Educational Intervention to Improve Nurses Knowledge of Pressure Injury
Info: 8468 words (34 pages) Dissertation
Published: 23rd Feb 2022
Improving knowledge of assistant nurses regarding pressure injury through an educational intervention to prevent pressure injury in an aged care facility.
ABSTRACT
Knowledge on pressure injury prevention is very important among the health care staff. Education, in-service education and trainings are one of the important and effective method in upgrading knowledge level of care staff. Health care staff with poor knowledge on pressure injury prevention is found to be not adopting effective preventive measures of pressure injury which can result into incidence of pressure injury. So, education session was conducted with the aim to improve the knowledge level of assistant nurses in the aged care facility. The method was a education session for each participants who participated in the pre test with the 25-30 minutes structures educational content with the help of power point slide and the explanations with the help of posters. The evaluation of the knowledge level was assessed by using structured questionnaire before and after the education session. Comparison between the pretest and post test were done to assess the improvement of knowledge level. The score above 75% was considered good level of knowledge, 50% to 74% was considered moderate level of knowledge and 50% below was considered having poor level of knowledge. It was found that level of good knowledge increased from 13% to 78%, moderate knowledge decreased to 22% from 40% while no participants had poor knowledge after the education session which showed improved in knowledge level of assistant nurses in aged care facility.
Table of Contents
Click to expand Table of Contents
Part One
1.1 Introduction
PART TWO
2.1 BACKGROUND
2.2 LITERATURE REVIEW
2.2.1 Search Strategy
2.2.2 Literature Review Of The Articles
2.3 Aim Of The Project
2.4 Rationale And Significance Of The Subject
PART THREE
3.1. Description Of The Project
3.1.1 Strategies/Methods
3.1.2 Time frame of the project activities
3.1.3 Evaluation Tool
3.1.4 Educational Contents
PART FOUR
4.1 Data Presentation
PART FIVE
5.1. Results
5.2. Limitations/ Challenges
5.3. Changes From The Proposal
5.4. Implications For The Practice
5.5 Summary
5.6 Conclusion
REFERENCES
APPENDIX
Permission Letter
LIST OF TABLES AND FIGURES
Figure 1: PowerPoint slide of pressure injury prevention
Figure 2: Pressure Ulcer Prevention Guide
Figure 3: Smith & Nephew Pressure injury identification guide
Figure 4: Smith & Nephew Pressure injury outline of care
Figure 5: Pressure Area Clock
Figure 6: Data representing which are true statement about pressure injury
Figure 7: Graph representing most susceptible site to develop pressure injury
Figure 8: A risk to develop pressure injury
Figure 9: Graph represents what should not be done to prevent the pressure ulcer
Figure 10: Graph represents the people who should actively involved in the reduction of a patient/resident’s pressure injury
Figure 11: Graph represents the risk factors for development of pressure injury
Figure 12: Graph represents the time frame in which pressure injury can form
Figure 13: The graph represents the when the patients are assessed for risk of pressure injury
Figure 14: This graph represents the best guidelines for the residents who are risk of developing pressure injury should be evaluated
Figure 15: Graph represents the repositioning technique to prevent pressure injury.
Figure 16: The graph represents the true or false answer of the self administered questionnaire which was from question number 11 to 18.
Figure 17: Pie charts showing level of pressure injury prevention knowledge during pre and post test.
Part One
1.1 Introduction
Pressure injury are the injuries which are localized damage to the skin or body tissue resulting pressure combined with shear and friction (Agrawal & Chauhan 2012). It is more common on elderly patients and patients with neurological impairment in young and has high mortality rate altering quality of life so prevention is considered as important goal (Agrawal & Chauhan 2012). The risk factors that can cause bed-sore are malnutrition, poor nutrition status, poor personal hygiene, mobility problems, chronic illness , paralysis, ageing, incontinence, loss of sensation, circulation disorders (Bhattacharya & Mishra 2015).
The prevalence of pressure injury has remained as a matter of concern in the globe as it is the third leading disorder in terms expenditure (Agrawal & Chauhan 2012). As a matter of fact, pressure injury is still an unsolved problem in developed nations such as United States of America, The United Kingdom and Australia in which the prevalence of pressure ulcer is 11%, 29% and 16.5% respectively (Alja’afresh & Mosleh 2013). Most importantly, pressure injury is a quality care indicator that shows the level of care provided to the patient (Payne 2016).
This report illustrates project which took for six weeks from 16 April 2018 to 27 May 2018 where education session on pressure injury was conducted and the improvement on the knowledge level of pressure injury was assessed among Assistant Nurses working in the aged care facility. The questionnaire adapted from PREVENT PRESSURE ULCERS with some modification, is taken as a evaluation tool to assess the improvement of the knowledge on pressure injury among assistant nurse before and after the education session.
Research Question:- Does an educational intervention improve the knowledge of assistant nurses regarding pressure injury prevention in an aged care setting?
PART TWO
2.1 BACKGROUND
Pressure injury is considered as the diseases entity since long time ago. Pressure injury is costly to be treated and physically devastating complications in the 20th century and it is considered as the third most expensive disorder after cardiovascular diseases and cancer (Taylor, B and Kaas, J 2002, p. 41). Several studies have undergone on the pressure injury usually on the incidence of pressure injury. In spinal cord injury patients, pressure injury it likely occurs in 30-85% of patients during the 1st month of injury. Also, patients with paraplegics and quadriplegics are prone to multiple injuries (Chauhan et.al 2005, p.36-37).
In addition, in-service education and training should be carried out to train and develop awareness among staff regarding the proper use of risk assessment tool and skin inspection to prevent PI. Apart from risk assessment, regular weight check to identify malnutrition among residents need to be implemented. Because evidence suggests that unplanned weight loss related to poor nutritional intake and inactivity or bed bound leads to the development of PI in older people (Iizaka et al. 2010). The preventive measures recommended by the National Pressure Ulcer Advisory Panel (2016) for pressure injury through risk assessment, skin assessment, skin care, nutrition, reposition and mobilization, education. Healthcare setting follow the recommended guideline by NPUAP to prevent the risk of pressure injury among elderly people through developing specific policy. The current policy of pressure injuries preventive measures provides detailed description of risk assessment (Barden, Norton or Waterlow risk scale), skin integrity assessment, and skin care, repositioning, application of foam or air mattress and pressure relieving measures, documentation, education, training, in-service education, recording and reporting of the pressure sores incidence from assistant nursing to registered nurse and to higher authority and also consulting with family members regarding referral if condition became severe (Watson et al 2009).
2.2 LITERATURE REVIEW
2.2.1 Search Strategy
For the extensive literature review the literature search strategy has been developed. The databases from UOW CINAHL, PubMed, Medline Plus, Scopus, Science Direct and the Cochrane Review were used. The literature review paper for this project includes the various research studies which are mainly qualitative, quantitative, randomized controlled trial and the systemic reviews. The literature review was limited to English language articles which were published in the year 2000 to 2018. Moreover, the websites namely Prevent pressure ulcers, World Health Organization. The search terms used are P1= Pressure injury, P2= Knowledge, P3= Prevention. P4= Health personnel or Health care workers or health staff or health workers or Assistant nurses, P5= Education or education program or training or inservice education. The combination of the search terms using AND P1 and P2 and P3 and P4 and P4=P5 which was the result for literature search.
2.2.2 Literature Review Of The Articles
Pressure injuries are a normal occurrence in aged care facilities since the gaining population is most vulnerable due to their softened tissues and body structure as they age (Edsberg, Black & Goldberg et al., 2016). The commonly affected areas are hips, elbows, heels, coccyx, shoulders, ankles, and behind the cranium (Fullbrook, Nowicki & Franks, 2014).
Abraham & Johnson claim when pressure is applied to these areas, there is partial or complete obstruction of blood to the soft tissue and it results in a pull on blood vessels meant to feed the skin. Also Fullbrook, Miles & Nowicki, et al., elaborate that these injuries are more serious in individuals who hardly move around like is the case for the aged population especially if they are bed ridden or need support and are on a wheelchair (Nguyen, Chaboyer & Whitty,2015). Other than old age, other factors have been associated with pressure injuries. According to Hazelholf, Gerritsen & Schoonhoven et al., they include microclimate, diseases like neuropathy and paralysis that affect skin sensation, diseases like arteriosclerosis that reduce blood flow to the skin, and protein-calorie malnutrition. However, Nguyen, Chaboyer & Whitty, insist that the aged population in aged care facilities is more affected because the age of these individuals slows down their healing process and most of them have diseases like diabetes and arteriosclerosis that slow down their immune system further (Edsberg, Black & Goldberg et al., 2016).
Besides, Edsberg, Black & Goldberg et al., do claim early detection of pressure injuries is difficult thus making treatment and prevention of pressure ulcers more difficult. In critically ill and frail individuals, the most common primary prevention method is to regularly turning the individual in an effort to redistribute the body pressure being experienced. According to them, Santamaria, Gerdtz & Sage et al., this has always been practiced since the 19th century besides advocating for a healthier diet with more protein for the person, and keeping the skin dry. Santamaria, Gerdtz & Sage et al., insist that prevalence rate of pressure injuries in Australian aged care facilities was at 26% in 2013 and up to 23% in European aged care facilities (Fullbrook, Nowicki & Franks, 2014). Awareness and education of both caregiver and patients is an very important factor in the prevention, reduction and treatment of pressure injuries. To limit the risk of getting pressure injuries, all the individuals involved from the multidisciplinary group should be able to detect the early signs of the damage of the skin caused by pressure and should plan the care accordingly (Lloyd, J 2007).
Numerous campaigns and guidelines have been published on how pressure injuries can be reduced and prevented (Santamaria, Gerdtz & Sage et al., 2015). A classic example is the Pressure Ulcer Risk Assessment and Prevention Campaign being driven by the Royal College of Nursing in Australia (Nguyen, Chaboyer & Whitty,2015). The Australian Pan Pacific Pressure Injury Alliance also published a clinical guidelines report that recommends various strategies meant to prevent pressure sores. Abraham & Johnson claim that the guidelines suggest pressure redistribution, repositioning, support surface redistribution, and providence of a healthier nutritional support as prevention measures that can be adopted by aged care facilities.
According to Santamaria, Gerdtz & Sage et al., training and education session is important because assistant nurses get to understand the patients and other staff members they will be working with in the aged care facility. On this note, Abraham & Johnson insists that training will involve both theoretical and practical responsibilities where the assistant nurses will be expected to demonstrate the practical aspect of all the theory they will be taught. Both Hazelholf, Gerritsen & Schoonhoven et al., and Nguyen, Chaboyer & Whitty, claim they should also be taught on pre-service training which includes how to treat these patients from the moment they are received and making sure that they are comfortably settling in their new accommodations (Santamaria, Gerdtz & Sage et al., 2015). Training will also involve understanding the role of family members in taking care of their patient.
According to Santamaria, Gerdtz & Sage et al., Involvement with family members is important because it is important to understand the patient on a personal level including their family life and how the established visiting policies are affecting the patients. Edsberg, Black & Goldberg et al., insist that training should also involve improving the nurse’s empathy and teaching them on the importance of supporting the patients and their families considering that the aging individual will be deteriorating over time and may succumb to their age at any point. Besides, Fullbrook, Miles & Nowicki, et al., claims interacting with the aging individual’s family will create a good relationship between the assistant nurse and the individual’s family and the former can teach the latter how to turn their family member whenever they visit for long hours (Abraham & Johnson, 2003).
Fernandes et al. 2008, conducted a study with descriptive-comparative orientation ,50 participants comprising of 11 nurses, 10 technicians and 29 nursing assistants, took part. The instrument of the change was educative intervention and knowledge of the professionals was the dependent variable, data regarding which was collected in January and February 2005, prior to and post the informative mediation. The test is made out of 41 true or false proclamations whose substance originate from North-American rule suggestions for the proof based practice to foresee and anticipate PU with content adjustment for the setting of help of the basic patient. The assistants and technicians got 74.3% of right answers in the pre-mediation stage and 81.2% in the post-mediation stage, showing that for this gathering of experts, the intercession enhanced the test outcomes. In the post-mediation stage, in 23 questions, the assistants and nursing specialists got more right answers and in 25, the rates of right answers were higher than 80%, which proves an expansion in the right answers after mediation. The information displayed demonstrate that the educative mediation delivered positive results in the worldwide right decision taking rates about knowledge with respect to PU preventive measures, its beginning and assessment. Nonetheless, in a few inquiries, the level of information was beneath 70%. PU counteractive action requires better comprehension of the experts about the viewpoints including its improvement, and in addition attitudes towards moral care with the appropriation of prescribed practices on, including the use of reasonable resources.
According to study conducted by wogamon, 2016 actualized a quality change exertion to investigate the impact of a 1-hour CNA training program about early recognizable proof, treatment, and counteractive action of PUs on PU learning, PU rate, and PU avoidance intercessions, including skin checks. In the experiment all the 33 employed CNAs( Certified nursing assistant) participated who worked in an aged care where inhabitants of 55+ years of age were residing. Their knowledge about PU was assessed utilizing the Pressure Ulcer Toolkit poll previously, promptly after, and 3 months following the instructive mediation about PU aversion. Residents’ medicinal records were dug for information on turning/repositioning, skin checks, and suggesting staff of suspicious zones of skin for the 3 months pre-and post-instructive mediation. Out of 31 CNAs surveyed, 26 (84%) claimed that they received training regarding PU prevention in the classroom during their initial CNA training, and 81% received on-the-job training at some point in their careers regarding PU prevention. The Quality Indicator report demonstrated a lessening from 5 PUs to 0 (12.3%) in the 3 months pre-mediation to 0% in the 3 months post-intercession. Revealing of skin breakdown by CNA expanded from 8 reports to 17, with an increase by 68%. Wogamon, 2016 reported that although knowledge scores did not get improved significantly by the training on PU identification and prevention measures, but the rate of PU development was significantly lowered and thequantity of reported skin appraisals and PU intercessions got improved after the instruction program.
2.3 Aim Of The Project
Assistant nurses are the one who are the first care taker of the resident so research on this population should be done to assess the knowledge level and the practice they are doing it. The sole main of this project was undertaken to assess and improve the knowledge of the assistant nurses regarding pressure injury and its prevention through an educational intervention to prevent the pressure injury in an aged care facility within six weeks.
2.4 Rationale And Significance Of The Subject
Pressure injury has become one of the global health issues mostly affecting elderly in residential aged care setting. The incidence of pressure injury in residential aged care setting is very common and one of the critical health concern which is directly linked with the quality care and the burden on the caregiver and the organization. Elderly with immobility are very prone to pressure injury which can lead to pressure injury, wound infections and also sepsis. So, the preventive measures should be applied in order to prevent the pressure injury. It can be achieved through updating the knowledge of care staff by raising awareness and training (McErlean et. al. 2006, p: 62-73).
Pressure injury are very common among elderly who is in acute and chronic care facilities. As it is said prevention of pressure is always better than treating the complications which is associated with it, so it is essential to prevent the occurrence of pressure injury. Prevalence of pressure injury is defined as the number of clients with at least having one pressure injury who exist in a population at a given point in time (WOCN 2009). Moreover, 1 million individuals usually develops pressure injury each year (WOCN 2009).
According to study done by Prentice, J, Stacey, M and lewin, G 2003, p. 87-88, it shows that the people having pressure injury is in range of 10.6 to 13. 6% in private hospital where as 3% to 5.4 % in an aged care. Among the population who were receiving or getting home care for pressure wound, the incidence of pressure injury has been increased from 6 to 8 %. Hence, In between 1983 and 2002, the incidence of pressure injury is increased from 3% to 36.7%, which is overall reported incidence of pressure injury in Australian health care setting.
Education sessions on pressure injury and its preventive measures should be conducted much often to assess and follow up knowledge and awareness on the preventive measures of pressure injury (Mengistu, D & Dilie, A 2015).
PART THREE
3.1. Description Of The Project
This part of the project includes description of the project conducted for six weeks from 16th April to 27th May 2018 in the aged care facility aimed to improve knowledge level of assistant nurses on pressure injury. The number of participants who voluntarily agreed to take part in the project were involved.
Structured questionnaire on pressure injury adapted from Prevent Pressure Ulcers (Know the facts and Take Action) was distributed to get an insight of their knowledge level on pressure injury among 10 AINs (Assistant Nurses) working in the aged care facility. Education sessions were conducted based on structured educational contents based on the questionnaire. Pre-test and post-test was taken to compare the findings before and after an education session.
3.1.1 Strategies/Methods
The following strategies were implemented in order to conduct the project. After topic and research question was finalized and just after the planning literature search was done on pressure injury prevention and the instrument was finalized. After that lesson plan on the contents of pressure injury prevention for the education session was developed. Approval from Director of nursing was taken and the purpose of the project was made aware. Likewise, assistant nurses working in an aged care were also informed about the project. Pre test was conducted to assess the knowledge of AINs followed by 20-30 mins of education session and the post test was done.
3.1.2 Time frame of the project activities
| ACTIVITIES | WEEK | DATE |
| Planning Framework of the project | Week 1 | 16/04/2018- 22/04/2018 |
| Review and research of the articles | Week 1-2 | 23/04/2018-29/04/2018 |
| Questionnaire and Education session materials development | Week 2 | 23/04/2018-29/04/2018 |
| Informed and approval from director of nursing and assistant nurses | Week 3 | 30/04/2018-06/05/2018 |
| Pretest | Week 4 | 07/05/2018-13/05/2018 |
| Education session | Week 5 | 14/05/2018-20/05/2018 |
| Post test | Week 5 | 14/05/2018-20/05/2018 |
| Data Analysis | Week 6 | 21/05/2018-27/05/2018 |
3.1.3 Evaluation Tool
The instrument used was self administered questionnaire on pressure injury prevention among assistant nurses adapted from Prevent Pressure ulcer and has been attached as APPENDIX below. Details regarding the participants were not included in the study. Total 18 Questions were included to assess the knowledge level of assistant nurses. Questions were structured type with multiple choice questions, true or false. Each of the correct answer were marked as One. For each correct answer one was given and for the wrong answer no marks were given. The score above the 75% was considered good level, 50% to 74% was considered moderate level and below 50% was considered having poor level of knowledge.
3.1.4 Educational Contents
Contents of the education session was according to the topic and the time was allocated for each topic regarding pressure injury prevention. The lesson plan is developed below:-
| S.No | CONTENTS | METHODS | TIME DURATION |
| 1 | Introduction on pressure injury | Explanations/PPT Slide | 1 minutes |
| 2 | Information on Epidemiology, Common areas affected | Explanations/PPT Slide | 3 minutes |
| 3 | Information on pathogenesis, risk factors | Explanations/PPT Slide | 4 minutes |
| 4 | Information on stages of pressure injury | Explanations/PPT Slide | 2 minutes |
| 5 | Prevention of pressure injury | Youtube video/ Posters/ Explanations | 8 minutes |
| 6 | Complications | Explanations | 2 minutes |
| 7 | Summary | Interactive discussion/ summarization | 4 minutes |
The power point slides used in the education session has been attached below:-
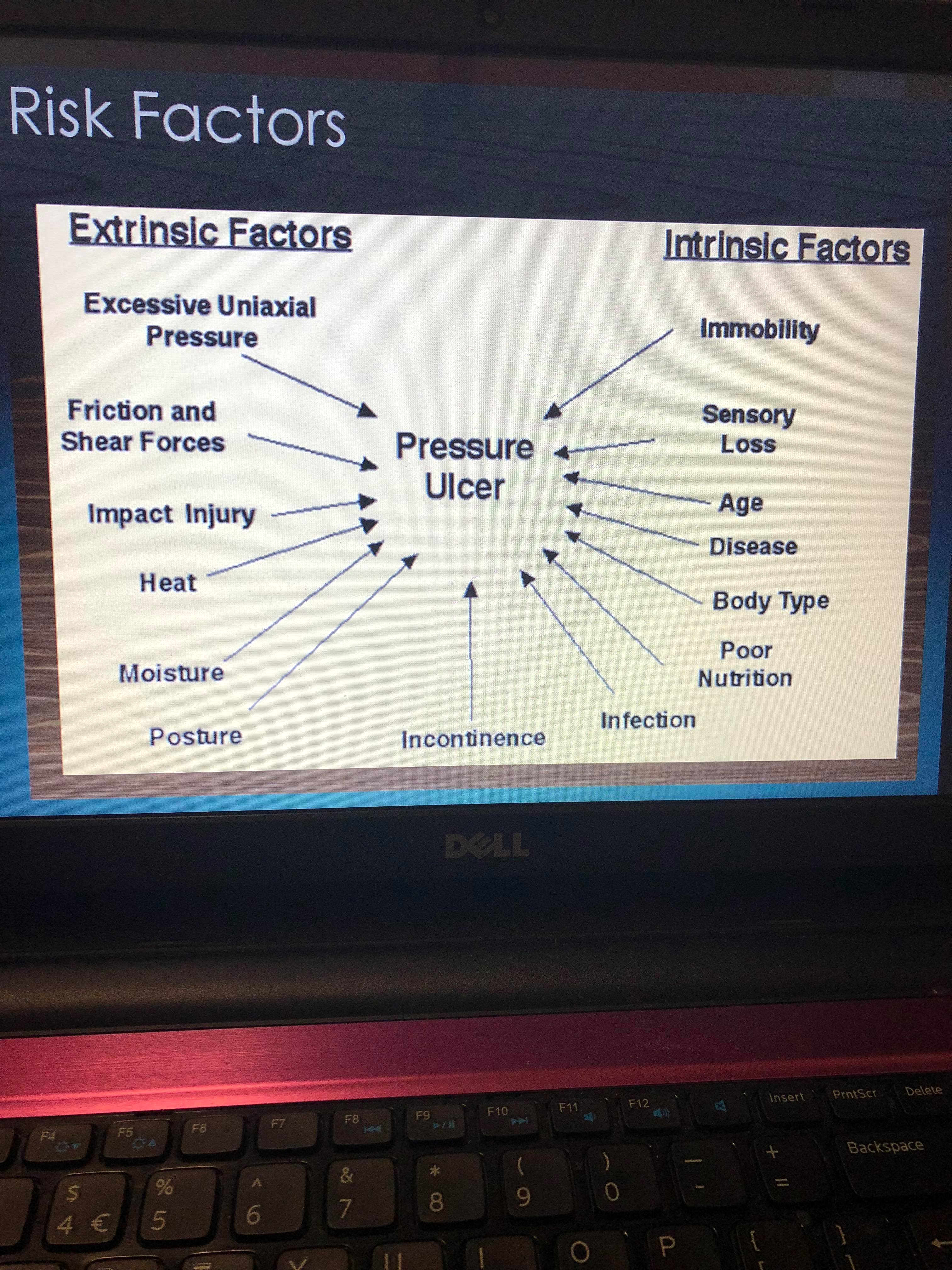
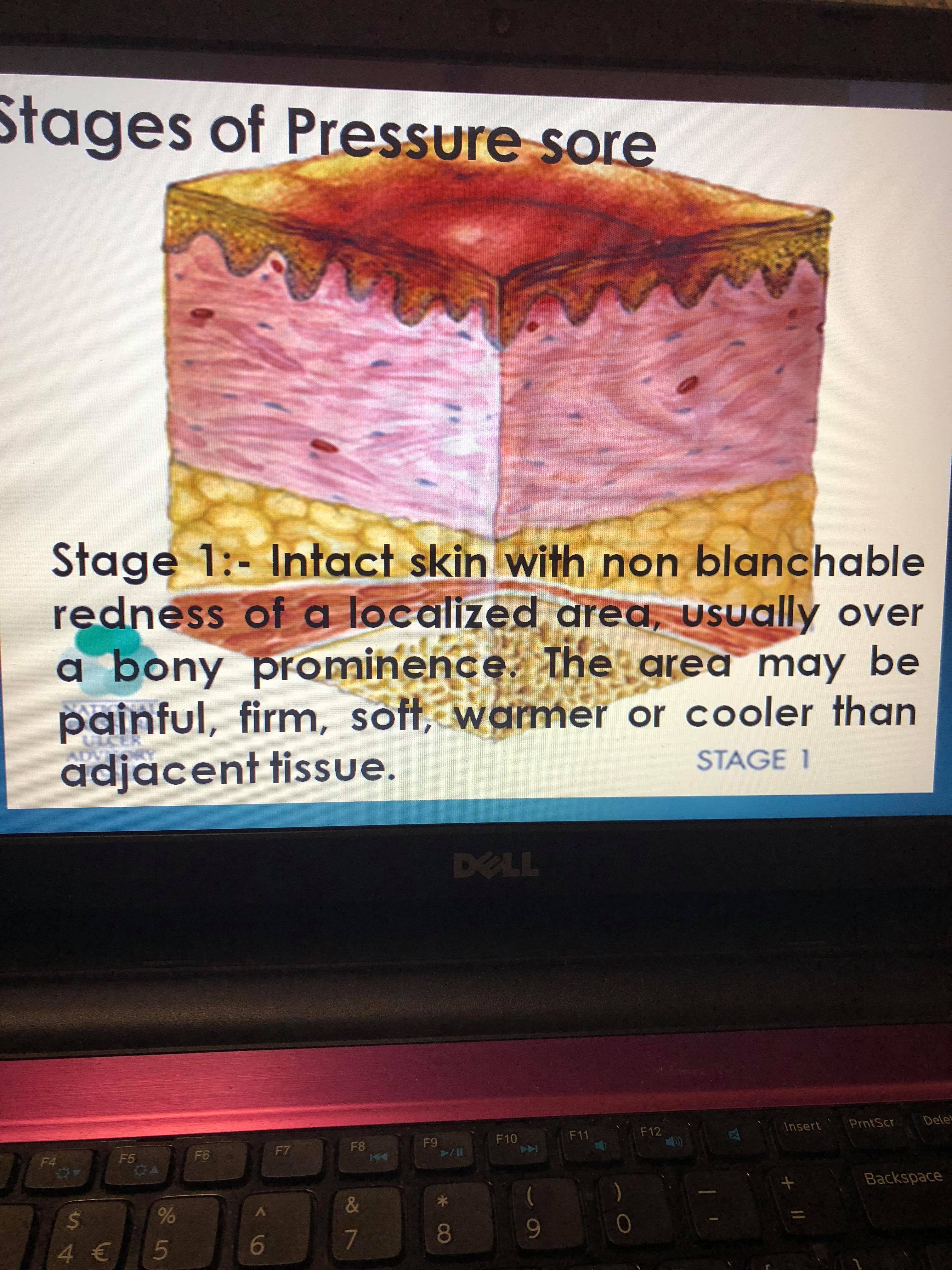
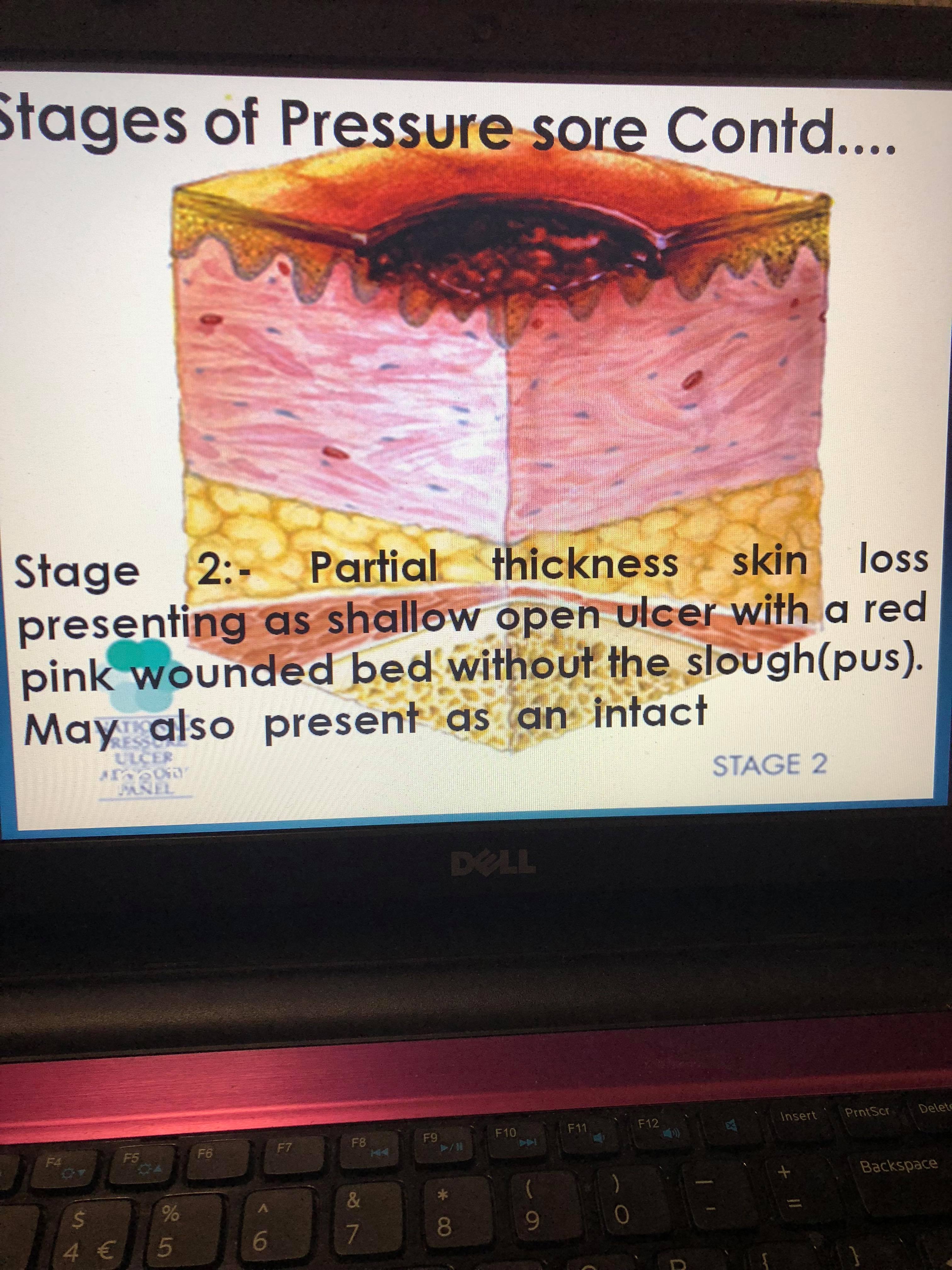
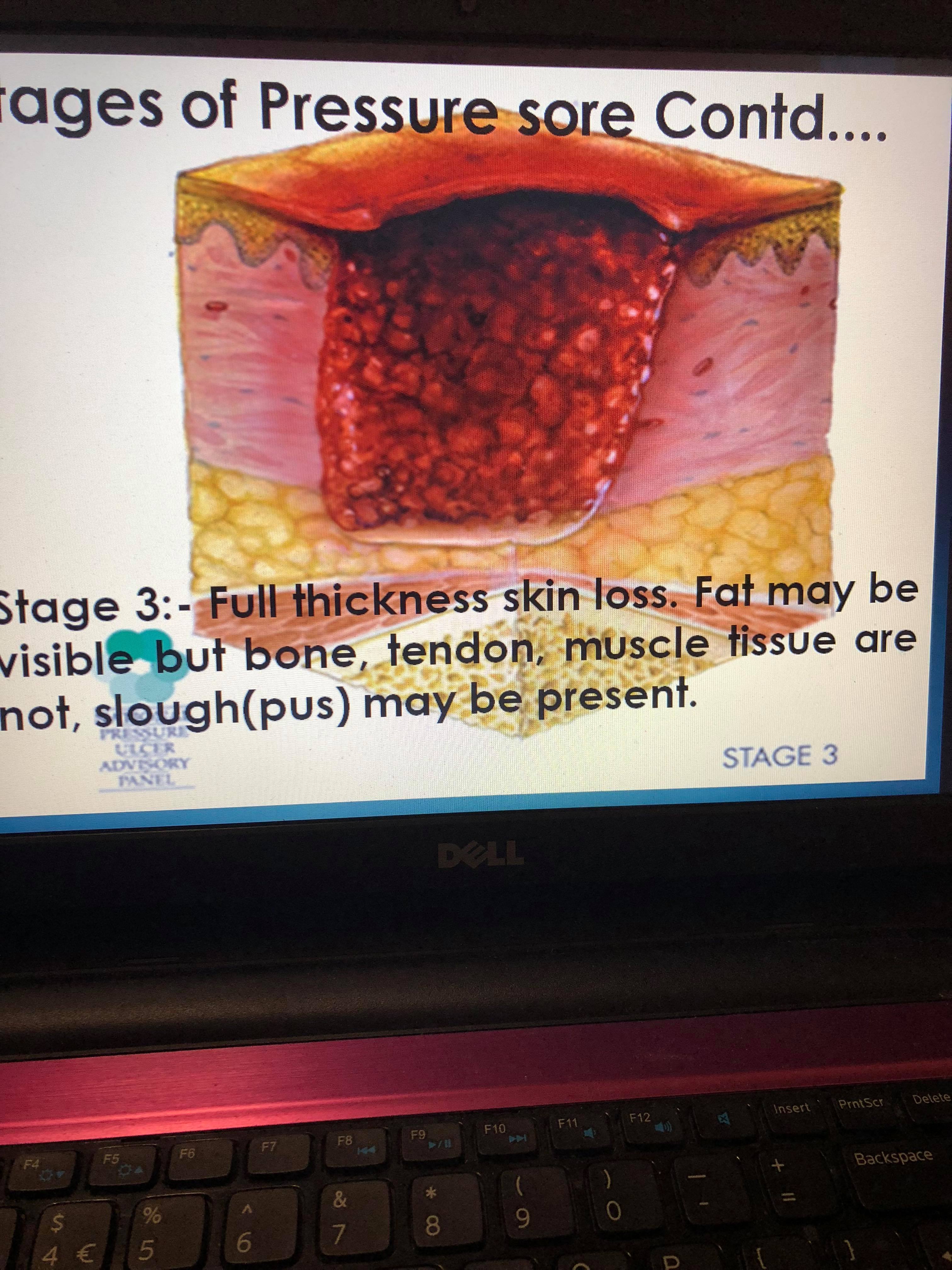
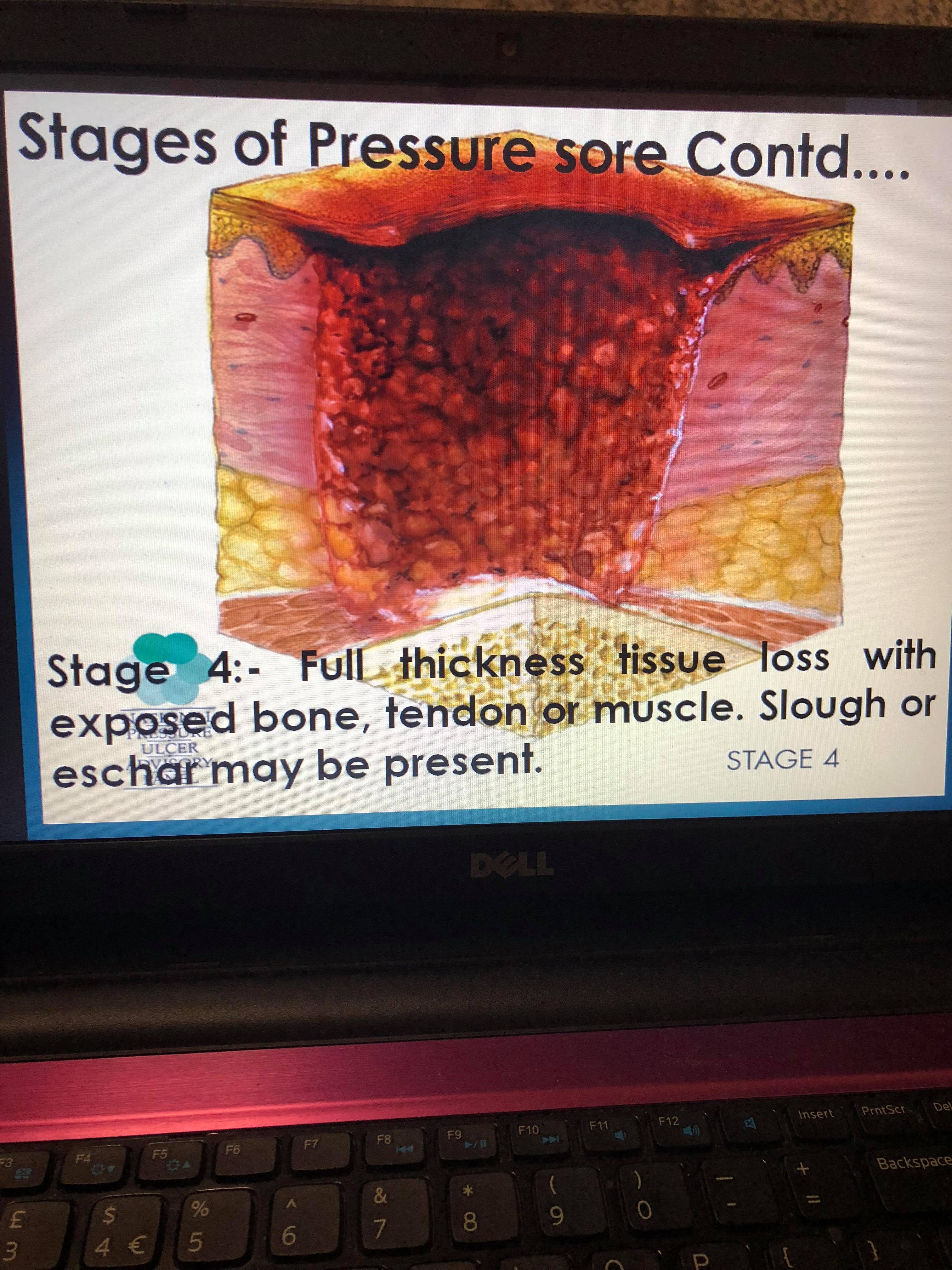
Figure 1: PowerPoint slide of pressure injury prevention
For the prevention part, you tube video was shown which covered over all area of pressure injury and preventive measures which can be done to prevent pressure injury. I have attached the link of you tube video:-
https://www.youtube.com/watch?v=vimqv2dgo-Y
The posters used in the education session is attached below:-
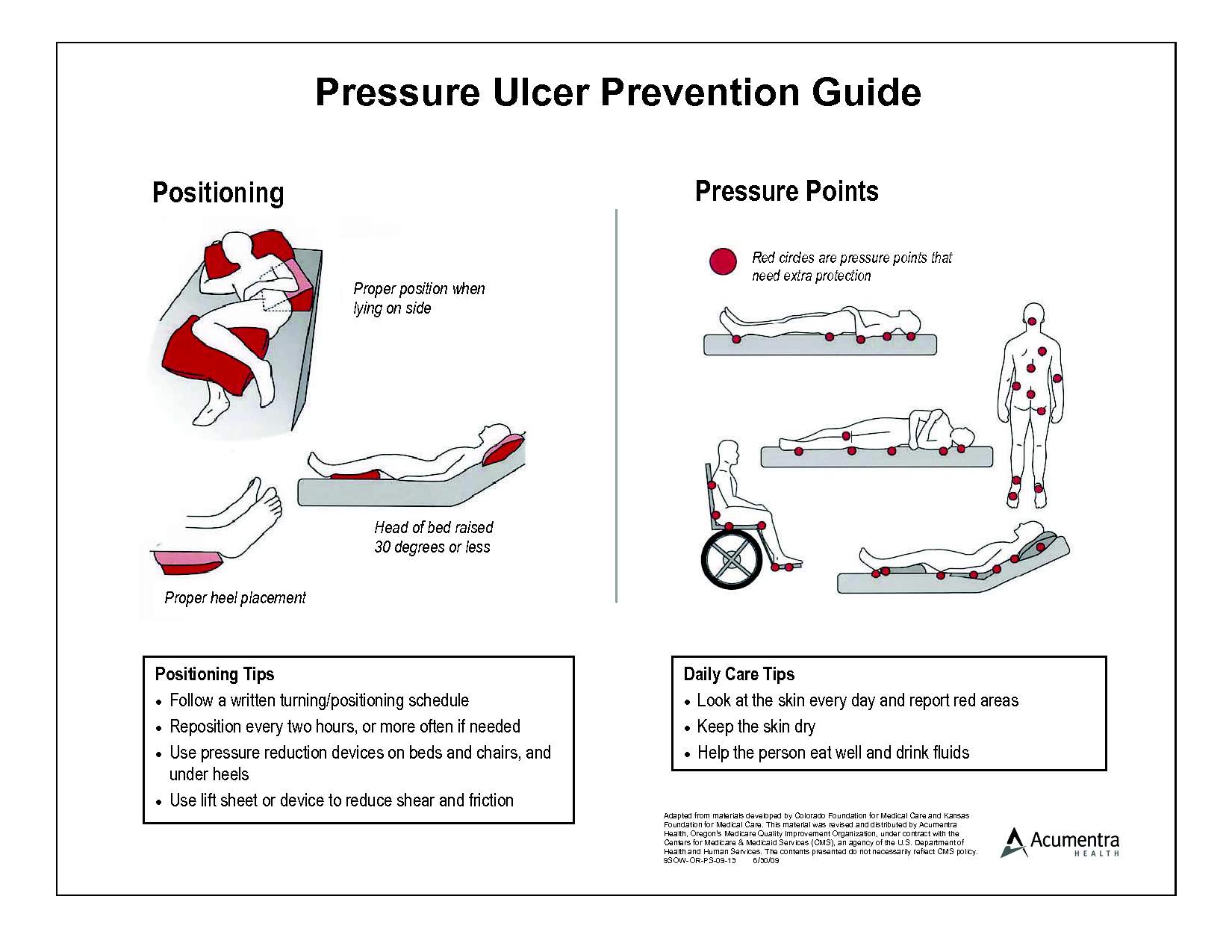
Figure 2: Pressure Ulcer Prevention Guide
IMPLEMENTATION AFTER EDUCATION SESSION:
After the education session I have asked permission with my Manager to attach some posters regarding prevention of pressure injury in nursing station board and I have also made Pressure area clock and attached to the head of bed side which indicates that the resident need repositioning. Two and Four hourly pressure area clock were placed in bed side according to the condition of the resident. If resident is not able to mobilize himself and needs assistance with repositioning and usually are double assist then two hourly pressure area clock was paste in head of the bed and outside the door of the residents room so whenever nurses passes by they will be aware that they have to reposition the resident. And if resident are usually wheelchair bound and move himself but has to depend on nurses for toileting and need assistance while walking were kept under four hourly pressure area clock. The picture of the posters and pressure area clock has been attached below.
The poster pasted in the nurse station and notice board is attached below:-
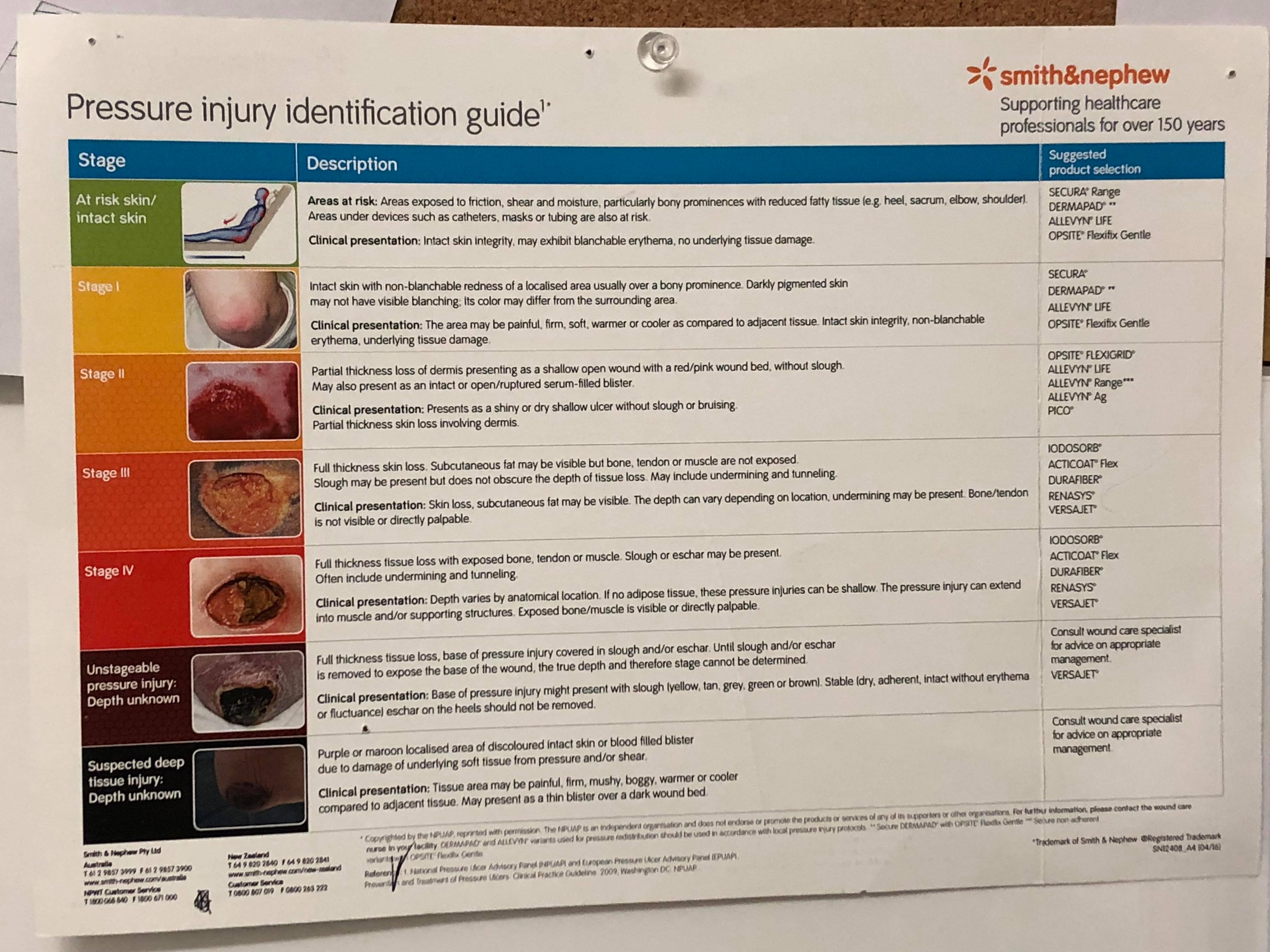
Figure 3: Smith & Nephew Pressure injury identification guide
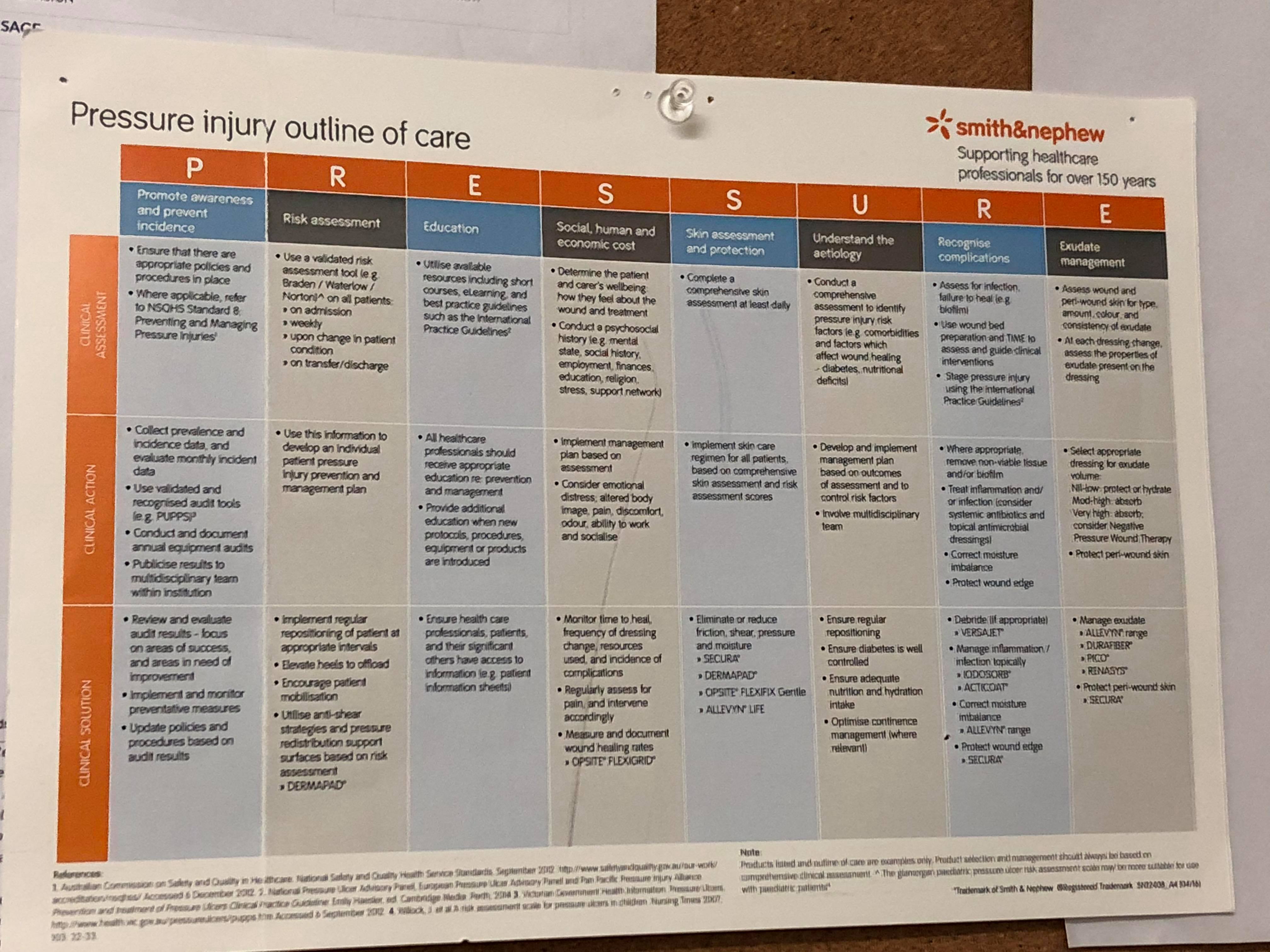
Figure 4: Smith & Nephew Pressure injury outline of care
The pressure area clock in bed side and outside the door has been attached below:-
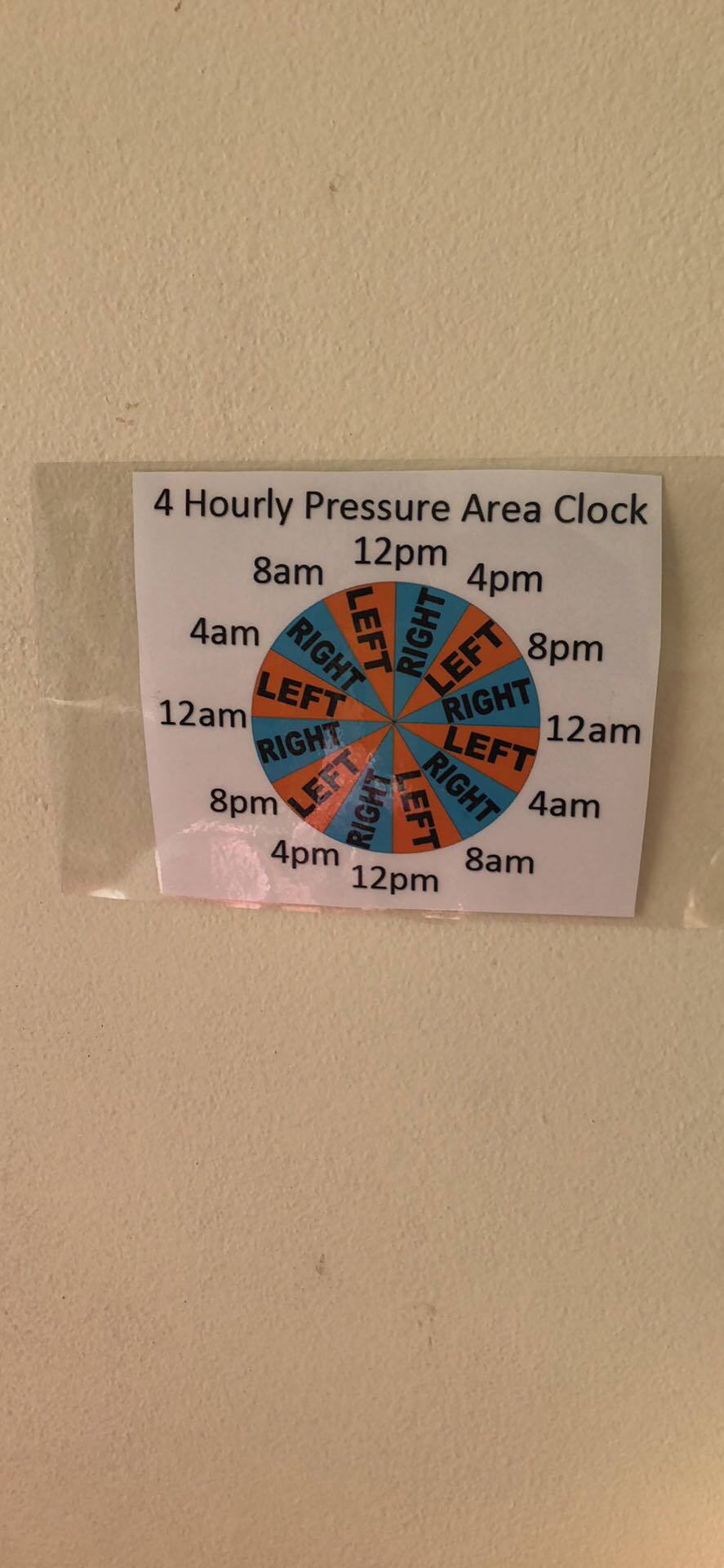
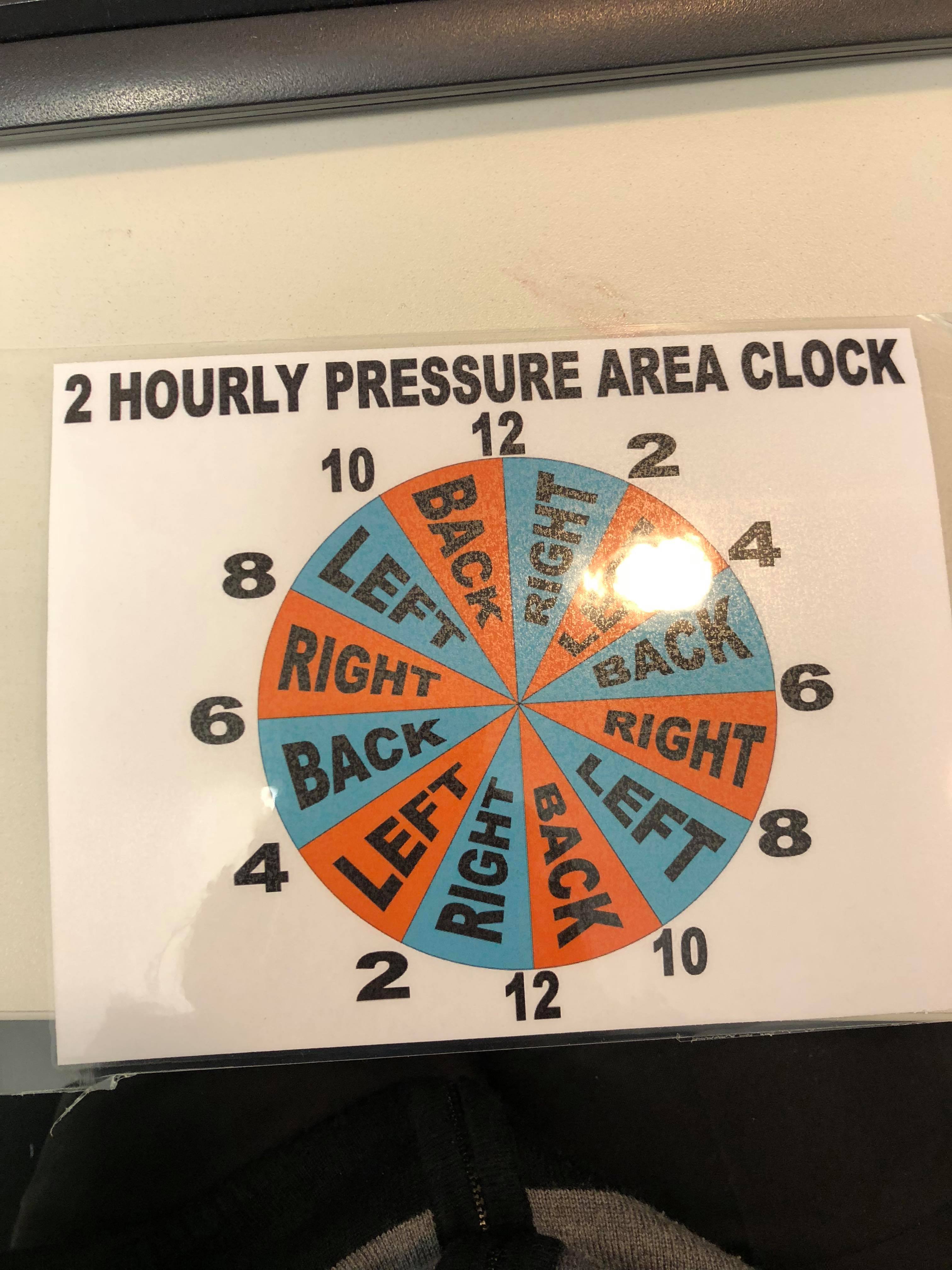
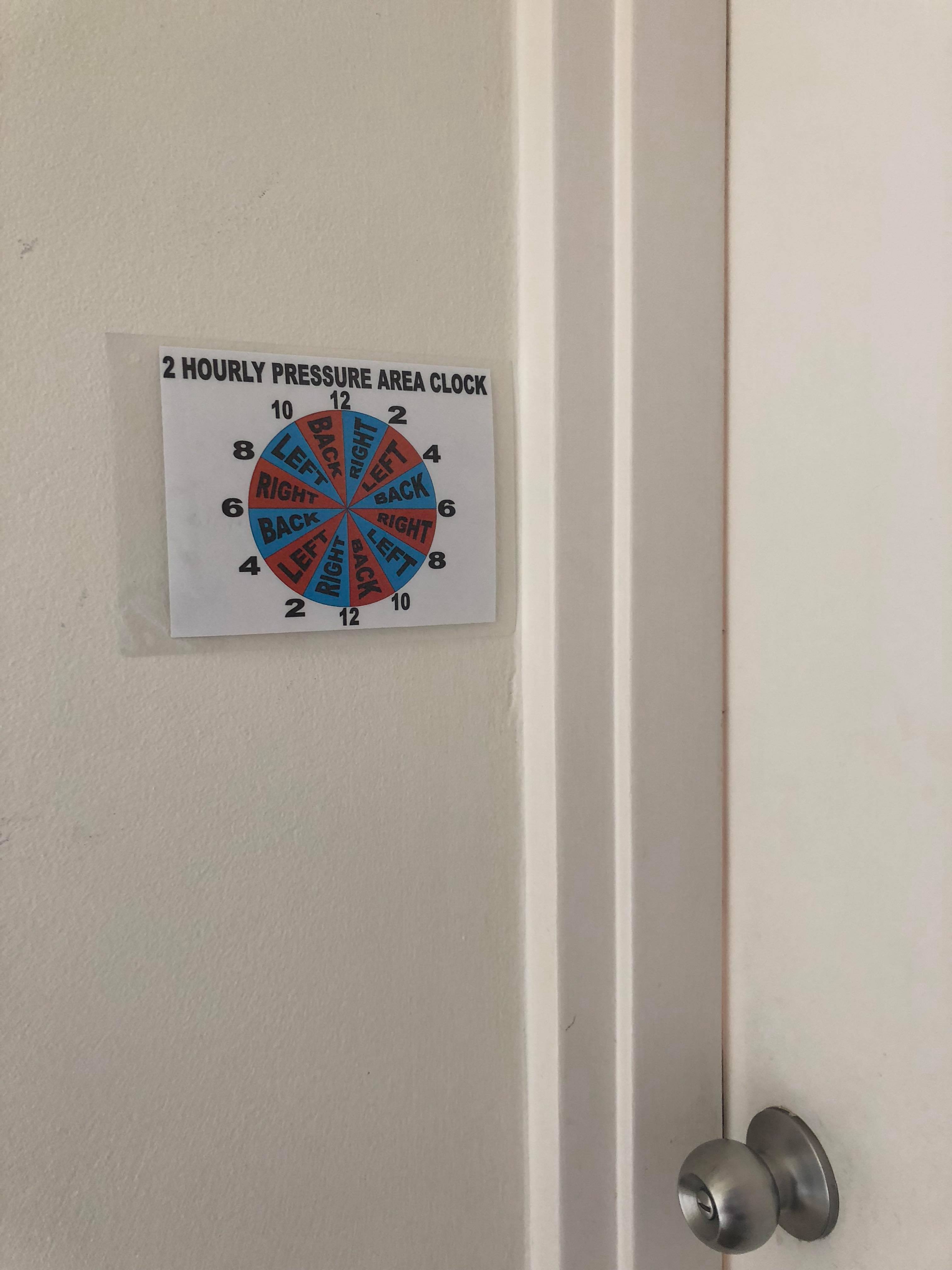
Figure 5: Pressure Area Clock
PART FOUR
4.1 Data Presentation
The data was collected from 10 assistant nurses working in aged care facility who participated in the pre test and post test. The collected data are presented in the form of graphs below which represents the response of assistant nurses on following test items:-
PART A : CHOOSE THE BEST ANSWER
1) Which statement is true about pressure injury?

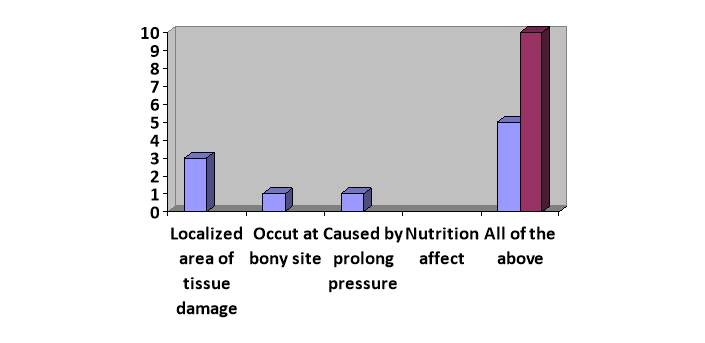
Pre test
Post test
Figure 6: Data representing which are true statement about pressure injury
The figure demonstrates that only 5 participants gave correct answer at pre-test and during post test all 10 participants gave correct answer.
2) Which sites are the most susceptible to pressure ulcer development
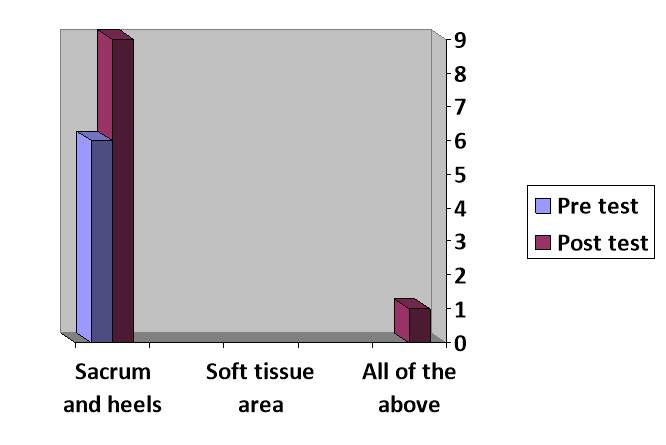
Figure 7: Graph representing most susceptible site to develop pressure injury
Majority of the participants gave correct answer after education session
3) Patients/residents would be considered most “at risk” to develop a pressure ulcer
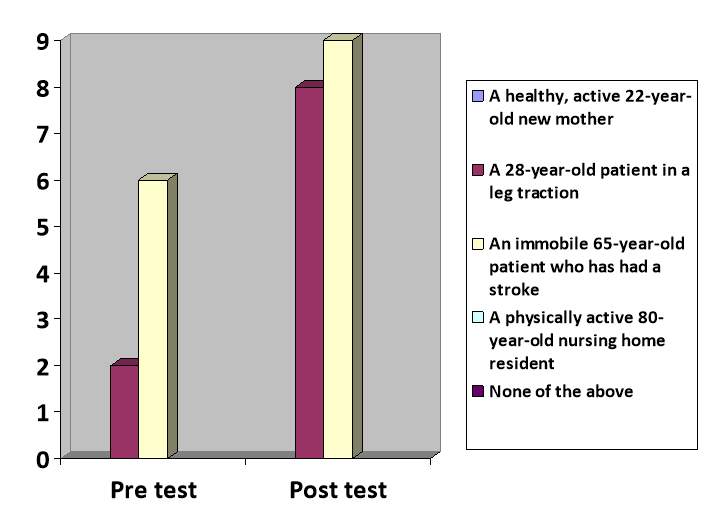
Figure 8: A risk to develop pressure injury
After the education session most of the participants gave the right answer about the risk to develop pressure injury.
4) To prevent pressure ulcers from developing, which of the following steps should NOT be taken?
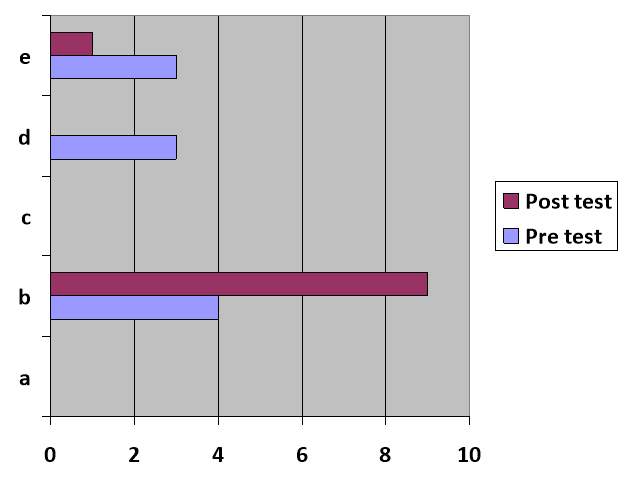
Figure 9: Graph represents what should not be done to prevent the pressure ulcer
During the pre test and post test of education session though this question is the tricky one during pre test only few gave the correct answer but after the education session majority of the resident gave correct answer.
5) In a home health care agency, who should be actively involved in the reduction of a patient/resident’s pressure ulcer?
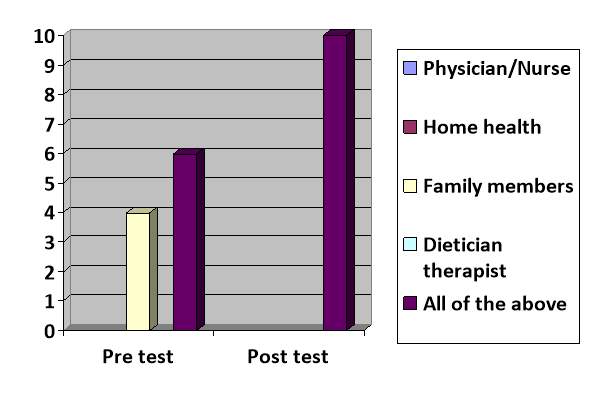
Figure 10: Graph represents the people who should actively involved in the reduction of a patient/resident’s pressure injury
The result indicates that after the education session the knowledge of participants was increased and gave the correct answer.
6) A resident/patient is at risk for pressure ulcers when they are or have:
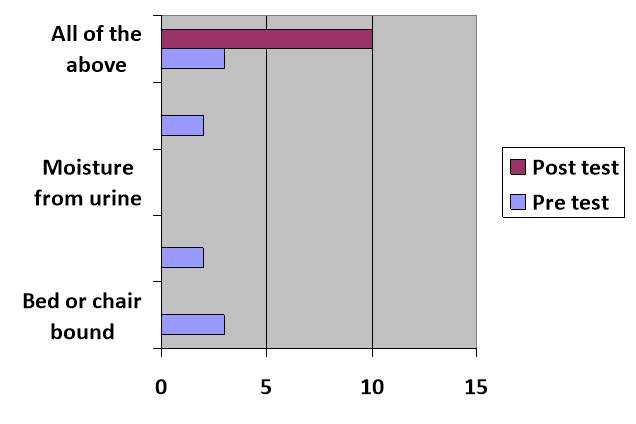
Figure 11: Graph represents the risk factors for development of pressure injury
Majority of the participants gave correct answer about the risk factor of development of pressure injury in pre test after education session
7) A pressure ulcer can form in:
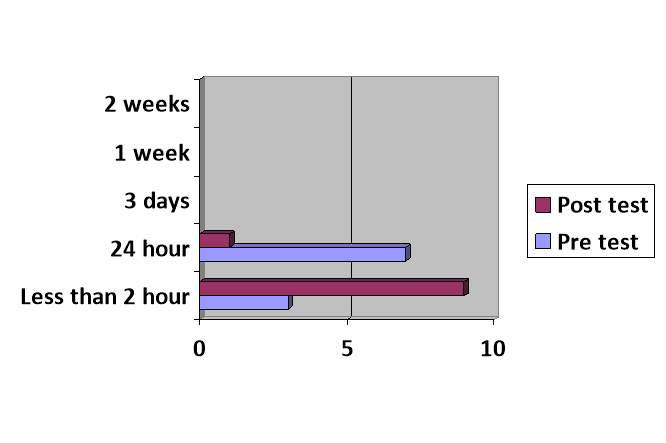
Figure 12: Graph represents the time frame in which pressure injury can form
Pressure injury can form in less than 30 minutes in residents if there is high pressure in small area of the body so option a is correct answer which majority of the participants gave after education session.
8) Residents/patients are assessed for risk of pressure ulcers:
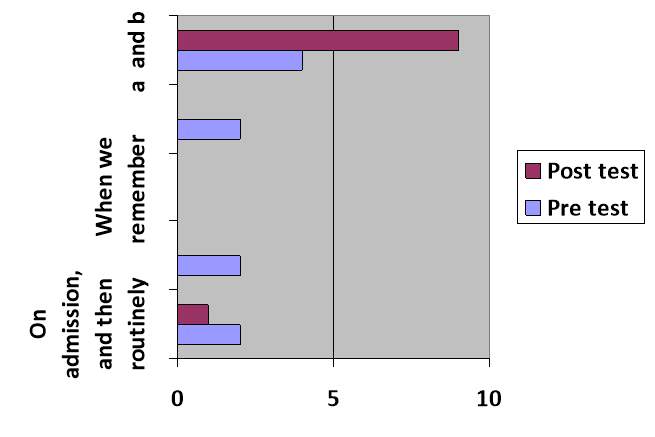
Figure 13: The graph represents the when the patients are assessed for risk of pressure injury
Residents assessment of pressure injury is very essential and there are different tools for the assessment of risk Though each individual client is at potential risk of developing pressure injury, client with neurological problems, poor nutrition, deformity, old age and those who are immobile are at high risk of developing pressure ulcer (Payne 2016). After education intervention majority of the resident chose option e which is the correct answer.
9) According to best guidelines, residents and patients who are at risk of developing a pressure ulcer should be evaluated for which of the following:
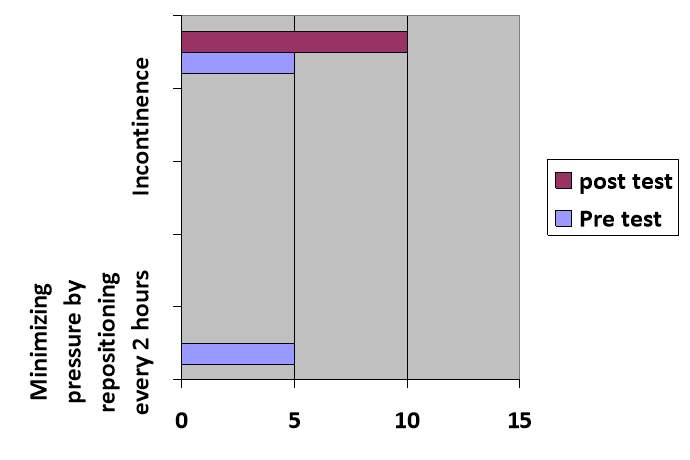
Figure 14: This graph represents the best guidelines for the residents who are risk of developing pressure injury should be evaluated
In this session of the test 50% of the participants gave correct answer in the pre test and after the education session 100% of the participants gave correct answer in the post test.
10)Which of the following repositioning techniques are key preventing pressure?
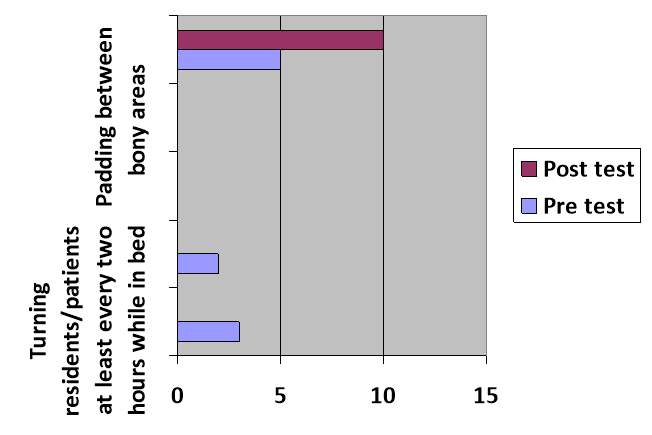
Figure 15: Graph represents the repositioning technique to prevent pressure injury.
This graph represents the repositioning technique to prevent pressure injury and after the education session majority of the participants gave right answer.
PART B
CIRCLE ‘TRUE’ OR ‘FALSE’
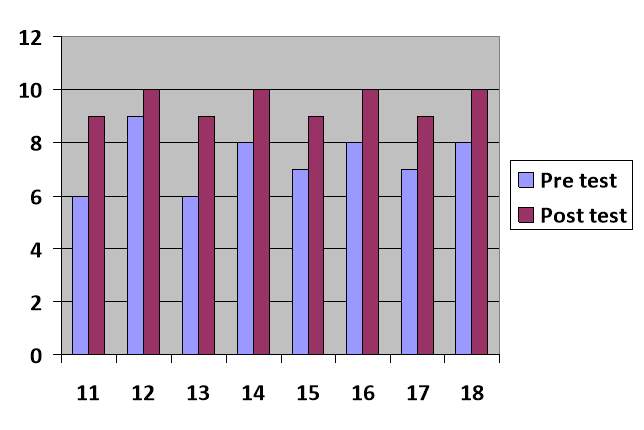
Figure 16: The graph represents the true or false answer of the self administered questionnaire which was from question number 11 to 18.
Question number 11 to 18 is a true or false questions for each correct answer 1 is given and for the incorrect answer 0 marks is given. Though the knowledge of participants seems pretty fair in true or false questions but still not 100% but after the education session almost 100% of the participants gave the correct answer which clearly denotes that after the education session participants level of knowledge has increased.
PRE TEST:-
POST TEST
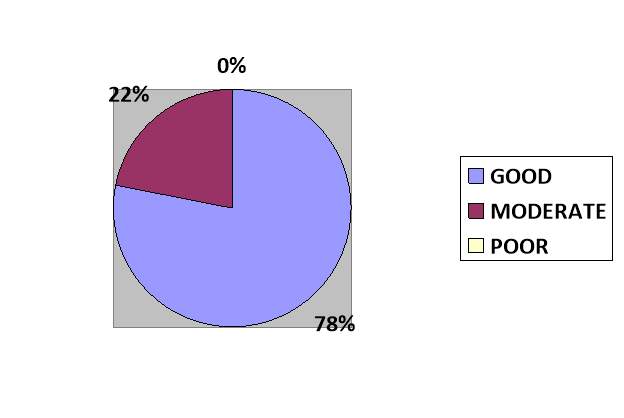
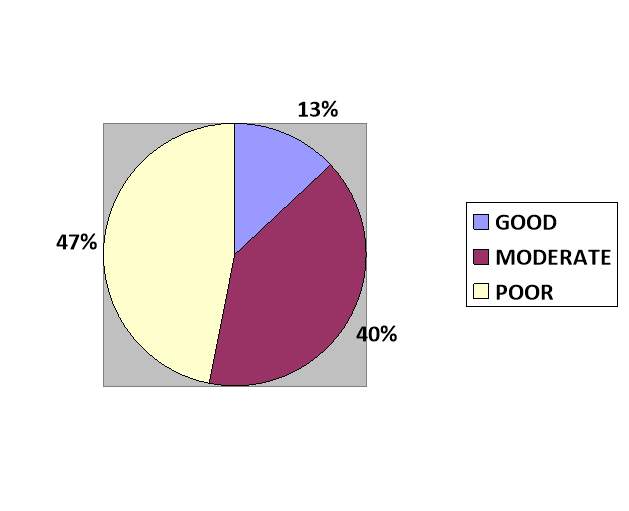
Figure 17: Pie charts showing level of pressure injury prevention knowledge during pre and post test.
The pie chart illustartes the knowledge level of assistant nurses which is based on the questionnaire set above in the evaluation tool. The pre-test pie chart shows that 47% of the participants had poor knowledge and 40 % had moderate level of knowledge whereas 13% had good knowledge regarding pressure injury. Moreover, the post test pie chart shows that 78% had good knowledge regarding pressure injury followed by 22% of moderate knowledge level. This pie chart between pre and post test denotes that the level of good knowledge increased from 13% to 78%. Similarly, moderate level of knowledge decreased to 22% from 40%.
PART FIVE
5.1. Results
The knowledge level of assistant nurses of good knowledge increased from 13% to 78%. Similarly, moderate knowledge level decreased to 22% from 40% after the education session.
5.2. Limitations/ Challenges
The limitations/challenges faced while conducting this project are as follows:-
- All the assistant nurses were not able to participate due to duty hours and schedule.
- Participants were not able to manage time due to their tight duty schedule.
- Due to lack of time of the participants pressure to finish the educational content on time.
- Hard to bring all participants in one education session so it resulted in two education session.
5.3. Changes From The Proposal
Some changes were made after result was published of project proposal keeping in mind the valuable feedback of subject coordinator. The aim of project proposal was very board so it has been changed and have become specific one. The aim of the proposal was to increase awareness regarding pressure injury among the care staff working in an aged care setting to reduce the incidence and prevent the pressure injury which has been changed to education intervention to improve knowledge level of assistant nurses in the aged care facility.
5.4. Implications For The Practice
- All the health care staff should have knowledge about pressure injury and its preventive measures to provide quality and holistic care.
- Assistant nurses should be trained on pressure injury prevention and ongoing in service education to update the knowledge regarding prevention of pressure injury.
- The different approaches and strategies should be applied rather than just one single intervention to bring a positive change in the knowledge level
- Identification of the factor which is lacking in the aged care and introduction to the effective implementation to prevent pressure injury should be carried out.
5.5 Summary
Pressure injury is one of the global health issues and occurrence of pressure injury in aged care facilities is very common since the elderly people is most vulnerable due to their softened tissues and body structure as they age. It is the critical health concern worldwide which is directly linked with the quality and holistic care and the burden on the caregiver and the aged care facility. So in order to prevent the pressure injury the different preventive measures and strategies should be applied. One of the factor contributing to the less implementation of preventive measures and compliance is poor education. Knowledge is a ongoing process so upgrading the knowledge of care staff is essential so that the implementation are adopted properly. Therefore, education session was conducted in the aged care aiming to improve the knowledge level of pressure injury among assistant nurses. The result demonstrates that level of good knowledge was increased from 13% to 78%. Similarly, moderate knowledge level decreased from 40% to 22%. Moreover, participants did not report poor level of knowledge which was 47% before the education session. This result illustrates that the chief aim of the project has been met.
5.6 Conclusion
This project was conducted in period of six weeks and firstly the project conducted to collect the relevant information regarding pressure injury and its prevention with the help of search strategies. This project helped to broadened critical thinking and reasoning skills in reviewing the related literature. To conduct the project by assessing, thinking and planning strategies which are achievable, measurable, realistic, accurate and be completed within time frame. Moreover, it analysis and presentation of the data was done in appropriate manner. Finally, this project provided an opportunity to reflect, limitations, challenges and implementation practice for the future. Despite of the fact this project has its own significance and relevance but it would have been better with different strategies, wider settings, more number of participants, more use of tools and resources with extended time. This project could be conducted in the aged care setting with more participants to assess and upgrade the knowledge of assistant nurses with educational intervention and tools to assess its effectiveness. This project has helped me a lot and the experience of conducting it was very thrilling and exciting and the learning achieved from this would be very much useful for the future reference and implications.
REFERENCES
Abraham, M & Johnson, B 2003, ‘Changing the Concept of Families as Visitors’, Supporting Family Presence and Participation, Bethesda, MD: Institute for Family-Centered Care.
Agrawal, K, & Chauhan, N 2012, ‘Pressure ulcers: Back to the basics’, Indian Journal of Plastic Surgery, pp. 244-254, NCBI Resources, viewed 24 May 2018
Bhattacharya, S, & Mishra, RK 2015, ‘Pressure ulcers: Current understanding and newer modalities of treatment’, Indian Journal of Plastic Surgery, vol. 48, no. 1, pp. 4-16.
Chauhan V.S, Goel S, Kumar P, Srivastava S, Shukla VK 2005, ‘The prevalence of pressure ulcers in hospitalized patients in a university hospital in India’, Journal of Wound Care, Vol. 14, pp. 36–37.
Edsberg, L.E, Black, J.M, Goldberg, M, McNichol, L, Moore, L, & Sieggreen, M 2016, ‘Revised national pressure ulcer advisory panel pressure injury staging system: revised pressure injury staging system’, Journal of Wound, Ostomy, and Continence Nursing, vol.43, no.6, pp.585.
European Pressure Ulcer Advisory Panel (2003) Pressure Ulcer Prevention Guidelines. Available at: http://www.epuap.org/glprevention.html (accessed 26 October 2009), viwed on 28th May 2018.
Fernandes, LM, Caliri, M & Haas, VJ 2008,’The effect of educative interventions on the pressure ulcer prevention knowledge of nursing professionals’, Acta Paul Enferm, vol.21, no. 2
Fullbrook, M, Nowicki, P & Franks, C 2014, ‘Decreasing Pressure Injury Prevalence in an Australian General Hospital: A 10 Year Review’, Wound Practice and Research.
Hazelholf, T, Gerritsen, D, Schoonhoven, L & Koopmans, T 2014, ‘The Educating Nursing Staff Effectively. (TENSE) Study: Design of a Cluster Randomized Controlled Trial’, BMC Nursing, vol.13, no. 46
Hemavathy, V, Girijabhaskaran & Devi, K 2016,’ A study to assess the knowledge and practice regarding pressure ulcer among students of BSC nursing 3rd year in Sree Balaji College of nursing, Chennai’, International Journal of Applied Research, vol. 2, no. 4, pp. 252-253.
Iizaka S, Okuwa M, Sugama J and Sanada H., 2010, ‘The impact of malnutrition and nutrition-related factors on the development and severity of pressure ulcers in older patients receiving home care’, Clinical Nutrition, vol. 29, pp. 47–53
Martin L, Nelson E, Lloyd R and Nolan T 2007, ‘Whole System Measures’, IHI Innovation Series white paper. Cambridge, Massachusetts: Institute for Healthcare Improvement; 2007. (Available on www.IHI.org)
McErlean, B, Thomas, L, Page, T & Simunov, K 2006, ‘Collaborating to improve pressure ulcer prevention practices: the South Australian experience’, Primary Intention, vol. 14, no. 2, pp. 67-73.
Mengistu, D & Dilie, A 2015, ‘Assessment of Nurses’ Knowledge, Attitude, and Perceived Barriers to Expressed Pressure Ulcer Prevention Practice in Addis Ababa Government Hospitals, Addis Ababa, Ethiopia ‘, Advances in Nursing.
Nguyen, K.H, Chaboyer, W, & Whitty, J.A 2015, ‘Pressure injury in Australian public hospitals: a cost-of-illness study’, Australian Health Review, vol. 39, no.3, pp. 329-336.
Payne, D 2016, ‘Strategies to support prevention, identification and management of pressure ulcers in the community’, British Journal of Community Nursing, vol. 21, no. Sup 6, pp. S10-S18.
Prentice J, Stacey M & Lewin G 2003, ‘An Australian model for conducting pressure ulcer prevalence surveys’, Primary Intention, Vol. 11, no.2, pp.87-88.
Santamaria, N, Gerdtz, M, Sage, S, McCann, J, Freeman, A, Vassiliou, T & Knott, J 2015, ‘A randomised controlled trial of the effectiveness of soft silicone multi‐layered foam dressings in the prevention of sacral and heel pressure ulcers in trauma and critically ill patients: the border trial’, International wound journal, vol. 12, no.3, pp. 302-308.
Taylor, B and Kaas, J 2002, ‘Heel ulcers in critical care unit: A major pressure problem’, Critical Care Nurse, Vol.25, pp. 41-53.
Wogamon, CL 2016,’ Exploring the Effect of Educating Certified Nursing Assistants on Pressure Ulcer Knowledge and Incidence in a Nursing Home Setting’, Ostomy/Wound management, vol.62, no.9, pp. 52-60.
Wound, Ostomy and Continence Nurses Society Position Statement on Avoidable Versus Unavoidable Pressure Ulcers’ 2009, Journal of Wound, Ostomy & Continence Nursing ,Vol. 36, Iss. 4, PP. 378-381
Wound, Ostomy & Continence Nurses Society (WOCN) 2016a, Guideline for prevention and management of pressure ulcers (injuries), Mt. Laurel, NJ: Author.
APPENDIX
Pressure Ulcer Knowledge Questionnaire for Health Care Workers
Circle the BEST answer:
Please read the questions carefully before answering. Your answers will be kept confidential.
Date:
PART A:_-
1) Which statement(s) are true about pressure ulcers:
a. They are localized areas of tissue damage
b. They tend to occur at bony sites
c. They are caused by prolonged pressure
d. The patient/resident’s nutrition status affects the development of a pressure ulcer
e. All of the above
2) Which sites are the most susceptible to pressure ulcer development
a. Sacrum and heels
b. Temporal (side)area of the head
c. Soft tissue areas
d. Abdominal area
e. All of the above
3) Which of the following patients/residents would be considered most “at risk” to develop a pressure ulcer
a. A healthy, active 22-year-old new mother
b. A 28-year-old patient in a leg traction
c. An immobile 65-year-old patient who has had a stroke
d. A physically active 80-year-old nursing home resident
e. None of the above
4) To prevent pressure ulcers from developing, which of the following steps should NOT be taken?
a. Routinely observe high-risk bony skin areas
b. Turn patient/residents only upon their request
c. Minimize pressure
d. Keep the skin dry and clean
e. Depending on the patient/resident’s condition, encourage physical activity and a balanced diet
5) In a home health care agency, who should be actively involved in the reduction of a patient/resident’s pressure ulcer?
a. Physician/ Nurse
b. Home health/hospice aides
c. Family members
d. Dietitian/ therapist
e. All of the above
6) A resident/patient is at risk for pressure ulcers when they are or have:
a. Bed or chair bound (immobility)
b. Poor nutritional status
c. Moisture from urine and feces or wound drainage
d. Sensory impairment (such as stroke or dementia)
e. All of the above
7) A pressure ulcer can form in:
a. Less than 2 hours
b. 24 hours
c. 3 days
d. 1 week
e. 2 weeks
8) Residents/patients are assessed for risk of pressure ulcers:
a. On admission, and then routinely
b. When there is a change in condition
c. When we remember
d. When the physician orders it
e. a and b
9) According to best guidelines, residents and patients who are at risk of developing a pressure ulcer should be evaluated for which of the following:
a. Minimizing pressure by repositioning every 2 hours
b. Use of pressure reduction surfaces
c. Nutritional status
d. Incontinence
e. All of the above
10) Which of the following repositioning techniques are key in preventing pressure:
a. Turning residents/patients at least every two hours while in bed
b. Repositioning residents/patients confined to a chair at least hourly
c. Floating heels
d. Padding between bony areas
e. All of the above
PART B
Please circle “True” if you think the statement is true and “False” if you think the statement is false.
11) A pressure ulcer can lead to death True False
12) Donut devices or ring cushions help to prevent pressure ulcers True False
13) Obese patients/residents are rarely malnourished and therefore at lower risk of developing pressure ulcers True False
14) A daily bath or sponge bath will prevent pressure ulcers True False
15) Friction or shear may occur when sliding a person up in be True False
16) A blister on a resident’s/patient’s heel is not a concern True False
17) Bony prominences (areas) should not have direct contact with one another True False
18) Massaging a bony prominence (area) promotes circulation and prevents pressure ulcers True False
Permission Letter
Cite This Work
To export a reference to this article please select a referencing stye below:
Related Services
View all


Related Content
All TagsContent relating to: "Nursing"
Nursing involves providing care for people and families, whether that be during bad physical or mental health, illness or injury. Nurses are compassionate and empathetic, supporting people during their time of need.
Related Articles

DMCA / Removal Request
If you are the original writer of this dissertation and no longer wish to have your work published on the UKDiss.com website then please: