Music Supported Training and Music Listening Interventions on Stroke Patients
Info: 10820 words (43 pages) Dissertation
Published: 9th Dec 2019
Tagged: MusicHealth and Social Care
Introduction: Music supported therapies and listening may provide beneficial motor and cognitive effects following incidents of stroke but there has been no comprehensive synthesis of the available data describing efficacy of both support music listening in stroke.
Areas covered: A systematic review was performed examining the modalities, administration and measured effects of music supported training and music listening interventions on motor and cognitive function applied to post-stroke populations. A total of fourteen published trials were identified. All studies demonstrated pronounced benefits of musical supported training and listening on multiple measures of motricity or cognition. Heterogeneity precluded meta-analysis and all included studies had potential risk of bias. Common reporting or methodological limitations included a lack of blinding, lack of detail on the intervention and safety of reporting.
Commentary: A mounting body of evidence provides the basis for the implementation of music supported therapies as routine treatment for post-stroke populations, yet scant evidence within the music listening division deems it is too early to recommend as a routine treatment, despite its strong implications in ameliorating cognitive dysfunction in the neurological population. Available studies pertain a risk of bias. Accepting these caveats, music listening may have beneficial effects on both mood and cognition and we await the results of ongoing controlled studies.
Introduction.
Burden of disease for stroke.
Stroke represents a major cause of death and the most important cause of acquired disability in adults of developed countries, affecting approximately 6.24 million individuals per year (World Health Organization, 2017) globally. Although there is a steady decline in worldwide death rates related to stroke, it remains the third leading cause of death, and the leading cause of disability in the UK. Around two thirds of stroke survivors have residual neurological deficits that persistently impair function (Greshem et al, 1975), where serious physical, psychological and social impairments entail. Respectively, the personal burden of being a stroke survivor is high. Motor impairments are among the most common and most disabling consequences of stroke (Ward and Cohen, 2004), this limits individual’s participation in daily life activities resulting in a loss of stroke survivor’s independence, exacerbating psychological dysfunction. For this reason, restoration of motor function is a key target of stroke therapy.
Rehabilitation of upper-limb motor dysfunction and total motor dysfunction have been revealed to improve the quality of life of patients after stroke, and are safe and effective methods for restoring social and occupational functioning. Motor dysfunction therapy relies on both pharmacological (Chollet et al, 2011) and non-pharmacological treatments (Samuelkamaleshkumar et al, 2014). Currently, pharmacological therapy is essentially symptomatic and does not have a satisfactory impact on symptoms related to the progression of neurodegenerative diseases. Therefore, several health institutions recommend the development of non-pharmacological complementary interventions as a first-line treatment. For example, intensive motor therapy can improve important motor functions. However, the effectiveness of standard physiotherapeutic approaches in stroke rehabilitation have found to be sub-par in efficacy (Langhammer and Stanghelle, 2000). In the human brain, one of the most powerful sources of auditory stimulation is provided by music. Consequently, more attention has been given to the effectiveness of non-pharmacological approaches in dysfunction therapy, including a growing interest in music therapy and other music-based stimulations.
The necessity for advancements in stroke rehabilitation.
Traditionally, methods of stroke rehabilitation have focussed on providing therapy within the first three months of initial stroke onset, as natural history studies demonstrate a plateau in recovery after this three month period. Recently, this paradigm has been challenged as experiments demonstrate that functional motor gains, and possible neuroplasticity, can occur long after this supposed time window (Szmerda and Bacharach, 1998). Another paradigm that has been challenged in stroke rehabilitation is the modality of rehabilitation intervention that is administered, for example, classical approaches developed by Bobath (1978) have been found to be quite limited. Thus, with the urgent need for more efficacious therapies, data has accumulated indicating that repetition of mass practiced movement’s leads to enhanced motor control (Sterr et al, 2002). An example of this is constraint-induced therapy (CIT), here, the healthy extremity is immobilised whilst the use of the affected paretic extremity is enforced by shaping procedures for several hours a day. Studies in subacute and chronic patients have shown that CIT leads to functional reorganisation in the brain, demonstrated by transcranial magnetic stimulation (TMS) and positron emission tomography (PET) scans (Liepert et al, 1998).
It is this functional plastic reorganisation of neural networks that plays an important role in recovery after brain injury (Kall et al, 2012). Literature on motor learning and recovery indicates that rehabilitation interventions should be meaningful, task specific, tailored to the person’s interests and provide sufficient repetition and challenge to induce training effects. Importantly, animal studies have shown that cortical plasticity is increased by the motivational value and behavioural relevance of the stimulation (Buonomano and Merzenich, 1998). With this in mind, understanding of the brains plastic properties has led to the development of a novel new form of stroke rehabilitation, music supported therapy (MST).
Though the curative effect of music remains uncertain, music easily elicits movement, stimulating interactions between perception and action systems (Zatorre, Chen and Penhune, 2007). Thus, music-making may be an effective way to induce plastic changes in the motor system. Music-supported therapy is a prospective new series of therapy programs, and comprehensive research suggests that it could also be useful because of its promotion of relaxation and of cognitive and motor improvement in post-stroke rehabilitation (Thaut, 2005). Therefore, music-supported therapy has been developed with the aim of improving motor and cognitive recovery after stroke. The definition of music-supported therapy is not only hearing the music but also singing and playing rhythm and percussion instruments and is based on four principles: (i) massive repetition and exercising of simple finger and arm movements; (ii) auditory-motor coupling and integration and reinforcement of motor effects due to immediate auditory feedback; (iii) shaping and adapting the training according to individual progress; and (iv) emotion-motivation effects due to the playfulness and emotional impact of music and the acquisition of a new skill (Ripolles et al, 2015). During motor skill learning, massive practice of movements can reduce kinematic and dynamic execution errors (Krakauer et al, 1999). On the other hand, motor skill training will be more effective if task variability is introduced in the training program, this variability is introduced in MST, whilst not present in CIT. These variations are related to sensorial cues involved in the musical training (multimodality) which leads to dynamic sensorimotor readjustments thus, improvement in motor control. Neuroimaging studies play a crucial role in elucidating the interplay between musical activities and the neural rewiring of the injured brain, a summary of this data is outlined below for both MST and passive music listening, though it is Important to mention that the neurophysiological changes underlying successful musical neurodegenerative dysfunction rehabilitation are not scarcely understood, despite their clinical effectiveness.
Why music? Neurophysiological evidence of music effects.
Music promotes brain plasticity.
Aside from their clinical efficacy, validation of rehabilitation techniques can be evidenced by neuroplasticity, defined as the central nervous systems (CNS) capacity to reorganise its structure, function and connections in response to internal and external constraints and goals during learning, development or after injury (Cramer et al, 2011). Neuroplasticity may be induced by therapy as behaviour can lead to the reorganisation of representational maps (Muellbacher et al, 2002) as well as intra and interhemispheric changes and balance. Over the last decade, researchers have paid a great deal of attention to the neurophysiological basis of musical processing, particularly focussing on the long-lasting effects of fine motor learning, auditory motor coupling and the relationship of emotion and reward in these processes (Koelsch, 2010). This focus has been largely facilitated by neuroimaging studies.
Neuroimaging of non-rehabilitative effects of music playing.
Regarding non- rehabilitative measures, a wealth of evidence has accumulated showing that music playing is a strong inductor of neuroplasticity (Pantev and Herholz 2011; Wan and Schlaug 2010), requiring the processing and integration of multimodal information including auditory, sensorimotor and visual pieces. Long lasting structural and functional changes have been observed in various brain areas, including the sensorimotor cortex, auditory regions, visual spatial areas, the corpus collosum and the hippocampus (Schulze et al, 2009; Seither-Preisler et al, 2014). During the playing process, there are feedback and feedforward interactions between auditory and premotor areas of the cortex. Similar to other motor skills, motor, premotor and supplementary motor areas (SMA) are involved, as well the cerebellum and basal ganglia in musical motor performance, demonstrated by a study involving professional pianists, showing enhancement of fMRI activity in these areas when listening to learned melodies (Bangert et al, 2006). The premotor cortex (PMC) was also enhanced when listening to melodies that were trained 5 days prior. In addition, healthy individuals observed with transcranial magnetic stimulation (TMS) showed an enlargement of the cortical representation of the hand after being trained to play the piano (Pascual-Leone et al, 1995).
Neuroimaging of non-rehabilitative effects of music listening.
Music is the most complex auditory stimulus regarding its breadth of the neural networks involved in its perception and learning (Zatorre, 2013). Beyond the plasticity in motor regions associated to music making, neuroimaging studies have also been used to investigating the effects of music listening in non-rehabilitative settings. Neuroimaging studies of healthy subjects have demonstrated that listening to musicproengages a wide spread bilateral network of temporal, frontal, parietal, cerebellar, and limbic/paralimbic areas, respectively related to the perception of complex acoustic features, syntactic and semantic processing, attention and working memory, episodic and semantic memory, motor and rhythm processing, and emotions and reward processing (Bhattacharya et al, 2001). Since the brain areas involved in music processing are mainly supplied by the MCA cognitive and emotional networks are indefinitely engaged (Ayotte et al, 2000).
Neuroimaging of rehabilitative effects of musical supported interventions.
There is a complex relationship between impairment and function in stroke rehabilitation, where impairment usually reflects the symptom at the level of the damaged structure, the paresis affecting the mobility of the upper extremity is an example of this. As It has been observed that primary motor damage provokes both the diversion of fibers and also the growth of novel brain connections from the ventral premotor cortex to the primary somatosensory cortex (Dancause et al, 2002), again, in rehabilitation these neuroplastic effects are essential in remapping the neurological post-stroke nervous system. Results in a study by Ripolles et al showed that improved hand function is associated with increased activation of ipsilesional motor areas and decreased activation in contralesional regions during movement of the affected hand (2015). In this study, chronic stroke patients showed a decrease in contralesional activation of motor and neighbouring regions after MST. These improvements in motor function are in agreement with previous studies applying MST in subacute stroke patients (Schneider et al. 2007) Connectivity between three pairs of regions changed significantly in this experiment, showing enhanced fMRI activity between: supplementary motor area (SMA)-precentral gyrus (PRG), PRG-inferior frontal gyrus and PAC-SMA. Enhancements in the premotor cortex (PMC), SMA and several auditory and motor regions were also observed, continuous with studies of healthy participants (Bangert et al. 2006). To boot, activity in motor regions ipsilateral to the affected limb (when participants performed a motor task) was significantly reduced after the application of the MST. Furthermore, the involvement of premotor regions and the SMA in the reorganization of the sensorimotor cortex observed is corroborated by animal studies on the effects of brain damage in functional reorganization (Dancause et al, 2002). This wealth of increased neurological understanding supports the impetus for further study in music supported therapies.
Summary and Aims.
The view of the adult brain as a changing and adapting functional and structural core has motivated the design of MST due to music’s distinct neurological affects. Neuroimaging studies have demonstrated that music learning, playing and listening are strong inductors of neural plasticity. Compared to other sensorimotor activities, music learning involves the integrated activity of motor and auditory systems increasing the shaping of movements through the immediate auditory feedback. Moreover, the activation of mesolimbic structures when listening and learning is involved in processing emotions and reward information, adding a component of increased motivational drive to the therapy, a key factor that isn’t present in other therapies. In addition to movement repetition and auditory feedback about the movement precision, the rapid establishment of auditory-sensorimotor corepresentations during the playing process has been hypothesized to underlie the efficacy of this treatment approach, alongside its promotion of relaxation. Thus, the most critical aspect of this research is how these beneficial effects can be translated into therapeutic approaches, treating and rehabilitating the long-term disadvantages in quality of life of stroke survivors.
A recent emergence of clinical trials have shown that post stroke musical training and music listening develop significant improvements over conventional therapies, these improvements include: motor improvements in gait and upper limb function; as well as improvements in cognitive functions including attention, memory and learning (Shauer and Mauritz, 2003; Schneider et al 2007; Sarkamo et al, 2008). These clinical outcomes improving motricity are common outcomes of musical training therapies, whereas passive music listening regimens lead to outcomes within the cognitive domain. Although the general efficacy of music supported therapies has been described in the literature, the content of these music based interventions varies, with great differences in experimental parameters as these interventions have not yet been standardised. Thus, the key aim of this systematic review is to provide description and definitions the modalities and content of music based interventions applied in experiments on stroke groups, as well as describing the significance in improvements of outcomes measuring of motor and/ or cognitive function.
Methods.
Literature search.
A number of primary references accessed from relevant literature searching of electronic databases informs the basis of this systematic review. Research papers were extracted from Doris: Database of Research into stroke and PubMed up to the 17th February 2017. Search strategies approaching these databases entailed the use of appropriate keywords on specific review concepts: “music* supported training”; “music* supported therapy”; ”MST”; ”music”; ”listening”; ”audio” AND “motricity” OR “motor function” OR “cognition”. Results provided randomised control trials (RCT’s), controlled trials (RT’s) and cohort studies. All papers where initially scanned at the abstract level for relevance, whilst inappropriate papers and replicates were removed. The search was broadened by manually selecting references from key articles, as well as identifying specialist researchers in music supported therapies, i.e. Sarkamo to retrieve more available studies. To achieve study eligibility standards, initial inclusion and exclusion criteria were set.
Study selection.
Inclusion criteria: only RCTs, RCs and cohort studies were selected, only studies from 1990 to present were selected. Moreover, studies were only selected that had an intervention period of over 3 weeks, this is because motor outcomes are mostly found within a minimum training volume of three weeks. Exclusion criteria: experiments published in foreign languages were excluded. Furthermore, neurological populations that are not effected by stoke, i.e.: experiments where subjects included Multiple Sclerosis, Parkinson’s disease and Alzheimer’s patients. Studies with musically experienced or deaf subjects were excluded. Experimental stroke populations also had be grouped at a similar level of baseline function, evaluated by their baseline motor function, scoring a minimum of 50 on the Barthel index score or in equivalent tests. Also experiments with less than 3 subjects were excluded.
Data extraction.
After selection determined by inclusion and exclusion criteria, full text articles were then selected by summarising their quality. To do this, a number of data was retrieved to check the experimental eligibility of the given studies, including the aims of the study and study design. As well as this, details were extracted regarding descriptions of participant characteristics and the interventions applied from each study. For participant characteristics, the number of subjects, their age and baseline motor/ cognitive function was recorded. For the description of interventions applied, the name of each music intervention, a description of the intervention, the dosage of each intervention, detailed description of the procedure and session periods as well as the instruments/ technologies used were extracted. To boot, experimental motor/ cognitive outcomes were extracted providing evidence of the given intervention effects, these will be outlined by the pre and post therapy values including their standard deviation, relative to the statistical significance of the intervention. Individual studies provided a range of tests that assess motor/ cognitive outcome and all can be drawn upon when reviewing therapeutic efficacy.
Analysis.
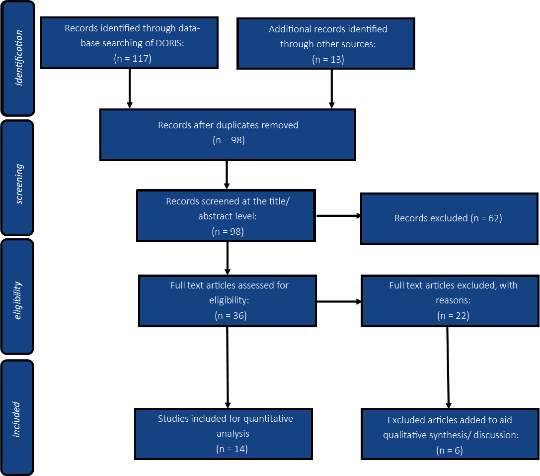
In total, 130 studies were identified in the literature search, 117 records were identified in DORIS and another 13 were provided from PubMed and broader searching, 32 duplicates were then removed followed by the removal of 62 more records after evaluation at the abstract level dependant on inclusion/ exclusion criteria. Further exclusion of 22 records was determined upon evaluating full text articles for their relevance according to the eligibility criteria stated for quantitative analysis. The sum of this data extracted informs the results, providing a basis for description and definition of each therapeutic intervention, as well as providing information on their clinical outcomes. A graphical representation of the flow of citations reviewed and selected for in this research process is demonstrated below as a PRISMA flow diagram (figure 1) below. In addition, summaries of the experimental data is outlined in results table 1.
Figure 1) PRISMA flow diagram outlining the citation selection process.
Results.
Part 1) overview of experimental designs and descriptive analysis of music based interventions.
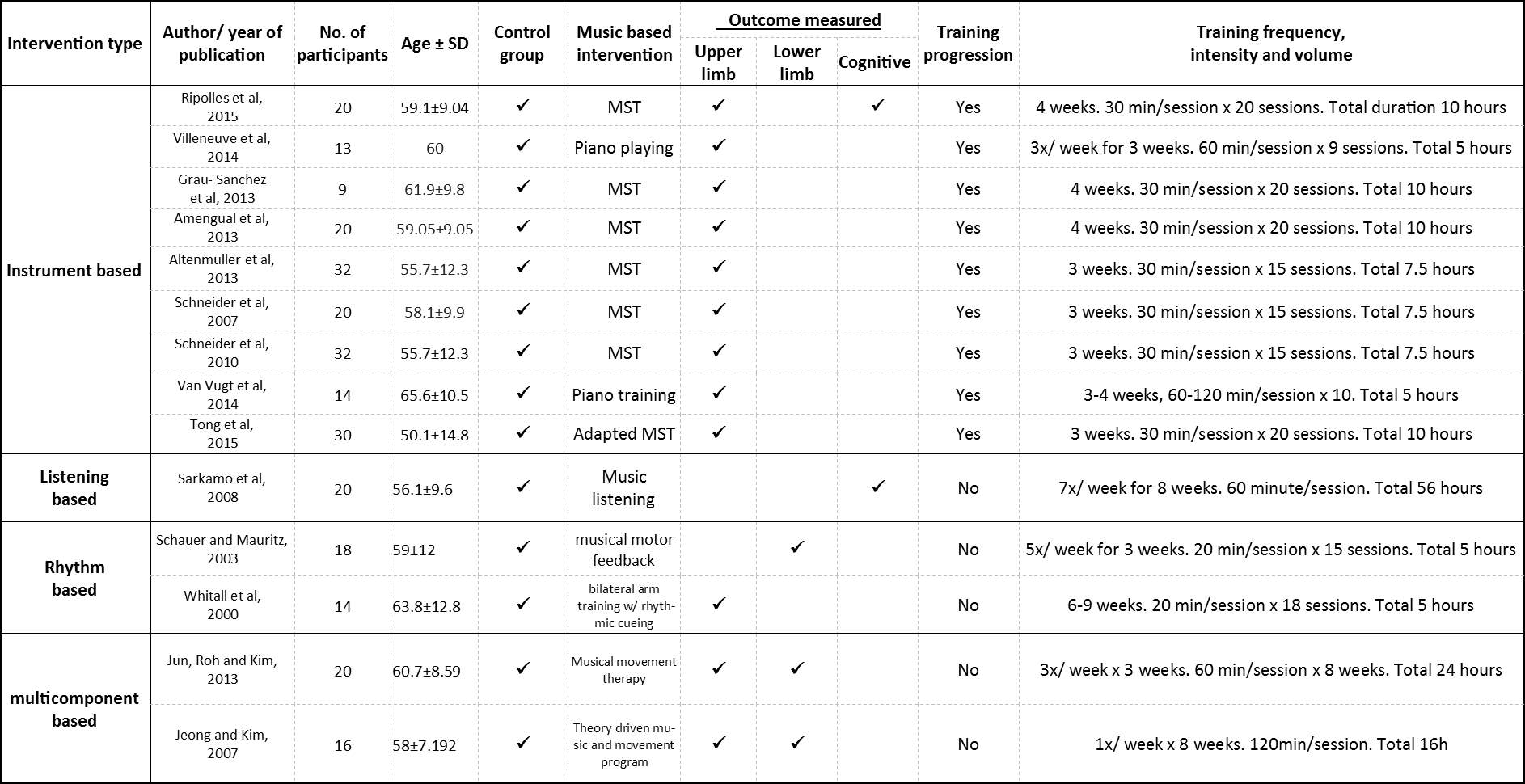
Of the total 14 studies identified, Studies were grouped dependant on the basis of intervention type stated. This resulted into the subdivision of studies into four groups, a total of 9 studies were grouped into instrument based interventions (Ripolles et al, 2015; Amengual et al, 2013; Grau-Sanchez et al, 2013; Altenmuller et al, 2009; Schneider et al, 2010; Schneider et al 2007; Tong et al, 2015; Villeneuve et al, 2014; Van Vugt et al, 2014). A further 2 studies were grouped into Rhythm based interventions (Whitall et al, 2000; Shauer and Mauritz, 2003). 2 more studies were added to a multicomponent based intervention group (Jeong and Kim, 2007; Jun, Roh and Kim, 2013) and a single final study was added to the listening based group (Sarkamo et al, 2009). Of these 14 studies, 3 were CT’s (Amengual et al, 2013; Grau-Sanchez et al, 2013; Jun, Roh and Kim, 2013), 2 were cohort studies (Villeneuve et al, 2014; Whitall et al, 2000), and the remaining 9 are randomised controlled trials. Five of these studies deviated slightly from the typical study design, as studies by Schneider et al and Sarkamo et al were three armed RCT’s (2010; 2009). Moreover, 1 study by Van Vugt et al had two MST groups of stroke patients, one delivered MST within in a group setting, whilst the second group of subjects were provided with MST on an individual basis (2014). Moreover, another study used muted and non-muted instrument design groups (Tong et al, 2015). Here it is important to note that the study by Villeneuve et al did not present data for a control group within one subject study. Finally, studies by Rippoles et al excluded control groups as the experiment was a case control design. In regard of recorded outcomes, studies targeted motor function, cognitive function, or both in one case.
All study designs were applied to stroke patient groups with similar levels of baseline function that all met the eligibility criteria. The allocation of stroke patients was high across studies, and there were no differences found when comparing the outcome measurements stated in the methods compared to those found in the results in the provided studies. Despite this, evaluation of publication bias could not be fully determined as registration of the clinical trials and original experimental protocols could not be found, thus changes between these and the methods stated in the texts selected could not be compared. In musical based interventions it is difficult to conceal the intervention from the participant, thus participant blinding was not used in any of the studies included. Descriptive information regarding participant characteristics, and the applied music based intervention as well as the measured outcome and therapy dosage are represented by Table 1. Below, a descriptive analysis of the content variability within interventions is described:
Instrument based interventions.
This group of intervention was further sub-divided into 3 music group’s dependant on differing modalities. The first group is music supported therapy (MST), the most predominant of sub-divisions which entails 6 studies. The second division provided an adapted form of MST in only one study, the third division consisted of 2 studies that applied training using a piano. The MST group involved the training targeted fine and gross motor functioning in stroke subjects showing mild/moderate paresis if the upper appendage. Both digital piano and drum instruments were used for this training. Access to all piano keys were covered, with the exception of eight white keys reading G, A, B, C, D, E, F and G, the drum kit consisting of 8 pads were also programmed to emit these same notes and sound (Ripolles et al, 2015; Amengual et al, 2013; Grau-Sanchez et al, 2013; Altenmuller et al, 2009; Schneider et al, 2010; Schneider et al 2007).
The adapted MST group varied in instruments used. Here, xylophones and a wooden percussion instruments were utilised. The main difference here is that two sets of conditions were applied, the first set of conditions involved the muting (by using sponge instrument replicas), whilst the second condition used unmuted instruments. Stroke patients with mild/moderate arm paresis played the instruments using appropriate sticks, which were attached to the affected hand if necessary (Tong et al, 2015).
The final 2 studies applied various alternate training protocols using a piano. The first study by Villeneuve et al, utilised a touch sensitive keyboard which had an integrated visual display that cued sequences of note pressings by falling dots determining the necessary time to play the note (2014). Consequent melodies were produced if all correct keys were pressed; if the wrong key/ no key was pressed after the cue, the program and the melody would cease until the correction was made. Subjects were further trained from home, being prompted to practice short sequences learnt during the training sessions using another type of roll up, touch sensitive piano. Another study by Van Vugt et al utilized a light touch M-key V2 musical instrument digital interface keyboard (2014). Simple sequences of children’s songs were learnt in groups or individually to determine if playing in sync with a group had therapeutic effects. The primary aim of the songs provided were to create a large variation in finger movements. Across these studies, difficulty was increased by either increasing the tempo/velocity or changing the variety of finger/hand movements to play the piece, thus, an element of progression was introduced. Training protocols for these groups lasted on average for 3 (range 3-4 weeks). Average training dosage of these sessions was 16 (9-20) sessions lasting for 39 (30-90) minutes, with a total administration of 8.4 (5-10) hours.
Multicomponent based interventions.
Two Multicomponent rhythm based interventions were found for stroke patients, the first (Jeong and Kim, 2007) is a theory driven music and movement program whereas the second is a music movement therapy program (Jun, Roh and Kim, 2013). Said programs combined different musical facets that include: listening to popular music favourable to the subjects taste; singing; playing percussion instruments such as the tambourines and maracas and eliciting movements of the upper and lower appendages to a rhythm. A much more creative form of therapy involving improvisation. Within this group, training protocols were 8 weeks, the average time per session was 90 minutes (ranging from 60-120 minutes), with a the average total of therapy time being 20 hours (ranging from 16-24 hours).
Rhythm based interventions.
Interventions for stroke within this subdivision are defined as studies where the subject’s motor movements were elicited as a reaction to music serving as an auditory stimulus. The first study by Whitall et al entailed the use of a bilateral arm trainer apparatus, this made use of two separate T-bar handles that moved in the direction of the transverse plain (2000). The subject would sit in the predetermined stance where the ankles, shoulders and wrists were in neutral position relative to the knees and hips being placed at 90° and the elbows in flexion at 60°. Sitting perpendicular to the apparatus, subjects would then push (extend) and pull (flex) the apparatus in sync to a musical metronome. The second study by Shauer and Mauritz provided subjects with portable music players (2003). Personally chosen pieces of music where then adjusted in tempo to approximately 10% above and below the subjects spontaneous cadence during gait. Progression was applied by increasing musical tempo relative to increases of subjects’ spontaneous cadence. Subjects were then prompted to walk when listening to the modulated musical pieces. Training protocols for these groups consisted of 3 or 6-9 weeks respectively, sessions were 20 minutes in duration for both groups with the total administration time being five hours.
Listening based interventions.Despite a great availability of music listening interventions on immediate remediation of symptoms, only one viable study was found in the literature search demonstrating the effects of listening after a three week administration period (Sarkamo et al, 2009). This intervention provided stroke subjects with portable music players, studying the effect of music listening compared to control groups who either listened to audio books or received standard care. The intervention protocol entailed one hour per listening session a day, carried out over an 8 week period with a total of 60 hours.
Table 1) Descriptive information regarding participant characteristics, and the applied music based intervention as well as the measured outcome and therapy dosage.
Part 2) outcome measurements recording the effects of music based interventions on motor function, cognition or both.
Motor outcome measurements used within instrument based intervention studies.
Measurements within this group for the upper limb were measured using various tests, these include: the arm paresis score (APS); the Jebsen hand function test (JHFT); the finger to nose test (FTNT); the action research arm test (ARAT); the nine-hole peg test (NHPT) and the box and clock test (BBT). In addition, computerised analysis of movement was utilised, quantifying: finger and hand tapping frequency and velocity, supination and pronation, reaching frequencies, velocities and distances.
For the studies within this group that used MST, significant increases were recorded for finger tapping and velocity tests, NHPT, ARAT, BBT and APS compared to control groups administered with conventional therapy/ constraint induced therapy. A single study by Ripolles et al also tested for cognitive outcomes, significant improvements were recorded in Stroop test C, trial marking test A, and the Ray auditory verbal learning test (RAVLT)(A1-A5) compared to control groups within the experiment. Other studies regarding the use of instruments also outline significant improvements in upper extremity measures over respective control groups. These statistical differences amongst music based studies are outlined below in Table 2 and 3. A comprehensive legend disregarding abbreviations already made in the text is detailed below the final table of the results section, Table 7.
Table 2) Effects of instrument based interventions, comparing experimental and control groups amongst studies.
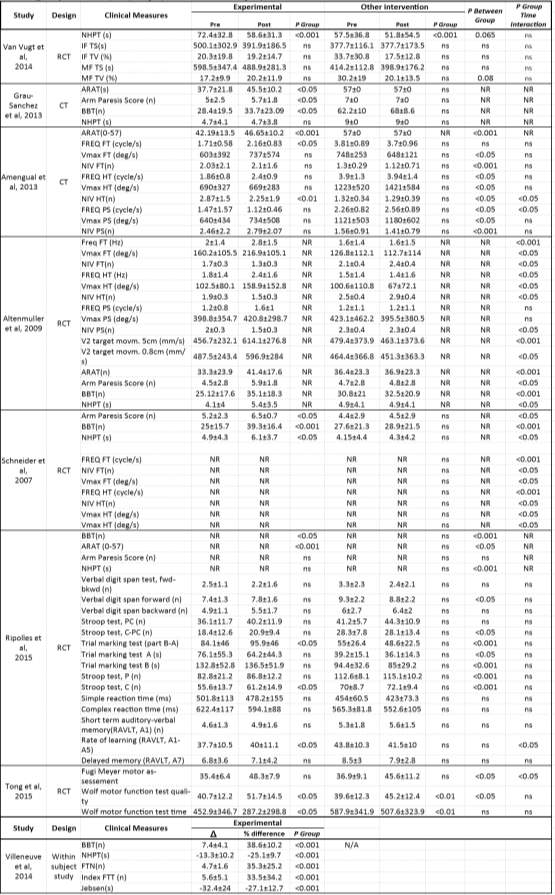
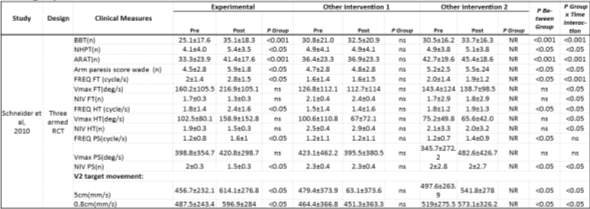 Table 3) Effects of instrument based interventions, comparing experimental and control groups in a 3 armed RCT.
Table 3) Effects of instrument based interventions, comparing experimental and control groups in a 3 armed RCT.
Mobility outcome measurements used within rhythm based intervention studies.
Here, spatio-temporal parameters of gait were measured, this was done by measuring pre and post therapy values of: velocity, stride length and time, double support, cadence and symmetry deviation for the single study. The second rhythm based study used various measurements regarding upper appendage movement.
Significant increases were recorded for gait velocity, stride time and cadence in the experimental group over the control non-musical control groups, where no statistical differences were found. These statistical differences amongst rhythm based studies are outlined below in Table 4.
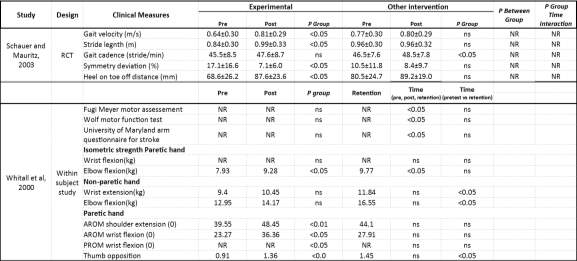 Table 4) Effect of rhythm based interventions, comparing experimental and control groups amongst studies.
Table 4) Effect of rhythm based interventions, comparing experimental and control groups amongst studies.
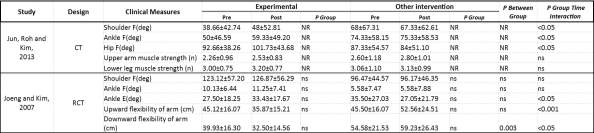
Various outcome measurements used within multi-component based intervention studies.
Within multicomponent based interventions, goniometric measurements of range of motion (ROM) were recorded for the shoulder, for elbow flexion, ankle flexion and extension. Muscle strength and upwards and downwards reach were also measured to determine flexibility. The Fugi Meyer motor assessment scale and the Wolf motor function tests were also applied to this group.
Experimental subjects demonstrated significant increases in ROM of both the shoulder and elbow, as well as hip flexion relative to the control group. To boot, significant increases in arm flexibility and ankle extension were also noted. These statistical comparisons amongst multi component based studies are outlined below in Table 5.
Table 5) Effect of multi-component based interventions, comparing experimental and control groups amongst studies.
Cognitive outcome measurements used within a listening based and instrument based study.
Regarding a solely listening based study by Sarkamo et al as well as an instrument based study by Ripolles et al that also recorded cognitive outcomes, significant changes in cognitive outcome were measured. Here, neurophysiological batteries were applied testing for: language, verbal memory, short and long term working memory as well as music cognition, visuospatial cognition, executive function and focused and sustained attention.
The study entailing only music listening showed significant increases in multiple parameters with respect to both control groups of audiobook listening and no intervention. Levels of focused attention was measured by the sum of correct responses and reaction times of the Cognispeed mental subtraction and Stroop tests. Moreover, verbal memory was measured the story recall subtest from the Rivermead Behavioural memory test and a word list teaming task. These statistical differences for cognitive outcomes are outlined below in Table 6 and 7.
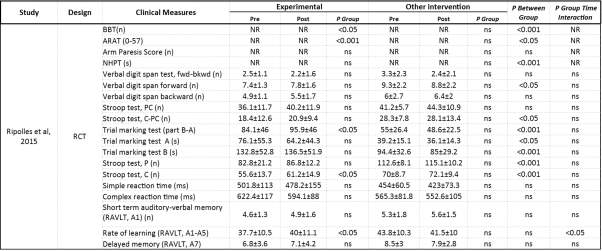 Table 6) Effect of listening based interventions, comparing experimental and control groups.
Table 6) Effect of listening based interventions, comparing experimental and control groups.
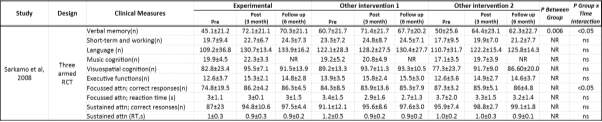 Table 7)Effect of an instrument based intervention in a 3 armed RCT.
Table 7)Effect of an instrument based intervention in a 3 armed RCT.
Legend
(Respective of table 1-7).
Data is presented as X ± SD.
Abbreviations: ns= not significant; NR= not reported; n= number; s=seconds; m= meters; min=minutes; mm= millimetres; deg=degrees; Δ =delta; F= flexion; E=extension; IF TS= index finger tapping speed; IFTV= index finger tapping variability; MFTS= middle finger tapping speed; MFTV= tapping variability; FREQ FT= finger tapping frequency; VMAX FT= finger tapping average angular velocity; NIV FT= finger tapping number of inversions of velocity; FREQ HT= hand tapping frequency; VMAX HT= hand tapping average angular velocity; NIV HT= hand tapping number of inversions of velocity;
FREQ PS= pronation and supination frequency; VMAX PS= pronation and supination average angular velocity; NIV PS= pronation and supination number of inversions of velocity; V2=maximum velocity of wrist; T25FW=timed 25 foot walk; FTN=finger to nose test ATTN= attention; FWD= forward; BKWD=backward.
Summary.
In summary, experimental results from this plethora of studies demonstrate a significant improvement in both motor and cognitive stroke symptoms over conventional therapies (CIT) and respective control groups (not receiving music). No significant group interaction over time was found in the study by Van Vugt et al, which contrasted MST delivery in group’s settings or in turn individually (2014). Demonstrating no difference of efficacy in group activity. For the study by Jeong and Kim, significant group over time improvements were observed for non-muted and muted musical groups, respectively (2007). Although the sum of this data is most prevalent for improving motricity, a lack of long-term listening based interventions prevent a competent analysis of this modalities rehabilitative efficacy, despite significant improvements of cognition within the group.
Discussion.
Key findings of the project.
The above analysis demonstrates that music based interventions have a strong clinical efficacy for the rehabilitation of both motor and cognitive functions within post-stroke neurological populations. The methods within this review extracted a range of therapy modalities differing in type, frequency, duration, dosage and outcome measures. For this reason studies were grouped respective of the interventions basis being either: Instrument, rhythm, multi-component or listening based for ease of reference and intervention dependant outcomes. Although most evidence is provided for motor outcomes, very few of these studies have focussed on the intertwined and complex improvement of cognitive function that is also a pronounced outcome of musical based therapies. Rather than this, specific study clinical outcomes were measured relative to the specific treatment administered. For example, the evaluation of hand and finger tapping velocity, variability and frequency measurement outcomes was applied to piano training groups, (Van Vugt et al 2014) as well as upper extremity function being measured within parameters of the BBT, APS, ARAT, NHPT and various other tests/scores evaluating the overall movement characteristic of the upper appendage within instrument based groups. One rhythm based study measured improvements of gait parameters (Schauer and Mauritz, 2003). Although all yielding significant improvements of studied motricity compared to control groups, only one listening and one instrument based intervention measured cognitive improvements. Despite less evidence being provided in the cognitive domain, the interventions recorded significant increases in attention, rate of learning. Verbal, short and long term memory, language, music and visuospatial cognition, executive function, and focussed and sustained attention respective to controls (Sarkamo et al 2008; Rippoles et al, 2015). Measurement of cognitive outcomes across all studies would be of great insight for stroke rehabilitations considering that motor impairment leads to further exacerbations of cognitive, emotional and behavioural symptoms.
Limitations of the project.
Across all studies, the stroke patient groups did not differ in demographic and clinical variables at the baseline of dysfunction, thus, rehabilitation effects received upon intervention can be directly attributed to the recorded clinical outcome of studies. Despite this, care still needs to be taken when interpreting the data given the potential impact of spontaneous recovery within stroke groups as well as other activities that may constitute rehabilitative aspects, this is only a minor limitation on the study considering intervention periods are relatively short and controls groups are present. Furthermore, in their own right, interventions across groups yield significant improvements over their control groups supporting the implication of musical supported therapies in the rehabilitative field of stroke. Unfortunately, the results were not generalizable across studies, thus, an all-inclusive, detailed recommendation scheme for therapy cannot be made and a meta-analysis was not performed. This was due to a number of limitations, as outlined below:
- Multi-component interventions utilizing many musical aspects including, these interventions are difficult to generalise in comparison with other groups as there was not a uniform therapy design, entailing content that was dealt with in an unstructured and improvisational manner.
- Some studies did not apply appropriate outcome measures to demonstrate the interventions full effect, for example, the study assessing gait parameters after walking to an auditory stimulus by Shauer and Mauritz did not apply appropriate measurements to evaluate balance or bimanual dexterity and coordination (2003).
- Only two studies applied some measurements to cognitive function, where the bulk of data concentrates on outcomes within the motor domain, leaving too few results for fair analysis of long term therapeutic effects within the cognitive domain.
- Effect sizes were not accounted for in the searching process weakening the basis on which statistical analysis can be provided.
- Importantly, heterogeneity, even in studies with similar experimental protocols was observed between the modality of the interventions, the outcome measurements used to demonstrate rehabilitative effects as well as a large variability between the number of experimental subjects and quantity of experimental groups/control groups. For example.
- Finally, although the stroke patient groups did not significantly differ in pathology relative to a baseline dysfunction, the pathophysiology of stroke patients substantially differs between each subject, effecting differences between recovery and ability, thus, this heterogeneity within its class has been noted.
- Despite satisfactory sample sizes across the majority of studies, only one study had an unsatisfactory sample size, determining it inapplicable for wider statistical analysis (Grau-Sanchez et al, 2013).
How findings fit with the current knowledge.
At large, the results provided in this review are principally consistent with the discussions of previous non-systematic studies, which highlight that musical supported therapies including instrument, rhythm, multi-component and listening based interventions as standardises therapies provide improvements within motor and cognitive domains (Altenmuller and Shlaug, 2015; Francoise et al, 2015). This study differed from that in the literature by systematically reviewing both effects of music supported interventions and listening interventions as well as describing their modalities.
Music performance is a dual task action requiring output of motor systems and simultaneous feedback by auditory and visual stimuli requiring the processing of the new skill entailing complex components involving rhythm and pitch. With respect to neurobiological mechanisms, it is thought that audio-motor coupling (AMC) may constitute a major element of the efficacy of music supported training. This is because a high speed mechanism is needed to during performance to control complex movement patterns regulated by continuous auditory feedback. Neuroimaging studies as mentioned have shown that audio-motor integration at cortical and sub-cortical levels must be elicited. During the learning and training phase, audio-motor coupling (AMC) is established and can be compared to the oral-aural loop in language processing (Schneider et al, 2010). Recent studies in supporting the rapid effects of AMC in novice subjects making music further supports the efficacy shown in music based therapies of neurological subjects (Bangert and Altenmuller 2003; Lahav et al 2007). Importantly, gross motor movement measurements of supination and pronation of the forearm in the study by Schneider et al demonstrated no significant improvements in MST over the control groups, as these movements are not associated with the instrument playing nore the music playing paradigm of both the piano and drums (2010). On the other hand, musically associated measurements of finger and wrist movements brought about significant improvements, highlighting the importance of complex movement regulated by auditory feedback in rehabilitative efficacy.
Despite the limited yet significant studies measuring the long term effect of listening based therapies on cognitive outcome, multiple short term studies on the immediate effects of music listening and the amelioration of cognitive symptoms corroborate with the outcome measures demonstrated in this review (Sarkamo et al, 2008). Music listening has a well document list of short term effects including the alleviation of anxiety, depression and pain in patients with somatic illness (Cepeda et al, 2006). Moreover, recent neuropsychological studies suggest that listening enhances a variety of cognitive functions, including attention, learning, communication and memory in both healthy subjects (Schellenberg et al, 2007), and in clinical conditions for stroke (Belin et al, 1996). In addition, administration of nonverbal auditory stimuli has provided temporary amelioration of left visual neglect post-stroke (Hommel et al, 1990). As shown, music listening can undoubtedly elicit cognitive improvements regarding many symptoms of stroke across multiple studies, despite the limitations regarding long term studies found in this study.
Suggestions for future work.
In the future, it will be interesting to understand further advancements in neurophysiological, neurophysiological and audiological fields which will eventually determine the components of music that constitute towards functional reorganisation in the brain. Thus, continued developments between these fields provides a mechanism in which the therapy is ever developing. A mounting body of evidence for AMC is a leading theory amongst others that leads to this reorganisation within the brain, yet there is much more to understand within these emerging fields of study. As learning is strengthened by expressive interactions, which is motivating and rewarding constitutes towards music based interventions therapy. For the reason, the investigation of the effect of different types of auditory stimuli (music and metronome) should entail.
Having described the contents of the intervention modalities, this review serves as a useful impetus for future researchers and therapists when planning their study designs, regarding their specific measurement outcomes in order to combat the relative symptoms that need to be treated within patient groups. To boot, as progression is an underpinning factor to effective therapy, these studies can be applied in clinical settings with the possibility of progression in future works.
Conclusion.
To conclude, the key finding presented within this study supports the pertaining view within the literature that novel therapies including both music listening and music training based therapies provide significant improvements of outcome measures within both cognitive and motor domains. This was established from an effective literature search extracting key studies based on eligibility criteria. Details regarding treatment modalities and measured outcomes have been descripted, which can also direct clinicians when tailoring therapeutic programs to treat specific neurological outcomes. This specificity is respectively of use, but in combination with the experimental limitations, an impetus is provided working towards controlled study designs to further elucidate music effects on subjects, outlining and understanding musical therapy as a whole. Importantly, this data is grounded by the effect of enhanced neuroplasticity to neurological populations, thus, these interventions can also be applied to similar pathology groups in clinical settings to other neurological diseases including Parkinson’s and Multiple Sclerosis. Progression availability in more clinical settings will only pronounce rehabilitative efficacy.
Music learning is a special process as it involves key elements of mass movement repetition, AMC, integration and reinforcement of motor effects from auditory feedback and shaping and adapting towards individuals progress, as well as the shaping and adapting the training according to individual progress; emotion-motivation effects are elicited due to the playfulness and emotional impact of music and the acquisition of a new skill. These conjunctive effects are not provided in current clinical settings where constraint induced therapies and standard physiotherapy is routinely administered.
The efficacy of music based interventions is thought to be due to the fact that these sensorimotor activities involve the integrated activity of motor and auditory systems, activating numerous brain networks, thus a leading theory for rapid plastic reorganisation is auditory-motor coupling, amongst other theories.
Fortunately, as demonstrated in this text, neurophysiological data has historically provided a basis for the development of therapies being applied to neurodegenerative populations, thus, the interaction between the growing fields of musicology, neuroimaging, neurophysiology and neurorehabilitation will continue to aid this therapy, especially considering overall bleak outcomes for the stroke patient.
Despite the risk of bias and recorded limitations within the study, the effects of a long term listening intervention have not been largely studied. Although the provided still provides significant improvements for the amelioration of language, memory, attention, cognition and executive function; other studies discluded from this review boast a plethora of pronounced cognitive outcomes as mentioned. Suggested that everyday music listening during early stroke recovery offers a valuable addition to the patients care, especially if other active forms of rehabilitation are not yet feasible at this stage, by providing an individually targeted, easy to conduct and inexpensive means to facilitate cognitive an functional recovery, thus, when approaching stoke rehabilitation, the provision of regular self-administered music listening should be provided within an optimal treatment regimen.
Bibliography.
Altenmuller, E. & Schlaug, G. (2013) Neurobiological Aspects of Neurologic Music Therapy. Music and Medicine [online]. 5 (4), pp. 210-216. [Accessed 03 February 2017].
Altenmüller, E., Marco-Pallares, J., Münte, T. & Schneider, S. (2009) Neural Reorganization Underlies Improvement in Stroke-induced Motor Dysfunction by Music-supported Therapy. Annals of the New York Academy of Sciences [online]. 1169 (1), pp. 395-405. [Accessed 03 February 2017].
Amengual, J., Rojo, N., Veciana de las Heras, M., Marco-Pallarés, J., Grau-Sánchez, J., Schneider, S., Vaquero, L., Juncadella, M., Montero, J., Mohammadi, B., Rubio, F., Rueda, N., Duarte, E. & Grau, C. et al. (2013) Sensorimotor Plasticity after Music-Supported Therapy in Chronic Stroke Patients Revealed by Transcranial Magnetic Stimulation. PLoS ONE [online]. 8 (4), pp. 618-683. [Accessed 03 February 2017].
Ayotte, J., peretz, i., Rousseau, I., bard, c. & bojanowski, m. (2000) Patterns of music agnosia associated with middle cerebral artery infarcts. Brain [online]. 123 (9), pp. 1926-1938. [Accessed 03 February 2017].
Bangert, M. & Altenmüller, E. (2003) Mapping Perception to Action in Piano Practice: A Longitudinal DC-EEG Study. BMC Neuroscience [online]. 4 (1), pp. 26. [Accessed 2 March 2017].
Bangert, M., Peschel, T., Schlaug, G., Rotte, M., Drescher, D., Hinrichs, H., Heinze, H. & Altenmüller, E. (2006) Shared networks for auditory and motor processing in professional pianists: Evidence from fMRI conjunction. NeuroImage [online]. 30 (3), pp. 917-926. [Accessed 03 February 2017].
Belin, P., Zilbovicius, M., Remy, P., Francois, C., Guillaume, S., Chain, F., Rancurel, G. & Samson, Y. (1996) Recovery from nonfluent aphasia after melodic intonation therapy: A PET study. Neurology [online]. 47 (6), pp. 1504-1511. [Accessed 03 February 2017].
Bhattacharya, J., Petsche, H. & Pereda, E. (2001) Interdependencies in the spontaneous EEG while listening to music. International Journal of Psychophysiology [online]. 42 (3), pp. 287-301. [Accessed 04 February 2017].
Bobath, B. (1978) Adult Hemiplegia: Evaluation and Treatment. 2nd ed. London: William Heinemann Medical Books Ltd.
Bunketorp Käll, L., Lundgren-Nilsson, Å., Blomstrand, C., Pekna, M., Pekny, M. & Nilsson, M. (2012) The effects of a rhythm and music-based therapy program and therapeutic riding in late recovery phase following stroke: a study protocol for a three-armed randomized controlled trial. BMC Neurology [online]. 12 (1). [Accessed 03 February 2017].
Buonomano, D. & Merzenich, M. (1998) CORTICAL PLASTICITY: From Synapses to Maps. Annual Review of Neuroscience [online]. 21 (1), pp. 149-186. [Accessed 04 February 2017].
Cepeda, M., Carr, D., Lau, J. & Alvarez, H. (2006) Music for pain relief. Cochrane Database of Systematic Reviews [online]. 19 (2). [Accessed 05 february].
Chollet, F., Tardy, J., Albucher, J., Thalamas, C., Berard, E., Lamy, C., Bejot, Y., Deltour, S., Jaillard, A., Niclot, P., Guillon, B., Moulin, T., Marque, P. & Pariente, J. et al. (2011) Fluoxetine for motor recovery after acute ischaemic stroke (FLAME): a randomised placebo-controlled trial. The Lancet Neurology [online]. 10 (2), pp. 123-130. [Accessed 04 February 2017].
Cramer, S., Sur, M., Dobkin, B., O’brien, C., Sanger, T. & Trojanowski, J. (2011) Harnessing neuroplasticity for clinical applications. Brain [online]. 135 (4), pp. 216-216. [Accessed 04 February 2017].
Dancause, N., Ptito, A. & Levin, M. (2002) Error correction strategies for motor behaviour after unilateral brain damage: short-term motor learning processes. Neuropsychologia [online]. 40 (8), pp. 1313-1323. [Accessed 03 February 2017].
François, C., Grau-Sánchez, J., Duarte, E. & Rodriguez-Fornells, A. (2015) Musical training as an alternative and effective method for neuro-education and neuro-rehabilitation. Frontiers in Psychology [online]. 6. [Accessed 04 February 2017].
Ghez, C., Krakauer, J. & Ghilardi, M. (1999) Independent learning of internal models for kinematic and dynamic control of reaching. Nature Neuroscience [online]. 2 (11), pp. 1026-1031. [Accessed 05 February 2017].
Grau-Sánchez, J., Amengual, J., Rojo, N., Veciana de las Heras, M., Montero, J., Rubio, F., Altenmüller, E., Münte, T. & Rodríguez-Fornells, A. (2013) Plasticity in the sensorimotor cortex induced by Music-supported therapy in stroke patients: a TMS study. Frontiers in Human Neuroscience [online]. pp. 1-11. [Accessed 03 February 2017.
Gresham, G., Fitzpatrick, T., Wolf, P., McNamara, P., Kannel, W. & Dawber, T. (1975) Residual Disability in Survivors of Stroke – The Framingham Study. New England Journal of Medicine [online]. 293 (19), pp. 954-956. [Accessed 04 February 2017].
Hommel, M., Peres, B., Pollak, P., Memin, B., Besson, G., Gaio, J. & Perret, J. (1990) Effects of Passive Tactile and Auditory Stimuli on Left Visual Neglect. Archives of Neurology [online]. 47 (5), pp. 573-576. [Accessed 05 February 2017].
Jeong, S. & Kim, M. (2007) Effects of a theory-driven music and movement program for stroke survivors in a community setting. Applied Nursing Research [online]. 20 (3), pp. 125-131. [Accessed 06 February 2017].
Jun, E., Roh, Y. & Kim, M. (2012) The effect of music-movement therapy on physical and psychological states of stroke patients. Journal of Clinical Nursing [online]. 22 (1-2), pp. 22-31. [Accessed 06 February 2017].
Koelsch, S. (2010) Towards a neural basis of music-evoked emotions. Trends in Cognitive Sciences [online]. 14 (3), pp. 131-137. [Accessed 06 February 2017].
Lahav, A., Saltzman, E. & Schlaug, G. (2007) Action Representation of Sound: Audiomotor Recognition Network While Listening to Newly Acquired Actions. Journal of Neuroscience [online]. 27 (2), pp. 308-314. [Accessed 04 February 2017].
Langhammer, B. & Stanghelle, J. (2000) Bobath or Motor Relearning Programme? A comparison of two different approaches of physiotherapy in stroke rehabilitation: a randomized controlled study. Clinical Rehabilitation [online]. 14 (4), pp. 361-369. [Accessed 04 February 2017].
Liepert, J., Miltner, W., Bauder, H., Sommer, M., Dettmers, C., Taub, E. & Weiller, C. (1998) Motor cortex plasticity during constraint-induced movement therapy in stroke patients. Neuroscience Letters [online]. 250 (1), pp. 5-8. [Accessed 04 February 2017].
Muellbacher, W., Richards, C., Ziemann, U., Wittenberg, G., Weltz, D., Boroojerdi, B., Cohen, L. & Hallett, M. (2002) Improving Hand Function in Chronic Stroke. Archives of Neurology [online]. 59 (8), pp. 1278. [Accessed 14 March 2017]. [Accessed 06 February 2017].
Pantev, C. & Herholz, S. (2011) Plasticity of the human auditory cortex related to musical training. Neuroscience & Biobehavioral Reviews [online]. 35 (10), pp. 2140-2154. [Accessed 05 February 2017].
Ripollés, P., Rojo, N., Grau-Sánchez, J., Amengual, J., Càmara, E., Marco-Pallarés, J., Juncadella, M., Vaquero, L., Rubio, F., Duarte, E., Garrido, C., Altenmüller, E., Münte, T. & Rodríguez-Fornells, A. (2015) Music supported therapy promotes motor plasticity in individuals with chronic stroke. Brain Imaging and Behavior [online]. 10 (4), pp. 1289-1307. [Accessed 06 February 2017].
Ripollés, P., Rojo, N., Grau-Sánchez, J., Amengual, J., Càmara, E., Marco-Pallarés, J., Juncadella, M., Vaquero, L., Rubio, F., Duarte, E., Garrido, C., Altenmüller, E., Münte, T. & Rodríguez-Fornells, A. (2015) Music supported therapy promotes motor plasticity in individuals with chronic stroke. Brain Imaging and Behaviour [online]. 10 (4), pp. 1289-1307. [Accessed 06 February 2017].
Samuelkamaleshkumar, S., Reethajanetsureka, S., Pauljebaraj, P., Benshamir, B., Padankatti, S. & David, J. (2014) Mirror Therapy Enhances Motor Performance in the Paretic Upper Limb After Stroke: A Pilot Randomized Controlled Trial. Archives of Physical Medicine and Rehabilitation [online]. 95 (11), pp. 2000-2005. [Accessed 07 February 2017].
Sarkamo, T., Tervaniemi, M., Laitinen, S., Forsblom, A., Soinila, S., Mikkonen, M., Autti, T., Silvennoinen, H., Erkkila, J., Laine, M., Peretz, I. & Hietanen, M. (2008) Music listening enhances cognitive recovery and mood after middle cerebral artery stroke. Brain [online]. 131 (3), pp. 866-876. [Accessed 05 February 2017].
Cite This Work
To export a reference to this article please select a referencing stye below:
Related Services
View all


Related Content
All TagsContent relating to: "Health and Social Care"
Health and Social Care is the term used to describe care given to vulnerable people and those with medical conditions or suffering from ill health. Health and Social Care can be provided within the community, hospitals, and other related settings such as health centres.
Related Articles

DMCA / Removal Request
If you are the original writer of this dissertation and no longer wish to have your work published on the UKDiss.com website then please: