Emotion Regulation in Adults
Info: 7724 words (31 pages) Dissertation
Published: 28th Feb 2022
Tagged: Psychology
Abstract
Emotion regulation (ER) is described as “…the extrinsic and intrinsic processes responsible for monitoring, evaluating, and modifying emotional reactions, especially their intensive and temporal features, to accomplish one’s goals” (Thompson, 1994, pp. 27-28). Emotion regulation has been studied extensively in the psychological literature, and results suggest that difficulty regulating emotion is associated with mental disorders, impaired functioning, and negative health outcomes (Mennin & Farach, 2007). Literature reviews and meta-analyses have examined the relationship between specific ER strategies and mental health outcomes (Lavendar, Wonderlich, Engel, Gordon, Kaye, & Mitchell, 2015; Aldao, Nolen-Hoeksema, & Schweizer, 2010; Busch, Pössel, & Valentine, 2017), using different frameworks to conceptualize the construct. Adrian and colleagues (2011) analyzed ER measures in the child/adolescent literature. In order to examine how ER is measured with adults, this review identified 132 studies appropriate for analysis. Overall, 50% of studies (n = 66) used one measure, and 35.6% (n = 47) used two or three measures of ER. Analyses showed that (a) 73.5% of the included studies have been published since 2011; (b) 72.7% of studies used a self-report measure; (c) self-report methods were used more in recent publications, longitudinal studies, and were associated with fewer citations; (d) cross-sectional designs used neurophysiological measures more frequently than longitudinal designs; and (e) clinical samples were older than non-clinical samples. A summary of the methods used to assess ER revealed differences in the way emotion and regulatory processes are conceptualized and understood.
Methodological Assessment of Emotion Regulation in Adult Samples
Gross (1998) described emotion regulation (ER) as an emerging field that has been explicitly examined since the 1970’s. The regulation of one’s emotions is a multi-faceted process involving influences to manage the emotions one experiences, when they are experienced, and the ways in which they are expressed (Gross, 1998). Managing emotions involves physiological arousal, behavioral expressions, and cognitive evaluations (Thompson, 1994), and regulatory strategies tend to be goal-oriented, involving the regulation of both positive and negative emotions. One might assume that measuring emotions and ER processes is a simple task, but this is not always the case. The minutiae involved in these processes has implications that affect psychological research and the way different tools designed to measure ER are conceptualized.
Different terms are used when referring to emotion and regulatory processes (Gross, 2015). There are affective categories described in the literature that share overlapping components with ER. Emotion regulation is viewed as a subsidiary in a hierarchy of responses (Gross, 2007), and the term affect regulation is the broad construct that encapsulates the other valenced responses. In addition to ER, other constructs include: 1) coping, 2) mood regulation, and 3) psychological defenses. Coping is differentiated from ER in that coping is primarily used to decrease negative affect, and coping strategies can be used for longer periods of time (e.g., bereavement) (Gross, 2007). Similarly, mood regulation tends to be used for affective states that last longer and occur in response to specific “objects”, rather than emotions (Parkinson, Totterdell, Briner, & Reynolds, 1997). Psychological defenses regulate impulses and associated negative emotions, are oftentimes unconscious, and are viewed as a stable trait. These processes share overlapping components, but some argue that it is important to make a distinction between them (Gross, 2007). Because these processes are often used interchangeably to describe the same phenomenon, it makes consolidating the ER literature difficult.
Conceptualization of regulatory processes becomes more complicated as Gross (2015) explains there are also different affective states that regulatory processes are used for. The term “affect” serves as an umbrella term for stress responses, emotions, and moods. Gross (2015) argues that, like regulatory processes, these states share similarities but have subtle distinctions. Stress responses are characterized by negative states and feeling overwhelmed by situational demands, and emotions tend to be triggered by specific negative or positive affective states (Lazarus, 1993). Moods are an affective state that last longer than emotions and are believed to bias cognition (Siemer, 2001), whereas emotions are characterized by their ability to affect behavior. The components of emotion proposed include an affective state that affects one’s behavior, but research suggests that emotion is difficult to define as it is comprised of more nuanced processes.
Gross and Barrett (2011) propose that there are different ways to conceptualize emotion and some argue that emotions are comprised of “loosely coupled changes” in self-reported emotion, behavior, and physiology (Mauss, Levenson, McCarter, Wilhelm, & Gross, 2005). Others posit that specific components are “core” to an emotion and argue that one’s subjective experience is principal (LeDoux, 2012). This position neglects the other two components involved with emotion (e.g., physiology, behavior), and one would be remiss to not account for these subsystems. Cunningham and Zelazo (2007) state that emotions unfold over time and are oftentimes context-specific. Emotion research must be aware of these conceptual foundations, and Gross (1998) offers a framework for emotion that accounts for the three subsystems of emotion.
Because it is imperative to first know an emotion is being experienced prior to its regulation, Gross (2007) proposes a modal model of emotion. This model is comprised of three main components that must be present for an individual to experience an emotion: an interaction between person and situation that elicits attention, meaning to the individual, and a culmination of the two that results in a “multisystem response”. This model is context-specific and contends that emotions can both be useful or harmful. Emotions are helpful when they guide decision making, motivate socially acceptable behavior, and provide individuals with the ability to change the situation (Gross, 2015). Helpful emotions often evoke safety-seeking behaviors during fear-provoking situations and induce more positive feelings that result in behavior that is socially beneficial. Only when an emotion grasps one’s attention and has meaning can it elicit a response. When that response is considered harmful or when the intensity or duration of an emotion is inappropriate for a specific situation (Gross & Jazaieri, 2014), regulation occurs.
Conceptual considerations in emotion regulation
Definitional discrepancies regarding the interplay of emotional processes have resulted in disagreement in measuring ER. Walden and Smith (1997) propose that ER strategies be classified based on the specific emotion system that the individual is trying to modulate (e.g., experience, expression, physiology). Gross (1998) disputes this categorization claiming that it ignores the nuances involved with ER and grossly lumps together different strategies that may in fact have different instrumental goals (e.g., behavior can be inhibited by changing one’s thoughts about the situation). Gross, Sheppes, and Urry (2011) state that a defining feature of ER is that it is goal-oriented. The goal of regulation can be different and subsequently affect the ER strategy that is chosen. For example, one may regulate anger with the goal of feeling less angry, but ER may also be used to achieve some other end. This goal-oriented process may involve showing enthusiasm for an unwanted birthday present to maintain a positive relationship with one’s mother. These components are important for both negative and positive emotions (Gross, 2015). Many ER strategies commonly used are conscious, such as the preceding example. Emotion regulation is often an unconscious process and includes an instinctual reaction, such as quickly covering one’s eyes during a scary movie. Whether unconscious or conscious, the goal-oriented nature of ER is a defining feature (Gross, Sheppes, & Urry, 2011), and research has found that regulatory strategies can be used to manage more than just one’s own emotions.
Gross (2015) contends that once an individual has the goal of regulating an emotion, one may regulate one’s own emotions or the emotions of another. Intrinsic ER occurs when one wants to manage one’s own emotions, and extrinsic ER is characterized by a desire to regulate another’s emotions (Gross & Jazaieri, 2014). Extrinsic ER was first studied in the developmental field to examine interactions between parents and children. The adult literature has assessed this strategy more recently as well (Levenson, Haase, Bloch, Holley, & Seider, 2014). The most commonly used ER strategy is the down-regulation of negative emotions, particularly the physiological and behavioral aspects associated with anger, anxiety, and sadness (Gross, 2015), but regulatory strategies are also used with positive emotions. Quoidbach, Berry, Hansenne, and Mikolajczak (2010) found that individuals were motivated to upregulate emotions such as love and joy to prolong the duration of that emotion. The proposition that individuals are motivated to decrease negative emotions and increase positive ones is representative of the hedonic approach of ER, but Tamir (2009) presents an additional understanding of ER. Within this view, emotions may be regulated for instrumental goals. An instrumental goal includes a desire to appear calm when one receives a promotion but one’s coworker does not. Just as emotion is a multifaceted process, ER is difficult to characterize. Models of emotion regulation have been proposed to help define the processes involved.
Frameworks for ER have been developed to provide clarity for a literature that is convoluted. One such framework is the multidimensional model of emotion regulation (Gratz & Roemer, 2004). This model is comprised of four dimensions theorized to act as maintaining factors for psychopathology. The first dimension assesses how flexibly one uses adaptive ER strategies to change one’s emotion. The second factor examines one’s ability to inhibit impulses and remain goal-oriented. The third component accounts for levels of awareness, clarity, and acceptance, and the fourth dimension assesses experiential avoidance. An advantage of using this model is the adaptability of the dimensions. The components are not disorder-specific and can be applied to mental disorders with different criteria. It offers a flexible framework that researchers can use to examine the effects of emotion dysregulation on symptoms (Racine & Wildes, 2013).
Another common model of ER is Gross’ (1998) process model. The process model extends on the modal model of emotion and provides categories for specific ER strategies. This model identifies strategies that can be used to intervene at the four points of the modal model of emotion (e.g., situation, attention, appraisal, response). These strategies affect the emotion that is being generated at each of these points. When a situation is emotionally relevant, it elicits attention. Gross (1998) defines situation selection as an action an individual takes that affects the likelihood that one will be in a situation that one expects to experience a particular emotion. The second type of strategy used during the situation stage is situation modification. This refers to changing components of a situation to modulate the situation’s emotional impact. Based on the modal model, it is necessary that an emotion grasp one’s attention before it is regulated. Attentional deployment shifts one’s attention away from the situation with the goal of changing one’s response. Appraisal occurs when a situation is evaluated. At the appraisal stage, cognitive change is used. This type of strategy adjusts one’s appraisal of a situation with the goal of mitigating its effect on one’s emotions. Cognitive change can be applied to both external and internal situations, and the most commonly used strategy is reappraisal (Ochsner & Gross, 2005). Response modulation is the final strategy and directly influences the experiential, physiological, or behavioral factors of the emotional response after the emotion has developed. Regulatory strategies that intervene at the response stage can include relaxation.
Models of ER are beneficial because they provide structure to definitions of regulatory processes and emotion-related constructs. It is advantageous to examine these models because they organize different components of ER. Because the field is complicated, these models are commonly used in studies interested in measuring ER. In order to account for the multiple processes, and to replicate the methods of Adrian, Zeman, and Veits (2011), the following definition of ER will be used in this study: “…the extrinsic and intrinsic processes responsible for monitoring, evaluating, and modifying emotional reactions, especially their intensive and temporal features, to accomplish one’s goals” (Thompson, 1994, pp. 27 – 28). The next section describes the findings of meta-analyses and reviews conducted in the adult literature that have used components of these two frameworks to describe the results of the ER literature.
Measurement of emotion regulation
Emotion regulation has been studied with adult samples to examine the relationships between the use of strategies and different factors that affect one’s ability to use ER. Successful use of ER is associated with positive outcomes such as improved health, relationships, and academic and work performance (Gross, 2015). Difficulty regulating emotions is related to psychopathology and negative health outcomes (Mennin & Farach, 2007). Regulatory strategies commonly used by individuals can vary between-persons and by mental disorders. Literature reviews and meta-analyses conducted in adult samples have examined the relationship between specific ER strategies and mental health outcomes (Aldao, Nolen-Hoeksema, & Schweizer, 2010; Hu et al., 2014; Szabo, Warnecke, Newton, & Valentine, 2017). Results suggest that use of maladaptive ER strategies (e.g., rumination, avoidance, suppression) is associated with greater psychopathology, and increased use of adaptive strategies (e.g., cognitive reappraisal) results in more positive outcomes.
Other meta-analyses compared ER strategies (Kohl, Rief, & Glombiewski, 2012) and found differences in effectiveness of acceptance strategies in reducing pain and negative affect. Results suggest that acceptance was a better strategy than maladaptive strategies such as suppression and rumination when the participants’ goal was to tolerate pain. Recent work has also examined the efficacy of treatment programs on ER ability (Khoury, Sharma, Rush, & Fournier, 2015; Menezes, et al., 2015; Franklin, Carson, & Welch, 2016). Khoury and colleagues (2015) found a reduction in overall anxiety and distress in studies examining the effects of mindfulness-based stress reduction in non-clinical samples, and Menezes and colleagues (2015) found similar results in studies assessing the effects of yoga on overall stress and anxiety. In another systematic review studying the benefit of cognitive behavioral therapy on depression and its effects on ER (Franklin, et al., 2016), results, as evidenced by brain imaging changes, revealed increased cognitive control and conscious regulation. The results of these studies highlight important strategies that, when used effectively, can greatly affect one’s well-being and functioning. Like the understanding of definitions and frameworks of ER, the methods used to measure this construct vary.
Meta-analyses and literature reviews provide pertinent information about mental health disorders, individual differences, and constructs that affect ER (Lavendar, et al., 2015), but many of these studies primarily used self-report measures. Aldao and colleagues (2010) summarized the results of 114 studies, all of which used self-reported measures of psychopathology and ER. Naragon-Gainey and colleagues (2017) examined the structure of common ER strategies using meta-analytic techniques for 331 studies’ self-report data. Lavendar and colleagues (2015) reviewed the literature examining emotion dysregulation dimensions in individuals diagnosed with anorexia nervosa (AN) and bulimia nervosa (BN). Their review highlighted the use of self-reported ER conceptualized using the dimensions proposed by Gratz and Roemer (2004). The authors argue that the framework proposed by Gratz and Roemer (2004) is preferable to other models because it accounts for other emotion-related constructs that are salient to psychopathology. There are different processes that affect emotion dysregulation in participants, and these included: alexithymia, inhibition, distress tolerance, experiential avoidance, clarity, and emotional awareness were identified. These constructs have been associated with greater difficulty accessing and engaging in adaptive ER. Results showed that reduced emotional awareness was associated with increased suppression in AN. Because these processes are frequently assessed as predictors of ER ability, measures that account for these will be included in this study.
It is imperative to know about commonly used ER strategies, but these reviews elucidate the current state of the field; most studies measuring ER use self-report measures. Self-report data are limited in that it relies on retrospective accounts of experience and does not assess for unconscious ER use, context-specific use, and temporal change (Naragon-Gainey, et al., 2017). Research suggests that ER is typically measured in four ways: self-report, neurophysiological, behavioral/observational, or other informant. Although a significant number of studies use self-report methodology, a smaller proportion of studies have examined the effects of ER strategies using other methods. In a meta-analysis assessing cardiovascular measures during rumination induction, 43 studies were included in analyses (Busch, Pössel, & Valentine, 2017). Weiss, Thomson, and Chan (2014) examined the ER literature in both children and adults diagnosed with Autism Spectrum Disorder and found that of the 32 studies included, 38% used self-report, 44% included an informant report measure, 31% included a naturalistic observation/behavior coding measure, and 13% included at least one physiological measure. Only 25% of studies used more than one method of measurement.
Employing other modes of assessment of ER provides unique information about emotion experience and offers more comprehensive understanding (Lavendar et al., 2015). Studies show that among the three components of emotion, self-reported emotion and facial behavioral indices were related but physiological response was not as strongly correlated when amusement and sadness were elicited (Mauss, Levenson, McCarter, Wilhelm, & Gross, 2005). Because “externalized processes such as facial expressions are more obviously subject to forces of socialization…than are the internalized processes of visceral, humoral, or immunological responses” (Cacioppo, et al., 1992, p. 110), it is imperative for studies to assess the three components of emotion. They each provide different insight into one’s experience. Measuring ER is a complicated process as there are considerations to make when deciding which modes of assessment are most appropriate for a study’s sample, but Zeman and colleagues (2007) state that the multimethod assessment of ER is paramount in measuring emotion-related experiences. In order to examine the state of the literature in children/adolescents, Adrian and colleagues (2011) conducted a review of the methodology in ER research.
The review spanned 35 years and included typically and atypically developing child/adolescent samples (Adrian, et al., 2011). They noted the patterns of methods used by factors such as age of sample and year of publication. The authors described the study of ER in children/adolescents as an “affect revolution” (Fischer & Tangney, 1995) because the study of ER has changed the way that emotion processes are characterized. Of the 157 studies included in analyses, 33% used a self-report measure, 24% used a physiological method, 56.6% measured behavioral or observational indices, and 36.9% of studies used a measure of other report. The results also showed that 61.1% of studies used one method to measure ER, and 38.9% used two or more indices to measure ER. Additionally, 82.2% of studies were published between 2001 – 2011, suggesting that research on ER has increased in recent years. Observational methods and longitudinal designs were used more often with younger age groups, and self-report measures were used most frequently with the oldest age group (13 – 18 years of age). There were no differences in types of methods by sample type (atypically vs. typically developing). Results also showed that there were 28 distinct self-report measures, 17 other-report tools, 47 observational paradigms, and 8 different physiological assessments used to measure ER.
The results from this study corroborate findings in the field that a majority of studies use only one measure of ER despite theoretical models suggesting that emotion is a multi-modal process (Larsen & Prizmic-Larsen, 2006). There are distinct developmental differences between children/adolescents and adults related to the measurement of ER. For example, the increased use of self-report measures with adolescents is developmentally appropriate and would not be well-suited for infants and children in the toddler/preschool age group. Rothbart, Ziaie and O’Boyle (1992) identified attentional deployment as a strategy that is used early in life and continues to be used in adulthood and later life (Isaacowitz, Toner, & Neupert, 2009). Distraction is a common form of attentional deployment, and its measurement may look different depending on the developmental stage of the sample. For example, using self-report to assess an individual’s use of distraction may be more commonly measured in adults. Whereas attentional deployment may be measured using gaze and eye tracking in infants and young children (Mischel, Ebbesen, & Zeiss, 1972).
Cognitive change is likely not measured as extensively in children/adolescents because children may lack emotional awareness and the ability to communicate use of these strategies effectively (Zeman et al., 2007). Adrian and colleagues (2011) state that parent and teacher ratings are often used to assess children and adolescents’ use of ER strategies. These and behavioral/observational methods such as tones of voice and facial expressions are used to capture the emotional experiences of this population. Observational methods are considered the “gold standard” of developmental research (Cummings, Davies, & Campbell, 2000), but it remains to be seen how often these methods are used in the adult literature. Despite these differences, there are likely similarities between assessment of ER in adults and children/adolescents. A review of the methodology used by studies examining ER in adults is necessary because the results can illuminate the strengths of the field and areas where improvement is warranted. The results can provide insight into ways ER may best be conceptualized. To our knowledge, a literature review examining studies and the way they measure ER has not been conducted with adults.
This study aims to replicate the methodology used by Adrian and colleagues (2011) by analyzing the use of measures of ER in adult samples. Goals of this study include: (1) examine the number and type of assessment strategy used in measuring ER in adults, (2) explore whether the use of modes of assessment differ based on age of sample, (3) investigate whether different methods are used for different samples (e.g., clinical vs. non-clinical), and (4) collect a summary of the measures currently used to provide a guide for researchers.
Method
The specific review criteria replicated the methodology used by Adrian and colleagues (2011). These search terms ensured that the different terminology used to measure regulatory processes was accounted for. The review process consisted of two steps. First, empirical articles with adult samples were identified (i.e., 18 years and older). Search terms (i.e., “emotional regulation”, “emotion regulation”, “emotion management”, “emotional competence”, “effortful control”, and “affect regulation”, “measure”, “scale”, “self-report”, “assessment strategies”, and “survey, and “peer-reviewed journals only”) were entered in both the subject and index terms of the PsycINFO database to capture all appropriate articles. A visual search of all of articles was conducted to determine appropriateness for the study. Studies were excluded if they were a conceptual or review article or if the purpose of the study was to assess the psychometric properties of a measure. Second, articles were coded to determine trends in the assessment of ER. Factors included: (1) the mode of assessment (self-report, neurophysiological, behavioral/observational, or other report)[1], (2) the year of publication, (3) the type of sample (clinical, subclinical, or non-clinical), (4) the research design (cross-sectional vs. longitudinal), and (5) the number of times the article has been cited (as of July 17, 2018).
Results
Methods used
One-hundred and thirty-two studies were identified as appropriate for the review. See the Appendix for a complete listing of the publications, with some articles cited in the References section and denoted by asterisks. The majority of studies (72.7%, n = 96) used one method of assessment, 19.7% (n = 26) used two measures of ER, and 7.6% (n = 10) of the studies used three methods. None of the studies included used all four methods of assessment. Another analysis determined the number of unique measures used and found that 50% (n = 66) used one measure, 35.6% (n = 47) used two or three measures of ER, 12.9% (n = 17) used four or five measures, and 1.5% (n = 2) used six distinct methods. Regarding the number of specific modes of assessment, 72.7% (n = 96) used self-report, 28.8% (n = 38) used a neurophysiological measure of ER, 20.5% (n = 27) used a behavioral/observational method, and 12.9% (n = 17) used a measure categorized as “other report”.
Methodology use by year of publication
Most studies including ER as a variable were published between 2011 and 2021 (73.5%, n = 97), followed by 2000 – 2010 (22.7%, n = 30), and 3.8% (n = 5) published between 1989 – 1999. The key search terms did not yield any studies published before 1996. Crosstab analyses were conducted to examine the number and type of ER measures used by decade (see Figure 1). Between 1989 – 1999, 20% (n = 1) of studies used self-report, 40% (n = 2) used at least one neurophysiological measure, 40% (n = 2) used a behavioral/observational measure, and 20% (n = 1) used one measure of other report. Between 2000 and 2010, 66.7% (n = 20) of studies used self-report, 23.3% (n = 7) used at least one neurophysiological measure, 16.7% (n = 5) used a behavioral measure, and 16.7% (n = 5) used a measure of other report. Between 2011 and 2021, 77.2% (n = 75) of studies used a measure of self-report, 29.9% (n = 29) used at least one neurophysiological measure, 20.5% (n = 15) used a behavioral measure, and 11.3% (n = 11) used a measure of other report.
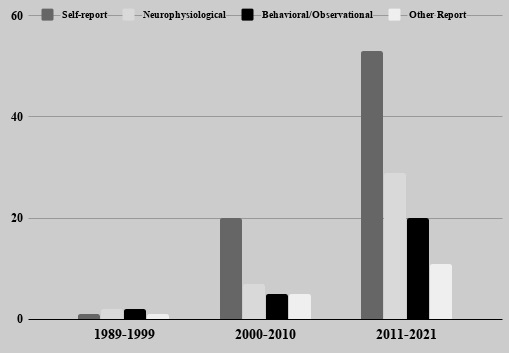
Figure 1. Frequency of ER methods used by decade.
Analyses conducted to examine patterns of ER assessment methods did not reveal any significant trends over time.
Sample type
Studies were coded based on sample type. Studies with samples with a Diagnostic and Statistical Manual of Mental Disorders (DSM) diagnosis (American Psychological Association; APA, 2017) or a medical equivalent were coded as “clinical” (22.7%, n = 30). Studies that included participants who endorsed symptoms of a mental disorder of interest without formal diagnosis were coded “subclinical” (9.8%, n = 13), and studies whose sample was characterized as typically-developing were coded as “non-clinical” (67.4%, n = 89). Chi-square analyses examined differences between sample type and age of participants. Sample age was categorized based on whether the primary sample was college-age (18 – 30) or community-based or mixed (31 – 70). Studies were coded as college-age if the study’s methods indicated that it used an undergraduate sample. Of the 122 articles that included the mean age of their study sample, 61.5% (n = 75) examined college-age samples, and 38.5% (n = 47) assessed samples older than 30 years. Frequency counts for contingency tables included in these analyses were 2 (1) = 9.38, p
Age of sample and methodology
In studies with younger samples (n = 75), 69.3% (n =52) used self-report measures, 36% (n = 27) used neurophysiological methods, 24% (n = 18) used behavioral/observational methods, and 9.3% (n = 7) used a measure of other report. For studies with older samples (n = 47), 86.4% (n = 38) used self-report, 13.6% (n = 6) neurophysiological measures, 11.4% (n = 5) used a behavioral/observational method, and 15.9% (n = 7) used a measure of other report. The number of ER measures used by different age groups did not differ significantly.
Design types
Overall, 82.6% (n = 109) of the included studies used a cross-sectional design, and 17.4% (n = 23) used a longitudinal design. Studies using different design types did not differ significantly when compared with factors such as age of sample, overall number of methods, and number of citations. Welch’s statistic examined differences in study design, as Levene’s test revealed a violation of the assumption of homogeneity of variance. Neurophysiological measures were more commonly used with cross-sectional than longitudinal designs, F(1,128.95) = 22.63, p
Impact by methodology
Chi-square analyses examined relations among the type and number of methods used, the sample and design of the study, and the number of PsycINFO citations. Correlations revealed a number of significant relations between article factors and methodology (see Table 1). Greater number of citations was related to studies using more methods (r = .17, p = .03) and the use of a behavioral/observational measure (r = .23, p = .01). Neurophysiological methods were used more often with younger samples (r = -.19, p = .02) and studies using a cross-sectional research design (r = -.25, p (r = .27, p (r = .15, p = .05), and associated with studies being cited less often (r = -.24, p r = -.15, p r = .21, p = .01).
See Table 2 for all measures used in included studies, organized by methodology type. Methods within each assessment category are listed in order of frequency of use. Measures used only once are listed alphabetically. Overall, there were 54 unique self-report measures, 14 neurophysiological indices, 18 behavioral/observational formats, and 11 other report assessments used in the included studies.
Table 1. Correlational matrix of variables
| Year of publication | Mean age of participants | Sample type | Research design | Times cited | |
| Number of methods | -.02 | -.02 | .08 | -.13 | .17* |
| Self-report | .27** | .15 | .12 | .15* | -.24** |
| Neurophysiological | .04 | -.19* | -.08 | -.25** | .10 |
| Behavioral/Observational | -.04 | -.09 | -.11 | -.04 | .23** |
| Other report | -.15* | .21* | .10 | .06 | -.01 |
Note: Sample type was coded as: 1 = healthy, 2 = subclinical, and 3 = clinical
Research design was coded as: 1 = cross-sectional and 2 = longitudinal
*p ≤ .05.
**p ≤ .01.
Discussion
The purpose of the current study was to replicate the methodology used by Adrian and colleagues (2011) and examine how researchers are measuring ER in adult samples. Empirical articles with adult samples were identified using specific search terms and were coded to compare the methodology based on five factors: (1) the mode of assessment (self-report, neurophysiological, behavioral/observational, or other report), (2) the year of publication, (3) the type of sample (clinical, subclinical, or non-clinical), (4) the research design (cross-sectional vs. longitudinal), and (5) the number of citations.
Analyses revealed that 35.6% (n = 47) of the studies used two or three measures of ER, 12.9% (n = 17) used four or five measures, and 1.5% (n = 2) used six distinct methods. Results suggest that some ER research uses a multimethod framework to capture this multi-faceted process (Gross, 1998), but a high percentage (50%, n = 66) of included studies only used one. The overall number of methods identified mirror results found by Adrian and colleagues (2011) in the child/adolescent literature, in which 61.1% of studies (n = 96) relied on one method. Results showed that 73.5% of studies were published between 2011 and 2021, and the remaining 26.5% were published between 1989 and 2010. These results corroborate the findings from Adrian and colleagues (2011) that the field is in the midst of an “affect revolution” (Fischer & Tangney, 1995), and the study of emotion regulation in psychology is continuing to grow.
Another goal of this review was to assess the tools commonly used to measure ER and consolidate the findings for researchers. A large number of measures have been created for the adult literature. Overall, there were 97 distinct formats used. There were more self-report tools identified than the other three methods combined. Behavioral/observational methods were the second most frequently used methodology, followed by “neurophysiological” and “other report”. The results of this study support findings from reviews and meta-analyses conducted in the field (Aldao, et al., 2010; Naragon-Gainey, et al., 2017; Menezes, et al., 2015). Despite urges for research to use more than one method (Morris, Robinson, & Eisenberg, 2006), these comprehensive reviews show that self-report was the only method used. In the child/adolescent literature, Adrian and colleagues (2011) found that studies used 47 observational paradigms, 28 self-report methods, 17 other report formats, and 8 physiological methods. These results suggest that adult samples rely heavily on self-report formats, and the child/adolescent field incorporates more diverse methodology. The increased use of behavioral/observational and other report measures in the child/adolescent field and decreased use of self-report measures may reflect developmental age and appropriateness (Durbin 2010), but given the retrospective nature of self-report and inability to accurately tap into unconscious processes (Naragon-Gainey et al., 2017), this highlights a gap in the adult field.
Not only was self-report used more frequently overall, but analyses examining the use of methodology by different factors found that self-report methods were used more often in recent publications, in longitudinal designs, and were associated with fewer citations. The increased use of self-report methods in longitudinal designs is not surprising, but the results are still illuminating. Completing a self-report measure is much easier than other methods. Researchers may be more inclined to use this method as opposed to multiple administrations of neurophysiological or behavioral indices over the course of a study. Self-report is more commonly administered, particularly during longitudinal studies, because other measures of ER are more time-intensive and expensive. With that being said, the use of neurophysiological and behavioral measures is critical because they capture components of ER that self-report may neglect. Conceptualizations of ER contend that emotions are temporally-based and context-specific (Cunningham & Zelazo, 2007), and using self-report at one point in time does not account for the nuances associated with ER.
Accordingly, cross-sectional designs used neurophysiological measures more frequently than longitudinal designs. Neurophysiological and behavioral measures provide information about automatic processes that are integral to understanding ER (Thompson, 1994). Further, research suggests that self-reported emotion and behavior (e.g., facial expressions) can be affected by factors such as social influence (Cacioppo, et al., 1992). Neurophysiological indices can provide a more objective measure of ER and offer an avenue for future research to explore further. Using these measures over time can elucidate how self-reported ER use maps on to habitual use. As studies continue to advance and measure ER in unique ways, it will be important to analyze the temporal use of ER (Levenson et al., 2014). Assessment of ER in more naturalistic settings (Naragon-Gainey et al., 2017) can allow researchers to gain insight into individuals’ real-time use of ER strategies.
The type of methods used by age of sample did not differ, but clinical samples were older than non-clinical samples. Forty-three studies (32.6%) were coded as “clinical”, and 67.4% (n = 89) were identified as “non-clinical”. The increased use of non-clinical samples is likely related to psychological research’s use of convenient samples from undergraduate students. Arnett (2008) found that in social psychology journals, 67% of American samples included undergraduate students. This is reflective of the current state of the field as most researchers use college-age samples that tend to be “non-clinical”. Though still interesting and important, using healthy, undergraduate samples limits the research questions and generalizations that can be made (Henrich, Heine, & Norenzayan, 2010). The studies that examined clinical samples were conducted at inpatient facilities or medical centers, and these participants tended to be older and have diagnoses such as breast cancer, bipolar disorder, and borderline personality disorder (Wang, Yi, He, Chen, Li, Yang, & Zhu, 2014; Gul & Khan, 2014; Becerra, Bassett, & Harms, 2016). Compared with the child/adolescent literature, examining age differences in ER is not as highly prioritized because developmental differences are not as substantial. Accordingly, it is critical to examine habitual use of ER in clinical disorders as there may be differences in strategy use and success in implementation over time.
The examination of ER in adult samples continues to develop, and findings suggest that evaluating ER in both clinical and non-clinical samples is of paramount interest to the field. Although multimethod assessment of ER has been advocated for (Zeman et al., 2007), use of more than one method was not reflected in this review. Different conceptualizations of ER complicate its measurement. There are competing definitions, models, and processes to consider, making it difficult to succinctly determine the current state of the literature (Mauss et al., 2005). Multimethod assessment of ER over time is an important area to explore as emotional unfolding has been described as “loosely coupled” over time (Grossberg & Wilson, 1968), while other research contends that emotional components should be synced together (Levenson, 1994). Because the constructs of emotion and ER are so closely related, it is beneficial to understand how emotion subsystems relate over time when ER strategies are being used. Use of ER may have differential impacts on the specific subsystem that is being regulated, and implementation of multimethod assessment could provide clarity on this issue.
Despite a dearth of studies using a multimethod framework, this review highlighted ways in which the field is progressing. Recent studies have examined ER with unique methods and offer new perspectives about the goals of ER processes. Netzer, Van Kleef, and Tamir (2015) assessed the effectiveness of interpersonal ER strategies by a partner’s success playing a video game. More recently, Levy-Gigi and Shamay-Tsoory (2017) examined the interpersonal effectiveness of ER strategies compared with intrapersonal strategies. Given the numerous processes and frameworks involved with conceptualizing ER, the field may benefit by finding ways to consolidate results. A feature of ER that characterizes models and descriptions is its goal-oriented component. Attempting to combine the literature using different factors may be too difficult. An avenue for future exploration could include defining studies by the goal of ER. There are innumerable regulatory strategies, and Gross (1998) claims that strategies may be used for different instrumental goals. Instead of categorizing studies by the strategy used, they can be collapsed depending upon the goal of the strategy. Once the goal of the specific ER strategy is identified, results can be classified. Using this method can allow for an examination of results across studies using different methods and measures. In this way, an intricate literature can be given more structure and results can be disentangled. It is also essential to examine the ways in which different ER-related processes (e.g., alexithymia, emotional awareness, experiential avoidance) correspond with ER strategies and change over time. These processes have been shown to affect ER (Lavendar et al., 2015), and future research efforts should examine their influence on ER goals using methods other than self-report.
This review identified methods that researchers use to measure ER, but there are several limitations to consider. The specific keywords used could have biased the results of the studies that were included in this review. Similar to the results found by Adrian and colleagues (2011), studies examining affective processes published earlier in time may have used different keywords that this search did not capture. Additionally, this search excluded some non-English journals that could not be translated to English, thus this review does not completely reflect the research being conducted in this field. In spite of these limitations, it is imperative for researchers to be aware of the state of the field and the ways in which the current methodology affects the future of emotion research.
This study has important implications. Similar to the results found by Adrian and colleagues (2011), ER research in the adult field continues to grow substantially. Future efforts need to prioritize using multiple methods to measure ER to capture the multifaceted processes of emotion and its regulation (Gross, 2007). Considerable work has been conducted with non-clinical samples, and continued efforts need to be made to assess ER in clinical samples as consistently. Given the paucity of studies incorporating longitudinal designs, using this design should be prioritized. This method can flexibly accommodate more complex research questions. Taking these recommendations into consideration can explicate some of the confusion in the field. In line with the findings of Adrian and colleagues (2011), advancement in multimethod assessment of ER and examining the three subsystems of emotion is indicated. By incorporating these suggestions, the field of ER can be understood more precisely.
[1] Modes of assessment are defined as: Self-report = an individual’s subjective assessment and integration of their own emotions; Neurophysiological = changes in somatic and autonomic or central nervous system activity; Behavioral/Observational = Body gestures, tones of voice, reaction time, and facial expressions that relay information about emotional experiences; Other report = questionnaires or interviews that assess some aspect of a participant’s functioning from someone else’s perspective
Cite This Work
To export a reference to this article please select a referencing stye below:
Related Services
View all


Related Content
All TagsContent relating to: "Psychology"
Psychology is the study of human behaviour and the mind, taking into account external factors, experiences, social influences and other factors. Psychologists set out to understand the mind of humans, exploring how different factors can contribute to behaviour, thoughts, and feelings.
Related Articles

DMCA / Removal Request
If you are the original writer of this dissertation and no longer wish to have your work published on the UKDiss.com website then please: