine. 2013: Springer Science & Business Media.
46. Crocetti, E., et al., Defining the roadmap towards revision of European Network for Cancer Registries (ENCR) coding standards and training for cancer registries, in The European Network of Cancer Registries (ENCR) and the Joint Research Centre (JRC) workshop. 2015, EU publications: Italy. p. 38.
47. Modirian, M., et al., Quality evaluation of national cancer registry system in iran: study protocol. Archives of Iranian medicine, 2014. 17(3): p. 193.
48. Shahmoradi, L., et al., A comprehensive model for executing knowledge management audits in organizations: a systematic review. The health care manager, 2015. 34(1): p. 28-40.
49. Stevens, W., et al., Literature Review for the Project Identification of Barriers to the Early Diagnosis of People with Lung Cancer within Primary Care and Description of Best Practice Solutions, F. Practice, Editor. 2009, Northern Cancer Network: Auckland. p. Pg. 107.
50. Forrest, L.F., et al., Socioeconomic inequalities in lung cancer treatment: systematic review and meta-analysis. PLoS Med, 2013. 10(2): p. e1001376.
51. Corsini, N., et al., Cancer survivorship monitoring systems for the collection of patient-reported outcomes: a systematic narrative review of international approaches. J Cancer Surviv, 2017. 11(4): p. 486-497.
52. Janati, A., et al., Communicable disease reporting systems in the world: a systematic review article. Iranian journal of public health, 2015. 44(11): p. 1453.
53. Wingo, P.A., et al., A national framework for cancer surveillance in the United States. Cancer Causes & Control, 2005. 16(2): p. 151-170.
54. Human Services, D., Cancer Reporting Standards Volume I: Oregon State Cancer Registry. 2009, Oregon Department of Human Services: Portlan, Oregon. p. Pg.216.
55. Menck, H. and C.R. Smart, Central Cancer Registries: Design, Management, and Use. 1994, Chicago, Illinois: Harwood Academic; CRC Press.
56. Cancer, A.C.o.S.C.o., Facility Oncology Registry Data Standards FORDS (Revised for 2016). Chicago, IL, 2016: p. 515.
57. McCusker, M.E., et al., Feasibility of linking population-based cancer registries and cancer center biorepositories. Biopreserv Biobank, 2012. 10(5): p. 416-20.
58. McClure, L.A., et al., Linking the National Health Interview Survey with the Florida Cancer Data System: A Pilot Study. Journal of registry management, 2016. 43(1): p. 16-22.
59. Marchevsky, A.M., et al., Thoracic Mesothelium
Protocol applies to malignant thoracic mesothelioma. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition, 2005.
60. Hofferkamp, J., Standards for cancer registries volume III: standards for completeness, quality, analysis, management, security and confidentiality of data. Springfield, IL: North American Association of Central Cancer Registries (NAACCR). 2008.
61. Knoppers, B.M., et al., Legal regulation of cancer surveillance: Canadian and international perspectives. Health Law Journal, 2000. 8: p. 1-94, i-xxxiv.
62. Yerrell, P.H., et al., Cancer Data and Aboriginal Disparities (CanDAD)-developing an Advanced Cancer Data System for Aboriginal people in South Australia: a mixed methods research protocol. BMJ Open, 2016. 6(12): p. e012505.
63. Giles, G.G. and V. Thursfield, Cancer statistics: everything you wanted to know about the cancer registry data but were too afraid to ask. ANZ journal of surgery, 2004. 74(11): p. 931-934.
64. Regisries, E.N.o.C., et al., Standards and guidelines for cancer registration in Europe: the European Network of Cancer Registries (ENCR) recommendations. 2003, International Agency for Research on Cancer.
65. Bray, F., et al., Planning and developing population-based cancer registration in low-and middle-income settings. 2014: IARC (International Agency for Research on Cancer).
66. Jensen, O.M., Cancer registration: principles and methods. Vol. 95. 1991: International Agency for Research on Cancer (IARC).
67. Dillner, J., A basis for translational cancer research on aetiology, pathogenesis and prognosis: Guideline for standardised and population-based linkages of biobanks to cancer registries. Eur J Cancer, 2015. 51(9): p. 1018-27.
68. Langseth, H., et al., Ensuring quality in studies linking cancer registries and biobanks. Acta Oncol, 2010. 49(3): p. 368-77.
69. Holleczek, B. and A. Katalinic, Toward a comprehensive cancer registration in Germany. Eur J Cancer Prev, 2017.
70. Tafazzoli, A.G., et al., Integrated decision support in a hospital cancer registry. Artif Intell Med, 2002. 24(3): p. 243-55.
71. Registries, J.A.o.C., Cancer Registry in Japan. JACR, 2010: p. 25.
72. Okamoto, N., A history of the cancer registration system in Japan. International journal of clinical oncology, 2008. 13(2): p. 90-96.
73. Higashi, T., et al., The national database of hospital-based cancer registries: a nationwide infrastructure to support evidence-based cancer care and cancer control policy in Japan. Jpn J Clin Oncol, 2014. 44(1): p. 2-8.
74. Bhurgri, Y., et al., Large-scale pathology-based cancer data–a reflection of population-based cancer data. Pathol Oncol Res, 2002. 8(1): p. 62-7.
75. Sierra, M.S. and D. Forman, Cancer in Central and South America: Methodology. Cancer Epidemiology, 2016. 44: p. S11-S22.
76. Sierra, M.S., et al., Cancer patterns and trends in Central and South America. Cancer Epidemiology, 2016. 44: p. S23-S42.
77. Parkin, D.M., et al., Cancer in africa 2012. Cancer Epidemiology and Prevention Biomarkers, 2014. 23(6): p. 953-966.
78. Allemani, C., et al., Global surveillance of cancer survival 1995–2009: Analysis of individual data for 25 676 887 patients from 279 population-based registries in 67 countries (CONCORD-2). The Lancet, 2015. Vol. 385(9972): p. Pg. 977-1010.
79. Fahey, R.L., Evaluation of the System Attributes of Timeliness and Completeness of the West Virginia Electronic Disease Surveillance System – National Electronic Disease Surveillance System Based System, in School of Public Health. 2015, Walden University: West Virginia. p. 146.
80. Boscoe, F.P. and C. Sherman, On socioeconomic gradients in cancer registry data quality. Journal of Epidemiology & Community Health, 2006. 60(6): p. 551-551.
81. Siesling, S., et al., Uses of cancer registries for public health and clinical research in Europe: results of the European Network of Cancer Registries survey among 161 population-based cancer registries during 2010–2012. European journal of cancer, 2015. 51(9): p. 1039-1049.
82. Weir, H.K., et al., Population-based cancer survival (2001 to 2009) in the United States: Findings from the CONCORD-2 study. Cancer, 2017. 123(S24): p. 4963-4968.
83. Crocetti, E., et al., The need for a rapid and comprehensive adoption of the revised European standard population in cancer incidence comparisons. European Journal of Cancer Prevention, 2016. 25(5): p. Pg. 447.
84. Zanetti, R., et al., The prevalence of cancer: A review of the available data. Tumori, 1999. Vol. 85(5): p. Pg. 408-413.
85. Xu, T., Chinese Anti-Cancer Association as a non-governmental organization undertakes systematic cancer prevention work in China. Chinese Journal of Cancer Research, 2015. 27(4): p. 423.
86. Moore, M.A., Cancer control programs in East Asia: evidence from the international literature. J Prev Med Public Health, 2014. 47(4): p. 183-200.
87. Jemal, A., et al., Cancer burden in Africa and opportunities for prevention. Cancer, 2012. 118(18): p. 4372-4384.
88. Wild, C.P., Cancer control: a reminder of the need for a balanced approach between prevention and treatment. EMHJ, 2014. 20(6).
Cite This Work
To export a reference to this article please select a referencing stye below:
Related Services
View all


Related Content
All TagsContent relating to: "Cancer"
Cancer is a disease in which cells grow or reproduce abnormally or uncontrollably. Cancerous cells have the potential to spread to other areas of the body in a process called metastasis.
Related Articles

DMCA / Removal Request
If you are the original writer of this dissertation and no longer wish to have your work published on the UKDiss.com website then please: