Epidemiology of Cronobacter Sakazakii
Info: 3031 words (12 pages) Dissertation
Published: 16th Dec 2019
Tagged: Medicine
Abstract
Cronobacter sakazakii once known as Enterobacter sakazakii is a new emerging pathogen that is responsible for various neonatal conditions such as meningitis, bacteremia and necrotizing enterocolitis in infants. Majority of the neonatal infections caused by C. sakazakii have been linked to the use of infant formula powder and some of the strains are able to survive and withstand dry conditions for over two years. C. sakazakii is not only present in infant formula it can also be found in a variety of foods and water supply. This pathogen is also present in different environments which includes houses and hospitals. C. sakazakii can cause serious infections in humans, therefore strict control measures are to be implemented to minimize or eliminate contamination at all levels. These measures include not only the safe handling of food but also legislative guidelines set up by the appropriate authorities.
Key words: Cronobacter sakazakii, Enterobacter sakazakii, infant formula powder, neonatal, control measures.
Introduction
C. sakazakii previously known as Enterobacter sakazakii belongs to class of Gram-negative bacteria that are found in our environment and can thrive in extremely dry conditions. However, the natural habitat of C. sakazakii is not yet known. This pathogen has been identified in various food items specially in dry foods which includes skim milk powder, infant formula powder, starches and herbal teas. C. sakazakii is also present in wastewater. Infections caused by C. sakazakii are not very common but can be extremely dangerous for infants. Elderly and people with immunocompromising cases could also be highly susceptible to C. sakazakii infections (Mullane et al., 2008).
C. sakazakii is capable of various infections but the symptoms of infection can be different for individuals depending on the area of infection and the age. Usually severe meningitis and sepsis are caused by C. sakazakii in infants who are less than twelve months old. Seizures can be seen in some infants with the infection. Infarcts or abscesses (swelling) may occur in infants with severe meningitis (Mullane et al., 2008). Meningitis due C. sakazakii is mostly seen in infant’s whore are less than two months old. Other serious complications such as hydrocephalus may also occur. Mortality rate of infants caused by meningitis from C. sakazakii is a staggering 40% which is very high (Carol Iversen et al., 2007). Even though infants are the most vulnerable to C. sakazakii infections, this pathogen could cause infections in both urinary tract and wounds in people of all different ages. Infections in blood streams can occur in immunocompromised individuals and people of old age from C. sakazakii. C. sakazakii has also been found in respiratory secretions of patients that are undertaking ventilation (mechanical) (Carol Iversen et al., 2007). Although in these cases C. sakazakii are usually found settling in the respiratory tract and do not show any activity of infection. Stool samples obtained from asymptotic people has shown presence of C. sakazakii. Infections caused by C. sakazakii are rare, the Centre for disease control and prevention in USA states that they receive about four to six reported cases in infants every year. Since reporting of cases are not mandatory in USA, other than for states like Minnesota the amount of infection in USA caused by C. sakazakii is not properly determined. Infections caused by C. sakazakii are diagnosed by using a laboratory culture, in case of detection of the pathogen from the culture physicians are encouraged to notify the hospitals. If an infant is believed to have sepsis or meningitis caused by C. sakazakii the infant must be put through a series of clinical tests which includes evaluation of blood, urine and cerebrospinal fluid cultures. Sepsis should be treated with empiric therapy as soon as possible. In recent times cases of multi drug resistant strains have been reported therefore antimicrobial sensitive patterns displayed by Cronobacter should be observed (Carol Iversen et al., 2007). Brain complications which includes swelling can be observed using studies from brain imaging. Treatments are not necessary if individuals have colonized C. sakazakii but show no signs of infection. However, cases of wound and urinary tract infection must be attended to as soon as possible with antibiotics. Consumption of infant formula powder (reconstituted) has shown a significant association with infants infected with C. sakazakii. Investigations carried out during several outbreaks have shown that the infant formula powder had been contaminated with C. sakazakii during processing in the factory and/or when the packaged formula was opened later inside a consumer’s house or another area. Since C. sakazakii is found in the natural environment the infection could occur from multiple sources (Chap et al., 2009). However, no reported cases of C. sakazakii infection from person to person exist even though other types of bacteria generally spread from contact of one person to the other. Infant formula powder is not sterilized, manufacturing of infant formula does not utilize any method which could completely sterilize the powder. In the processing facility C. sakazakii could enter the infant formula powder via an already contaminated raw ingredient (Chap et al., 2009). Contamination could also occur if the powder touches a surface that is already contaminated with C. sakazakii. Contamination can occur at any place if the infant formula powder container is opened, C. sakazakii can get into the powder via a spoon if the spoon was left on a contaminate surface and later it was put into the powdered milk. Also, an infant can get infected with C. sakazakii if a contaminated feeding bottle or contaminated water is used to prepare the infants drinking formula. Due to the gravity of problems caused by C. sakazakii the International Commission for Microbiological Specifications for food has declared C. sakazakii as a danger for specific groups of people. Because of this C. sakazakii falls under the category of pathogens such as Clostridium botulinum (Type A), Cryptosporidium parvum and Listeria monocytogenes which are very common. Compared to elderly population and individuals with immunosuppressed conditions, infants are the most vulnerable and commonly affected groups specially infants in hospitals that are under neonatal intensive care who are fed with formula powder are at high risk, therefore FAO/WHO which is the CODEX Alimentarius committee on food hygiene has undergone revision for the suggested international code of hygiene practices for foods for infants and children and thereby they have created a risk profile for C. sakazakii (Carol Iversen & Forsythe, 2004).
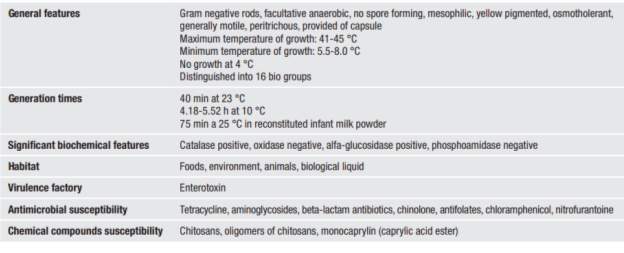
Table 1 Characteristic features of E. sakazakii
Epidemiology
Infections from C. sakazakii can occur in any age group. However, infants under the age of twelve months are the most common subjects. Statistics shows that in this group infants who are under neonatal intensive care, premature born after than thirty-six weeks old, immunodeficient infants, underweight infants and infants of mother with HIV positive are the most likely to be infected with C. sakazakii (Baumgartner, Grand, Liniger, & Iversen, 2009). The cause of this is that the infants are fed with powdered formula which can be contaminated with C. sakazakii. Infant formula powder is the main carrier of the pathogen. If an adult is infected only about fifty percent of the patients go through severe illness. And even if it is the illness is serious no cases of meningitis have been reported. Also in most severe cases, the mode of transmission of the microorganisms is not clearly known (Friedemann, 2007). Even though the incidence of infections is very low over the past few years the number of cases have slightly increased. Global statistics show that the number of infected cases are less than sixty. However, several other factors should be taken into consideration when looking at the number of cases because some countries do not have a system in place for reporting all incidences and not every laboratory clinical analysis does research on C. sakazakii. Therefore, we may be underestimating the number of infections caused by C. sakazakii. Death caused due to infection from C. sakazakii has gone over fifty percent in the past few years, however in recent years that number has come down to around twenty percent. Twenty percent is still a high number and the reported cases could be categorized into two major groups. The two groups are sporadic and epidemic. In 1961 2 cases of meningitis caused by C. sakazakii were reported, they were the first (Drudy, Mullane, Quinn, Wall, & Fanning, 2006). Back then C. sakazakii was known as Enterobacter cloacae. Later more and more cases related to C. sakazakii was reported globally. In the recent years there has been an increase in the number of cases reported. Advanced diagnostic methods and high number of infants at risk may have contributed to the number of cases reported (Carol Iversen & Forsythe, 2004).
Five cases of infections with C. sakazakii were reported from a pediatric unit in France during October to December of 2004 (Joseph & Forsythe, 2011). Two of the reported cases were fatal and during the same time another five people were identified with colonies in their intestines. Later it was found out that these infants were give infant formula powder infected with C. sakazakii. These incidences caused a lot of problems in many European countries. Some countries for example Ireland decided to stop the use of infant formula even though the infant milk powder suspected to have C. sakazakii was only sold in France and Algeria. New Zealand also had an infected case of C. sakazakii during the same period of time. However, this infection caused by C. sakazakii lead to the death of an infant who was in the hospital. Like the earlier cases this infant was fed with infant formula too, which was responsible for the transmission of the microorganism (Joseph & Forsythe, 2011). A case was reported in India back in 2006, an infant who was two months old had bacteremia caused by C. sakazakii in a medical care center. The infection was believed to be nosocomial. However, the mode of transmission but it was believed that it came from the hospital itself. Another case of C. sakazakii infection was reported in Spain. The infection occurred in 2007 at pediatric unit to an underweight premature baby. It was reported that the infant got neonatal sepsis from C. sakazakii. Even though infant formula was not given to the baby, liquid formula and breast milk was fed to the infant. How the infant was infected with C. sakazakii was unclear (Joseph & Forsythe, 2011).
Powdered infant formula (PIF) and C. sakazakii
PIF ca get contaminated with C. sakazakii at any point of the production process inside the manufacturing facility before the product is distributed. Contamination can also occur outside of the manufacturing plant once the consumers have opened the container of PIF. Contamination can occur at any stage when the formula is mixed with contaminated water or comes in contact with utensil and contaminated surfaces during preparation (Drudy et al., 2006). During feeding use of contaminated bottles with enteral tubing that has biofilms. Poor storage conditions such as leaving the PIF at room temperature for long periods of time could also result in contamination (Drudy et al., 2006).
It is believed that intrinsic contamination occurs at the stage after pasteurization of PIF has occurred. Because reconstituting PIF using hot water drastically reduces C. sakazakii. The PIF can get contaminated via the raw materials used for production of PIF which are not subjected to previous heat treatment (Friedemann, 2007). Proper pasteurization methods help reduce the amount of Cronobacter spp. The levels are typically low in most PIF products that are contaminated. The level is not more than one colony forming unit per gram
PIF contamination can occur in the later stages of the manufacturing process which is after pasteurization. Contaminating is common around the packaging stages of the finished product. C. sakazakii show resistance to drying (desiccation) and osmosis stress, these properties make this microorganism to contaminate and thrive in PIF (Friedemann, 2007). C. sakazakii contains an outer capsule composed of carbohydrates (heteropolysaccharides) which enables the pathogen to withstand osmotic desiccation. Therefore C. sakazakii can live up to more than two years in the PIF environment. However other pathogens with capsules have a short life cycle and are less like to be disease causing. C. sakazakii can also withstand acidic environments which means they are capable of surviving in the stomach of humans (human stomachs have low pH). C. sakazakii produce enterotoxins that make the microorganism resistant to heat, therefore it can withstand the pasteurization process (C Iversen, Lane, & Forsythe, 2004). C. sakazakii can travel from the intestine walls of humans and enter the blood brain barrier because the process is facilitated by an endotoxin that it produces. This endotoxin contains complex lipo-polysaccharides which gives C. sakazakii the ability to withstand heat and remain alive for longer time in PIF (reconstituted). Usually sialic acid is added to PIF because fortification of PIF with sialic acid helps infant brain growth. However, C. sakazakii is able to utilize the sialic acid for growth thus making it viable in the PIF (C Iversen et al., 2004). C. sakazakii has the ability to form biofilms. Biofilms make the microorganism resistant to disinfectants. Unlike other types of pathogenic species C. sakazakii biofilms have a high cell density making it resistant to environment stressors. Contaminated PIF (reconstituted) fed to infants via tubes can cause C. sakazakii to form colonies inside the tube. With time, these biofilms from these colonies start shedding cells, these cells can enter infants and cause infections (Nazarowec‐White & Farber, 1997).
Control and Prevention
To minimize the risk of C. sakazakii contamination PIF proper information on food manufacturing practices are to be provided in the manufacturing and handling stages. Precautions and guidelines should be set up in hospitals when mixing PIF to be fed to infants. Countries such as USA have their hospitals use guidelines set up by the American Dietetic Association when handling the preparation of infant milk formula. These guidelines state that PIF should be prepared in specific areas that are sterile and also the proper aseptic preparation techniques (Control & Prevention, 2002). Reconstituted milk is to be store at temperatures between three to four degrees Celsius, and that it should not be left for more than four hours after reconstituting. Utensils required for preparation of PIF must be disinfected. Milk formula should be reconstituted with hot water of temperatures more than 70 degrees Celsius. However, there are no precise testing methods or recommendations for C. sakazakii. Both the World Health Organization and Food and Agricultural Organization have set up guidelines for hospitals and homes when it comes to preparing PIF of infants. These guidelines/recommendations are stated above and mostly apply when preparing formula for infants for the first two months. Infants are at the highest risk of infection in their first 2 months (Control & Prevention, 2002).
Attention has to be given to enteral feeding tubes used to feed neonates in neonatal intensive care units (Beuchat et al., 2009). Formation of biofilms in these tubes can cause infections in the infants and hospital authorities have to take proper caution when using these tubes to feed neonates. Proper sterilization methods have to be put in place. Improvements of regulatory standards are necessary in the manufacture of infant foods. Good environment monitoring programs, use of GMP (good manufacturing practices) and HACCP (hazard analysis and critical control points) has to be put in place to minimize microbial contamination. PIF labelling must be improved with clear instruction on reconstituting the formula safely (Beuchat et al., 2009).
Conclusions
C. sakazakii is a pathogen that is emerging which is usually transmitted through PIF. C. sakazakii infections occur in certain groups of people and some cases can become fatal. Infants are at the highest risk and then the elderly and individuals with compromised immune systems. New control measures have been put in place under HACCP to reduce microbiological contamination in food manufacturing. C. sakazakii cannot be viable at high heats during the pasteurization process, however since C. sakazakii is easily found in the environment precautions must be taken when handling PIF post pasteurization.
Cite This Work
To export a reference to this article please select a referencing stye below:
Related Services
View all


Related Content
All TagsContent relating to: "Medicine"
The area of Medicine focuses on the healing of patients, including diagnosing and treating them, as well as the prevention of disease. Medicine is an essential science, looking to combat health issues and improve overall well-being.
Related Articles

DMCA / Removal Request
If you are the original writer of this dissertation and no longer wish to have your work published on the UKDiss.com website then please: