Family Planning Knowledge and Attitudes in The Gambia
Info: 14791 words (59 pages) Example Dissertation Proposal
Published: 3rd Dec 2021
Tagged: Health
Contents
Click to expand Contents
CHAPTER I
1.1 BACKGROUND
1.2 STATEMENT OF PROBLEM
1.3 JUSTIFICATION OF THE STUDY
1.4 RESEARCH QUESTION
1.5 RESEARCH HYPOTHESIS
1.6 SIGNIFICANCE OF THE STUDIES
1.7 SCOPE
1.8 OPERATIONAL DEFINITIONS
1.9 CONCEPTUAL FRAMEWORK
CHAPTER TWO
2.0 LITERATURE REVIEW
2.1 FAMILY PLANNING UTILIZATION
2.3 KNOWLEDGE OF FAMILY PLANNING
2.3 ATTITUDE
2.4 PRACTICE
2.5 REASONS FOR NOT USING MODERN CONTRACEPTIVES
CHAPTER 3
3.0 METHODOLOGY
3.1 BACKGROUND OF STUDY AREA
3.2 STUDY POPULATION
3.3 STUDY DESIGN
3.4 DURATION OF THE STUDY
3.5 SAMPLE SIZE DETERMINATION
3.6 SAMPLING METHOD
3.6 SELECTION CRITERIA
3.7 VALIDITY AND RELIABILITY OF INSTRUMENTS
3.8 DATA COLLECTION TOOLS
3.9 DATA COLLECTION PROCESS
3.10 DATA PROCESSING AND ANALYSIS
3.11 ETHICAL CONSIDERATIONS
3.12 DISCUSSION
3.13 STRENGTH AND LIMITATION
BUDGET
BUDGET NARRATION
Appendix
PARTICIPANT INFORMATION SHEET
Who has reviewed this study?
Consent / Assent Form
QUESTIONNAIRE
REFERENCES
CHAPTER I
1.1 BACKGROUND
Family Planning help individuals and couples to anticipate and attain their desired number of children in addition to the spacing and timing of their births. This is achieved by using modern contraceptive methods. Family planning encompasses a wide range of services such as sex education, prevention and management of sexually transmitted infections, preconception counseling and management and infertility management1.
The use of family planning services have realized a steady increase in many countries of the world. According to WHO, despite the positive increase there are still over 200 million women worldwide who would like to avoid a pregnancy but are not using an effective method of contraception due to reasons like lack of supplies, cultural, political barriers and poor quality of services2.
According to the United Nation’s Family Planning Fund(UNFPA), about 64 % of women of reproductive age (15-49), married or in a union, are using some form of contraception, either modern or traditional3. The report further revealed the current contraceptive prevalence rates (CPR) as 68.5%in Asia, 51.5% in Arab States, 65% in Eastern Europe and Central Asia,72.6% in Latin American and the Caribbean, 38.6 in Eastern and Southern Africa and the least West and Central Africa with 17.63. It has been observed that there has been a decline in the prevalence of induce abortion from 1995. As at 2008 the prevalence of induced abortion globally was 28%3. The study further revealed the trends in various region of the world as; Africa 29%, Asia 28%, Europe 27%,Latin America 32%, Northern America 19% and Oceania 17%3.
Adolescents are an important resource of any country. There is no universally accepted definition of adolescence bracket. WHO definition of adolescent is anyone between the ages of 10 and 19 years4. It is recognized that many of the health related behaviors that arises during adolescence has implications for the present and future health and development 5. This age group account for 1.8 billion of the world’s population .Adolescents comprises 20% of the world’s total population and the rapid changes in the population growth are realized in developing countries6.
The changing moral, social values and shift in the standard of societal behavior from conservatism to liberal interaction between both sexes is attributed largely to exposure to the media especially television and movies. Adolescents find themselves sandwiched between a glamorous western influence and a stern conservatism at home, which strictly forbids discussion on sex. This dichotomy aggravates the confusion among adolescents7. This has led to increase in premarital sexual activity, pregnancy among unmarried girls apart from the increasing incidence of abortion & Sexually Transmitted Infections7.
Despite the global reduction in maternal deaths, pregnancy related mortality remains the second leading cause of death among adolescent girls age 15-19 years8. There are a lot of factors contributing to these death such as unsafe abortion, obstructive labors because of the size of their pelvic. It was also found out that adolescents don’t have access to information about their sexuality and reproductive health and as a result, they are less likely to seek for or utilize reproductive health services. Adolescence pregnancy is a major public health problem because it does not only increase their risk of instrumental delivery, obstetric complications like obstructed labor and obstetric fistulae but it also increases their risk of having a poor pregnancy outcome for both the mother and the baby 8. Adolescent also have a higher risk of dying from pregnancy related causes when compared to older women because their pelvis and reproductive organs are not fully developed to begin reproduction.
According to the United Nation Family Planning Fund (UNFPA) pregnancies among girls below 18 years have irreparable consequences and some of these consequences are; it violates the rights of girls, life-threatening consequences in terms of sexual and reproductive health, and poses high development costs for communities, particularly in perpetuating the cycle of poverty. Early pregnancy will have negative affect on their education, health needs, increase risk of violence in the society, increase HIV infection and maternal deaths and disability9.
In The Gambia adolescents constitute 23% of the population, approximately 386 thousand and like their peers in other developing countries, they are faced with early physical maturation10. As a result, many of them venture into early unprotected sexual activities which predisposes them to unintended and often unwanted pregnancies 10.The consequences of unwanted pregnancy include, unsafe abortion practices which exposes them to pelvic inflammatory diseases, ectopic pregnancy, and secondary infertility, baby-dumping, sexually transmitted infections, including HIV/AIDS, involvement in drug use and abuse 11. However, even though there are no data on the impact on the consequences of limited Family Planning services to students, the uptake of family planning services is very low12.
Young people’s sexual rights are denied by both religious and traditional forces in the Gambia which promotes early marriage and stigmatizes premarital sex and pregnancy outside marriage. Misinformation about sex and lack of youth friendly sexual and reproductive health services also poses challenges to the sexual and reproductive health of young girls13 .
1.2 STATEMENT OF PROBLEM
There are 1.8 billion young people between the ages of 10-24 in the world and this cohort of age bracket is the fastest growing in most of the developing countries 14 This is a time when they are at a crossroad most especially concerning sexual and reproductive health where they have limited information.
Lack of sexual reproductive health information and service has led to many health problems. Globally, there are more than 2 million 10-19 year old living with HIV and about one in seven of all new cases of HIV infection occurred during adolescence 14.
Young people’s reproductive health is often over looked. Health facilities frequently fail to provide young adult with specialized reproductive health information and counseling services despite the fact that they are increasingly exposed to reproductive health risks. It is estimated that about 16 million girls aged 15-19 and 1 million girls under the age of 15 give birth annually and most of the births occur in low and mid-income countries 15.
Complications during pregnancy and childbirth are a common cause of death among young girls in developing countries. It is established that complication during pregnancy and childbirth are the 2nd leading killer of females and young women in developing countries,16.
The social setting has a negative toll in the adolescents’ sexual and reproductive health. In many settings, sex is not a matter of discussion in the home. In rural Gambia, students are considered to be “small children” who are not expected to have sex17. This type of thinking poses a barrier to access and makes reproductive health services not student youth-user-friendly. These research findings will be used to establish the existing gap between the adolescent and provision of reproductive health services and it will help to improve adolescent reproductive health.
According to UNFPA, 23.3 million women were helped to have access to modern family planning services and also bout 700 million condoms and other commodities were procured in 201518. The turnover of their investment averted 34,000 maternal deaths,12.3 million unintended pregnancies, 4.4 million abortions including 3.9 million unsafe abortion and 220,000 child death18.
1.3 JUSTIFICATION OF THE STUDY
The rationale of the study on students is that they make part of the adolescent cohort that are neglected in the health care system. The Gambia health demography survey (2013) reveals that the adolescent birth rate is 88.1%. This further shows that 18% of the adolescent women aged 15-19 are already mothers or pregnant with their first child19. This trend is similar to the figures within the sub-Saharan Africa sub region13.
A study on intervention to improve adolescents’ contraceptive behavior in low and middle income countries revealed that 15% of maternal death in sub-Saharan African happens among adolescents between the ages of 15 to 19yrs 16.
A study conducted among university students in Saudi Arabia identified that young people are faced with a number of risks to their sexual and reproductive health including adolescent pregnancy, sexual violence, and unmet family planning 20.
Lack of adequate knowledge and utilization of sexual and reproductive health services by secondary school students is a big public health challenge most especially when government looks forward to reduce maternal and child morbidity and mortality in the Gambia. Generally, adolescents’ sexual and reproductive health issues are neglected in service delivery and research in the Gambia. Most of the literature reviewed doesn’t really attempt to find out students’ knowledge, attitude and utilization of sexual and reproductive health services. The findings of his study will pave the way towards addressing issues related to their sexual and reproductive health. The rate of Sexual &Reproductive Health services by students is not known nor does the barriers for non-use of contraceptives is known.
According to World Young Women’s Christian Association about 68% of sexually active unmarried adolescents have an unmet need for modern contraceptive in Sub-Saharan Africa including Gambia11.
The 2013 Gambia Health Demography Survey (DHS) revealed that contraceptive use was lower among all women than among currently married women. It further showed that sexually active unmarried women are by far the most likely to be using contraception. If the 2013 HDS is to be compared with previous surveys it was evident that family planning uptake and continuity is on the decline in the country19. It is evident that the uptake of family planning is disproportionate across the various regions with Banjul being the highest and Upper River Region having the lowest19.
Unplanned and unwanted pregnancy among unmarried adolescents is a challenge for many developing countries including The Gambia. Currently in the Gambia there is no comprehensive program that addresses the reproductive health needs of adolescents leading to lack of accurate and appropriate sexual information that will prevent them from unplanned pregnancy21.
A report by the Ministry of Health and Social Welfare, The Gambia revealed that about 18% adolescent women age 15 to 19 are already mothers or pregnant with their first child22. The report further revealed that rural teenagers are twice more likely to have their first child earlier than urban girls22.
Currently, there is very limited data on students’ knowledge and utilization of sexual and reproductive health services in the Gambia thus this study will form the bases for further research in this area.
The goal of the study is to compare the knowledge, attitude and practice on family planning among rural and urban secondary school students in the Gambia. The specific objectives are (1) to determine the knowledge of secondary school students on family planning (2) To assess the attitude of secondary school student on family planning service (3) To identify practices of family planning services among students.
1.4 RESEARCH QUESTION
The study intends to answer the following research question;
- What is the level of family planning knowledge among secondary school students in the Gambia?
- Are there any difference between urban and rural secondary school students regarding family planning knowledge and attitude?
- What are the students’ sources of information regarding family planning?
- What is the level of practice family planning among secondary school students in the Gambia?
- Are there any difference between urban and rural secondary school students regarding prevalence of family planning?
1.5 RESEARCH HYPOTHESIS
The hypothesis of the study is geographical location has no effect on knowledge and attitude of students on family planning.
Geographical location has no effect to access and uptake of family planning services.
1.6 SIGNIFICANCE OF THE STUDY
Sexual and reproductive health problems like Abortion, risky sexual practice, unwanted pregnancy, Sexually Transmitted Infection (STI) and sexual violence are common phenomena among students and very little research have been conducted to present the magnitude of the problem. Therefore, this assessment is believed to give the present image of reproductive health related issues among of the students within the study area, which may help the concerned authorities to take necessary actions based on the findings. The study may also provide baseline information for further studies that may be conducted in similar issues.
1.7 SCOPE
This study will be conducted only on secondary schools in Region II & IV Education Directorates of The Gambia. The target population is all students attending secondary school education in these two regions.
Gambia has six regional education directorates. A simple random sampling was employed. Two regions were picked and they happened to be Region II&IV.
These two education regions were randomly selected using simple random sampling technique. The names of all the regional education directorates in The Gambia were written on small pieces of papers. The balloting started by picking the urban directorate. The Gambia has two urban regional education directorates, the names of the two directorates were balloted and region II was picked.
The rural regional education directors are four in number. The balloting procedure employed in selecting the urban regional education directorate was used and region IV was selected.
1.8 OPERATIONAL DEFINITIONS
Knowledge: is awareness and understanding that one has gained on reproductive health issues through learning and practice and respondents was considered to be knowledgeable if he/(s) correctly answered greater than or equal to 70% of the total knowledge assessing questions .
Attitude:The way of thinking to which family planning should be provided to and an intention to use family planning services in the future
Practice: Utilization of at least any family planning services
1.9 CONCEPTUAL FRAMEWORK
The conceptual framework to be used in the study will be the Health Belief Model (HBM) The HBM is a cognitive, interpersonal framework that views humans as rational beings who use a multidimensional approach to decision-making regarding whether to perform a health behavior. The model is appropriate for complex preventive and sick-role health behaviors such as contraceptive behavior.
Putting in mind that family planning is a dynamic and complex set of services, programs and behaviors towards regulating the number and spacing of children within a family. Contraceptive behavior, refers to activities involved in the process of identifying and using a contraceptive method to prevent pregnancy and can include specific actions such as contraceptive initiation, continuation or discontinuation, misuse, nonuse, and more broadly compliance and adherence
1.9.1 Constructs of the HBM for Family Planning
The constructs of the Health Belief Model which will influence the utilization family planning are being discussed below.
Perceived Susceptibility and Severity
The perceived possibilities of an unwanted pregnancy and its associated problems provides the incentive to use contraception. This considers personal feelings of the seriousness of becoming pregnant, based upon subjective assessment of medical and social consequences of pregnancy and childbearing most especially in a conservative society where people frowns at outside wedlock pregnancies. This construct may include factors like fear of body changes or pregnancy complications, or worry of quitting school, which can impact the likelihood of contraceptive use23.
Perceived Benefits
Perceived benefits relate to the perceived effectiveness, feasibility and other advantages of using a contraceptive method to prevent pregnancy vis-à-vis the perceived barriers. Through a cost-benefit analysis, the perceived ratio of a contraceptive’s benefits to its barriers helps determine the preferred and specific contraceptive action and method23.
Perceived Barriers
Perceived barriers are negative consequences of using contraception. This dimension includes factors such as perceived side effects of hormonal contraception. These fears have been found to be potential reasons why people may not use contraceptive .Disadvantages have been found to inhibit contraceptive use23.
Cues to Action
These are internal and external stimuli that trigger a consciousness of the perceived pregnancy threat and facilitate consideration of using contraception to remedy the threat. This may include symptoms like missed menses after intercourse (internal stimuli) or contraceptive communication from the media, and worry from a sexual partner or counseling by a health care provider23.
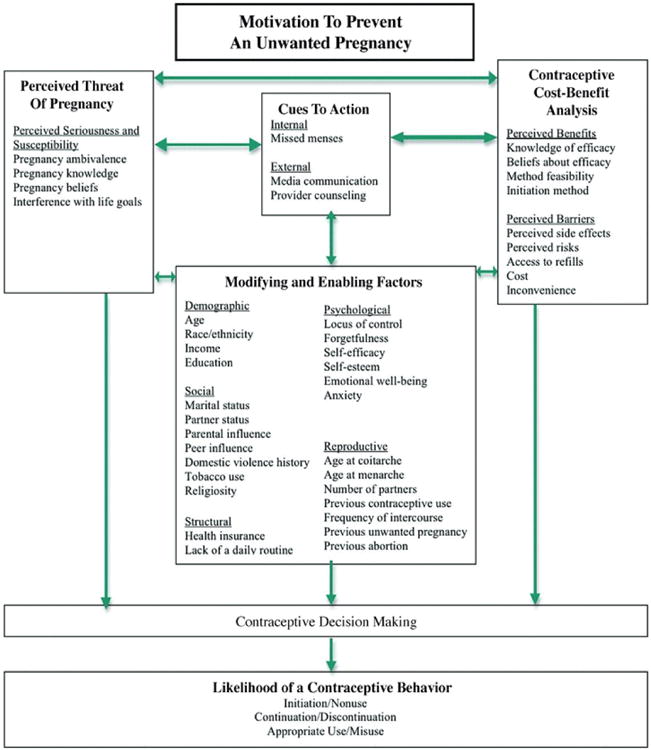
Figure 1. Constructs of the Health Belief Model, as Applied to Contraceptive Behavior
Source: Glanz et al, 2002, p. 52
CHAPTER TWO: LITERATURE REVIEW
Family planning is one of the great public health achievements in the 20th century. Family planning allows people to attain their desired number of children and determine the spacing of pregnancies. It is achieved through use of contraceptive methods and the treatment of infertility. Promotion of family planning and ensuring access to preferred contraceptive methods for women and couples is essential to securing the well-being and autonomy of women, while supporting the health and development of communities 1.
The other benefits of family planning among others are:
Preventing pregnancy-related health risks in women
When a woman can make an informed choice whether to be pregnant or not, it has a direct bearing on her health and the wellbeing of the entire family. Family planning allows the spacing of pregnancies and can delay adolescents from becoming pregnant thus reducing their risk of pregnancy related health issues and death from early childbearing. It prevents unwanted pregnancies and unsafe abortion consequences. Family planning enables women who wish to limit the size of their families to do so. Evidence suggests that women who have more than 4 children are at increased risk of maternal mortality (1).
Reducing infant mortality
Family planning can prevent closely spaced and ill-timed pregnancies and births, which contribute to some of the world’s highest infant mortality rates. Infants of mothers who die as a result of giving birth also have a greater risk of death and poor health(1).
Helping to prevent HIV/AIDS
Family planning reduces the risk of unintended pregnancies among women living with HIV, resulting in fewer infected babies and orphans. In addition, male and female condoms provide dual protection against unintended pregnancies and against STIs including HIV (1).
Empowering people and enhancing education – Family planning enables people to make informed choices about their sexual and reproductive health. Family planning represents an opportunity for women to pursue additional education and participate in public life, including paid employment in non-family organizations. Additionally, having smaller families allows parents to invest more in each child. Children with fewer siblings tend to stay in school longer than those with many siblings1.
Reducing adolescent pregnancies
Pregnant adolescents are more likely to have preterm or low birth-weight babies. Babies born to adolescents have higher rates of neonatal mortality. Many adolescent girls who become pregnant have to leave school. This has long-term implications for them as individuals, their families and communities1.
2.1 FAMILY PLANNING UTILIZATION
According to World Health Organization contraceptive use has increased in many parts of the world, especially in Asia and Latin America, but continues to be low in sub-Saharan Africa15. Globally, use of modern contraception has risen slightly, from 54% in 1990 to 57.4% in 2014. In Africa it went from 23.6% to 27.6%, in Asia it has risen slightly from 60.9% to 61.6%, and in Latin America and the Caribbean it rose slightly from 66.7% to 67.0%15Use of contraception by men makes up a relatively small subset of the above prevalence rates. The modern contraceptive methods for men are limited to male condoms and sterilization (vasectomy).
A study carried out in Ikeji Arakeji, Osun State, Nigerian showed that women with higher education are more likely to plan their families, have fewer children, have better access to health services, and experience less maternal mortality24.
Unmet need family planning is defined as “those who are fecund and sexually active but are not using any method of contraception, and report not wanting any more children or wanting to delay the next child. The concept of unmet need points to the gap between women’s reproductive intentions and their contraceptive behavior”25.
WHO estimated 225 million women in developing countries would like to delay or stop childbearing but are not using any method of contraception. Reasons for this include25:
- limited choice of methods;
- limited access to contraception, particularly among young people, poorer segments of populations, or unmarried people;
- fear or experience of side-effects;
- cultural or religious opposition;
- poor quality of available services;
- users and providers bias
- gender-based barriers.
The unmet need for contraception remains too high in many parts of the world. In Africa, 23.2% of women of reproductive age have an unmet need for modern contraception while in Asia, Latin America and the Caribbean – regions have relatively high contraceptive prevalence – the levels of unmet need are about 11 %25.
2.3 KNOWLEDGE OF FAMILY PLANNING
Knowledge on family planning services is an important step toward gaining access to contraceptive methods and using a suitable method in a timely and effective matter26. A survey conducted in in Osun State, Nigeria revealed that all ever-married and currently married women (100% each) know at least one method of family planning 26. The survey showed that people with little or no education and poor have the least knowledge about family planning26. The same survey showed that geographical location has an effect on knowledge on family26. It showed urban men have better access to family planning information through the mass media than rural men26. Additionally, education had a positive association with access to family planning information through the media.
A study in Tanzania showed that 98% of Tanzanian population have access to family planning information27. Despite the fact that there is high level of awareness, utilization of family planning services is a challenge since only 29% of women actually used the services27. If men are to be compared to women, the latter is more knowledgeable because most of the interventions are women focused.
In Lesotho, a study revealed that almost all the participants 99.2% had knowledge of one family planning method28.
A study carried out by the Nova Scotia Gambia Association (2009) revealed that students concerned about HIV/AIDS in Central River Region of the Gambia was high but other STIs was as low as 2.4% , 17.
For adolescents to lead a healthy, responsible, fulfilling lives and protect themselves from reproductive health problems, they need to be knowledgeable about themselves and need adequate information about the physical, psycho-logical changes that take place during puberty, menstruation, pregnancy and child birth29.
Inadequate knowledge remains a major barrier for adolescents: An in-depth study of four Sub-Saharan African countries found that 60% or more of adolescent men and women believed common misperceptions or had poor knowledge about the prevention of unintended pregnancy and HIV; one-third or more did not know of a source for contraceptives 30.
Among adolescents wanting to avoid pregnancy, the chance of having an unintended pregnancy is much lower if they and their partner use a modern contraceptive rather than a traditional method or no method at all 30.
A study carried out in Ethiopia showed that lack of knowledge of family planning was found to be another important reason for nonuse among women with unmet need. The study revealed that close to one third of the women surveyed had no knowledge of a source for a method or did not know of a method 31. This showed that knowledge can greatly influence the uptake of family planning services.
Lack of awareness about contraceptive methods may be a reason for not using contraception among Egyptian women32. The study further revealed that Egyptian women did not prefer discussing sexual related problems with men physician due to culture and religion32.
Lack of knowledge of modern contraceptive methods and their mechanism of action have been cited as one of the major reasons for the women’s nonuse of contraception33.
A study on Knowledge, Attitude and Practice on family planning among married women in Banteay Meanchey, Cambodia revealed that 99.3% among the respondents have heard about contraceptives regardless of educational level and socioeconomic status. Almost all the study participants heard about family planning and knew at least one modern family planning method. Despite the study revealed high knowledge of contraceptives among respondents, the knowledge varies from one method to another. The most known method by the participants were pills and injectable contraceptive, which accounted for 95% and 83% respectively. The other mentioned methods were the condom and IUD 34. The same study showed that most of the participants source of information about family planning was healthcare staff (67.4%),TV (50.7%) radio (35%) and then friends (33%)34.
As study to assess Knowledge, Attitude and Practice of family planning among health care providers in two local governments in Osun State, Nigeria showed that not all health care providers are knowledgeable about family planning method. Less than half knew all the methods most especially the new methods35. This can negatively affect their performance as they will not be able to discuss all methods or opportunities to their clients.
A study in Pakistan showed that the level of knowledge among women was 60%. Most of the knowledgeable were residing in the urban areas of Pakistan36. Adequate knowledge on family planning can be a catalyst for an increased utilization of the services.
A study assessing Knowledge, Attitude and Practice on Family Planning among married women in India shows that all the participants were knowledgeable of FP methods. The findings were higher for female sterilization, followed by use of condom and the least was traditional family planning methods. These findings should be taken with caution because of the fact that the study was within an urban setting with favorable conditions such as health training center, proactive health professionals and other information sharing enhancing facilities37.
A study assessing the awareness and practices of contraceptives was conducted among university students in Botswana and it revealed 58.6% and 59.1% of male and female respectively had good knowledge regarding family38. Furthermore, the study revealed that all the female students (100%) in the study were aware that contraceptives are not 100% effective as compared to 93.7% of the male students38. Finally, the study revealed that 90.6% of females knew that using contraceptives irregular will lead to pregnancy as compared 76.4% of their male counter parts38. The most common known family planning method was the condom 95.6% followed by the contraceptive pills 86.7%.38
A study conducted among students in Brazil revealed that 95% of the study participants were familiar with at least one method of family planning39. It further revealed that the most common method of family planning known by was the male condom39.
A study on knowledge, perception and practice of family planning among staff and students in Niger Delta University, Delta State, Nigeria showed that 84% of the participants had good knowledge of family planning40. The study revealed that 44% believed that family planning help to maintain the desired number of children a couple want, 19.6% said it allow women pursue their career while 18.7% felt it promotes promiscuity40.
2.3 ATTITUDE
Studies revealed that students’ attitude affects their knowledge of sexual and reproductive health 41.Sexual attitude and behaviors of adolescents is significantly sharpened by socio-psychological factors and consequently affect their knowledge of contraception 41. According to them, young adults need better sex education and greater access to family planning services.
A study conducted in Egypt showed that 75% of the women who were nonusers said they intended to use family planning in the future and 81% of the women who had discontinued using family planning intended to use it in the future 32. This shows that most of the women’s attitude towards family planning is very causal.
A student on knowledge, attitude and practice among married women in Banteay Meanchey, Cambodia, indicated that the women preferred to discuss family planning with their neighbors, husbands, doctors and close friends. Less than 10% of respondents had discussed family planning with other family members. A little more than half (52%) of the respondents considered family planning to be concerned with the health of the mother and child while 35% considered family planning to have specific issues on women’s health. Almost all respondents showed positive attitudes in discussing family planning, some respondents disapproved unmarried or single women discussing contraception. 34
A study conducted by the University of Lahore, Pakistan showed that 54% of women have positive attitude and approved family planning36. In a study in India, it was revealed that 83.1% of the participants had a positive attitude towards family planning and out of these about 75% of them were satisfied with the services they have received. This positive attitude towards family planning is reechoed by 5% who are thinking of switching to other types of family planning methods37.
A study among university students in Botswana revealed that about 66% of the study participants revealed that they had engaged in sexual intercourse38. Interestingly, the study showed that the majority of the sexually actively participants were using contraceptive and out of these a quarter were not regularly38.
2.4 PRACTICE
A survey carried out in China among migrant young adults, showed that 28.0% and14.2% of males and females respectively had pre-marital sex experiences, but only 47.4% of them used condoms, including 16.1% who used condoms half the time and only 4.0% used condoms every time42. The study further revealed that the proportion of study participants’ who actually used condoms was very low due to factors such as perceptions of risk, embarrassment, and cultural aspects of condom use42.
A study in Tanzania among adolescents showed that 59.2% of the study participants were encouraged to use family planning services by their parents compared with 11.7% who were encouraged by their religious leaders. Only 5.6 % of respondents had sought family planning services. The study revealed that females were more likely than males to report contraceptive use 55. 6% and 44.4% respectively. Out of those that reported to have sought for family planning services only 44.4% do so whenever they planned to have sex. The most commonly used contraceptive by males was the condom and females was the injection 27.
A study carried out in Pakistan showed that knowledge doesn’t correlate with practice. The study shows reasonable high awareness level and a very low service uptake, but despite only 17% of married women of reproductive age used modern contraceptives 43.
A study in West Ethiopia on the utilization of family planning showed 78.9% rural and 84.7% of urban rural women had ever used family planning service44. The study further revealed that urban women are more likely to used family planning services than rural women44.
There are many factors that prevent people from utilization of family planning services. Factors like desire for male children, religious reasons and the disapproval of partners45.
Religion and cultural believes plays a critical role in people’s acceptance and use of family planning methods. A study analyzing family planning utilization in India showed that Muslim women have greater opposition to family planning33.
Misconception was one of the reasons for non-use of contraception for fear of infertility. Many women believed that if they use family planning over a long period there are higher chance that when they needed to have children it may be very difficult 33.
A study in Cambodia revealed about 68% of respondents had previously used some modern contraceptive methods and 56% of respondents were using contraception at the time of the study. Among the current users, the majority were pill users (44.6%) followed by those using injection method (38%); and only about 8% of respondents said that they were using condoms. Other methods mentioned were Implants, IUD and female sterilization34.
A study in India showed that 61.3% of the study participants were using one method of family planning. It was also observed that as advance in age, educational level, family size and age of last child had a bearing in the uptake of family planning services37.
A study among staff and students of Niger Delta University on knowledge, perception and practice on family planning showed that 31% of the respondents used condom, 22.9 % used oral pills, 7.6% used the withdrawal method, 4.2% used implants, 3.6% used post-coital pills40. The respondents’ reason for choosing the above family planning methods were safety, reliability and accessibility40.
2.5 REASONS FOR NOT USING MODERN CONTRACEPTIVES
Many factor are responsible for nonuse of family planning commodities. A study in Cambodia highlighted side effects of the pill and contraceptive injection, and the desire for more children, as the main reasons for not using modern contraceptives34. Some respondents indicated disapproval husbands and relatives, husbands were often working away from home and sex was infrequent so contraceptive use became unnecessary; use of traditional calendar methods; and personal perception among respondents that the women themselves were not at risk of pregnancy34.
A study carried out by University of Lahore, Pakistan showed similar reasons for non-use of family planning services as the study carried out in Cambodia, however the one in Pakistan made emphasis on lack of knowledge about the sources of services36
A study conducted in Ghana revealed that adolescents faced with some barriers in accessing family planning services. These barriers among others were cost of services, societal perceptions of adolescents patronizing FP being spoilt, and adolescents’ fear of healthcare providers being judgmental, discriminatory and may not abide by the principles of privacy and confidentiality during FP service provision to adolescents. Shyness and intimidation were also highlighted to be another barrier to access, resulting from societal and healthcare provider attitudes46.
Factors for non-use of family planning varies from one region to another. A study carried out on factors influencing the uptake of family planning services in Talensi District of Ghana showed that the major constraint of women for non-used of family planning is that they cannot take decisions for themselves without the approval of their husbands, perceived misconceptions about family planning services such as family planning is meant for only married people, harmful to the womb47.
A study conducted in West Ethiopia revealed reasons why some study participants were not utilizing family planning services44. Most of the participants mentioned fertility related reasons such as breastfeeding and not having sex44. Some women were not utilizing family planning because of opposition from husbands or relatives while some it was because of religious reasons44.The study further showed that sometimes potential family planning users preferred not to use more reliable methods due to misconception and concerns about their health which is compounded by lack of adequate knowledge of family planning methods44.
CHAPTER 3: METHODOLOGY
3.1 BACKGROUND OF STUDY AREA
The research will be conducted in two Regional Education Directorates of the Ministry of Basic and Second Education of The Gambia. The two regions are Regions II and IV.
The Gambia is located midway on the bulge of the West Africa coast and stretches over 400 kilometers inland from west to east on either side of the River Gambia, varying in width from about 50 km near the mouth of the river to about 24 km upstream19. The country is surrounded on its three sides by the Republic of Senegal and to the west by the Atlantic Ocean19. The River Gambia runs through the entire length of the country19. The country has a land area of 10,689 square kilometers19.
The preliminary results of the 2013 population census showed that 1.9 million of which women comprises of over half of the country’s population19. About 57% of the population living in the urban areas which makes it more densely populated than the rest of the country19. The country is divided into 5 regions (West Coast, Lower River, Central River, Upper River and North Bank Regions), and two municipalities (City of Banjul and Kanifing Municipality) that constitute the Greater Banjul Area19.
There are five major ethnic groups and approximately 90% of the population are Muslim.19
The education system in The Gambia is a continuum from early childhood development (ECD) to university education with three years of pre-school education, nine years of uninterrupted basic education, three years of secondary education and four years of tertiary and higher education48. It was until 2007 a second ministry of education was created.48. Following the creation of a second ministry, the mandates to deliver education and training have now been segregated between the two ministries of education, namely: The Ministry of Basic and Secondary Education (MoBSE) and The Ministry of Higher Education, Research, Science and Technology (MoHERST)48.
The study will be conducted in Region II and IV.
Region II Education Directorate covers the West Coast Region. The region spans from Kartong to Kanlagi. It has a population of 699, 706 and an annual growth rate of 6.1%12. The male population is slightly higher than that of the females; 50.2% for male and the rest females12. The region has 1 hospital, 2 major health centre, 8 minor health centers and private clinics49. Region II has one hundred and seventy secondary schools and a student population of 54,69850.
Region IV Education Directorate covers Lower River Region. The region stretches from Jattaba to Pakaliba. The region has a population of 82,361 and the population distribution of males and females is 48.2% and 51.8% respectively. The region has 1 major health center, and 4 minor health centers49. Region IV spans from Jataba to Pakaliba. It has 28 secondary schools and a student population of 564950.
The study will be conducted in two different Regional Educational Directorates. The two directorates are Regions II&IV. Region II in this study will be considered urban area while Region IV as rural.
Regional Education Directorate II and IV were randomly selected using simple random sampling technique. Region II representing the urban while Region IV rural.
3.2 STUDY POPULATION
According to the Ministry of Basic and Secondary Education in The Gambia, there are 128 Juniors Secondary School Students in the two regions (117 in WCR & 11 LRR) and 60 senior secondary schools (53 in WCR & 7 in LRR). The total number of students in the junior secondary schools is 40,550 and 19,797 in the senior secondary schools50.
For representativeness, a proportional sampling will be conducted in all the schools for the purpose of this study.
3.3 STUDY DESIGN
A descriptive cross-sectional study design will be conducted to assess the KAP on Family Planning of Secondary School Students and observe whether geographical location has an effect on the KAP in Region II&IV Education Directorates of the Gambia.
Self-administered questionnaire and FGD will be used to collect with the aid of trained research assistants.
Focus Group Discussions (FGDs) qualitative method will used to compliment and validate the quantitative data collection. Twelve FGD sessions will be held in school selected for the study.
A focus-group session is an in-depth discussion in which a small number of people (usually 8-12) from the target population discuss topics that are of importance for a particular study or project51. It is advisable the participants for the FGD are homogeneous with respect to characteristics 51. The advantage of this method is that it method that determines attitudes, experiences, perceptions, and knowledge on a wide range of topics in many fields of endeavor. Focus groups lead to the voicing of attitudes and insights not readily attain able from other qualitative forms of data collection like the individual interview and the weaknesses of this method are that the effect of group dynamic can affect the interaction of the participants 52. Some of the participants may dominate the discussion while others may not participate in the discussion which may affect the findings, as the reflections and opinions of those not taking part will not be captured. Another weakness of the method is the social context in which it is conducted, because participants may not feel comfortable to openly talk about their experiences or opinions on the issue being discussed without being judged or ridiculed by other members of the group. The presence of some members in the group may intimidate some participants and they may conform to the dominant ideas that are presented 52.
3.4 DURATION OF THE STUDY
The study will take five months that is from December 2016 to May 2017. Refer to the Gantts Chart in the appendix.
3.5 SAMPLE SIZE DETERMINATION
Sample size will be calculated using the formula;
p=the proportion of research participants with adequate knowledge, attitude and practice (50% is assumed here since there is no known prevalence)
q=1-p
d=the degree of accuracy desired set at 0.05. Thus the minimum sample size with a design effect will be 769. Due to the sensitivity of the questions in the data collection tool, a 10% non-respondents rate will be considered, hence a total of 846 students will constitute the study sample.
3.6 SAMPLING METHOD
A multi-stage sampling technique will be used to recruit study participants for this study. First, a simple random sampling method will be used to select two regional education directorates from the six education directorates in The Gambia. In the second stage, in each of the selected education directorates schools will be randomly selected for the study. A total of twelve secondary school will be selected. The third will also a simple random sampling to identify the classes/grades that will be recruited for the study. Grade 7 to Grade 12 students will be recruited for the study.
A sample of 846 students will be recruited in the study out a study population of 60347 Secondary School Students. A proportional sampling will be conducted to ensure representation of 10 secondary schools that will be selected. Out of the 846, 90% of sample population will be allocated to Region II Education Directorate while the rest for Region IV Education Directorate. The list of the schools in the study and the number of students will be accessed by MoBSE.
3.6 SELECTION CRITERIA
The inclusion criterion is such that only students enrolled in the selected schools irrespective of age and sex.
The study excludes students that are absent on the day of data collection.
3.7 VALIDITY AND RELIABILITY OF INSTRUMENTS
The researcher with the help of the supervisor(s) will develop a questionnaire based on research objectives. The questionnaire will be peer reviewed (face validity) by the supervisor(s) and experts in family planning. The developed questionnaire will be pretested for reliability and validity at a different regional educational directorate.
The outcome of the questionnaire will greatly depend on how well the research participants understand the questions and their understanding may be affected by language skills, education and culture 53 . Pre-testing starts of reviewing and revising questions process53. The aim of pre-testing is to evaluate whether respondents interpret questions in a consistent manner, as intended by the investigator, and to judge the appropriateness of each included question,53
A total of 100 participants will be recruited for this purpose. The length of each of the 30 interviews would be timed. Ideally the length of each interview will not take more than 30 minutes.
After the pretesting of the questionnaire, SPSS package Version 20 will be used to statistically test the validity and reliability of the questionnaire.
3.8 DATA COLLECTION TOOLS
The Questionnaire in Appendix 1 will be used to collect data on the above mentioned variables. A Focus Group Discussion checklist will be used to collect the more information on the knowledge, attitude and practice. All tools will be pre-tested in a different regional education directorate for readability, understanding, and clarity.
The selected data collectors will be fluent in the local dialects in case there is a need to translate for the understanding of the students and during training they will translate the questionnaire back and forth for understanding and clarity.
3.9 DATA COLLECTION PROCESS
Study Permission – will be sought from Ethics Committee, Science Committee, the Ministry of Basic and Secondary Education, Regional Education Directors and the School principals, (see appropriate Appendix for each). The data collection will proceed with the permission of all the above, and the students are free to withdraw their permission at any time of the study if they so wish.
Data Collection – First the schools will be informed of the purpose of the study. A school day will be used at each school setting, which is between Monday and Friday. 12 data collectors will be trained for one week on the purpose of the study, questionnaire administration, and conduct of FGD. The research assistant are going to be Community Health Nurses (CHNs) with at least two years post training. When assured of a complete understanding and mastery of the tools, then the study proper will start at the selected schools. The research assistants who will be recruited for the study will qualified circuit community health nurses with at least four years post training work experience. The community health nurse cadre is the second level nurses in the Gambia. They have two years extensive training on nursing procedures. The reason of recruiting this cadre is that they are very good in collecting very sensitive community information.
At least a day will be spent at each school, where semi-structured questionnaires will be administered to the subjects, and two FGDs conducted. The questionnaires will be on knowledge, attitude and practice on family planning.
Data Management – since the data will be mostly coded, all will be entered after checking for errors. Ten percent of randomly selected data will be validated by double entry. The data will be kept in a locked safe and individual students will not be traced by names, because they can only be identified by codes known to the research team only.
3.10 DATA PROCESSING AND ANALYSIS
Data processing and analysis will be done using the Statistical Package for Social Sciences (SPSS) Version 20.0 for windows program. Descriptive statistics such as frequencies, percentage, and appropriate graphic presentation besides measures of central tendency and measures of dispersion will be used for Univariate analysis. Bivariate analysis will be used to analyze some of the variables.
The FGD data will be transcript and analyze using theme.
3.11 ETHICAL CONSIDERATIONS
This study will be subjected to the approval of the Ethics Review Board of University of Benin & University of Benin Teaching Hospital. Approval will also be sought from the Joint Gambia Government –MRC Ethics Committee in The Gambia. The study targets are secondary school students so their assent as well as their school principals’ consent will be sought with adequate information, after securing the approval of the Ministry of Basic and Secondary Education (MoBSE).
3.12 DISCUSSION
This study will compare the knowledge, attitude and practice on family planning among secondary school students in Region II&IV Education Directorates. Even though a cross-sectional study cannot confer causality, it is the design of choice here because it is quick, economical, and the study is a prevalence study that does not require follow up.
3.13 STRENGTH AND LIMITATION
Strength of the study is its large sample size and it is including students of many schools.
Due to the sensitivity of the study subject, some study participants may feel ashamed to raise their hands when they need clarifications. This can cause them not to fill all parts of the questionnaire. Therefore to reduce nonresponse rate an additional 10% will be increased on the sample size. This may limit the generalization of the findings.
The other strength of the study is the use of FGD. FGD will be used to validate the data collection using the questionnaire.
STUDY TIMELINE
The study hopes to take this long to be accomplished. See Table below for summary of the study timeline.
|
Task |
2016 | 2017 | |||||
| November | December | January | February | March | April | May | |
| Obtain ethics approval | |||||||
| Obtain Funding | |||||||
| Data Collection Tools | |||||||
| Recruit & training of data collectors | |||||||
| Pilot study, test tools | |||||||
| Travel to study site to work on sampling | |||||||
| Select study participants | |||||||
| Data collection | |||||||
| Data cleaning & entering | |||||||
| Data analysis & write up | |||||||
| Publish Findings | |||||||
BUDGET
| Budget line | Description | Quantity /days | Unit cost (GMD) | GMD | USD Estimate |
| Human resources | Coordinator | 20 | 350 | 7000 | 175.00 |
| 5 Research Assistants | 20 | 250 | 25000 | 625.00 | |
| Students | 846 | 15 | 12,690 | 317.25 | |
| Sub Total | 44,690 | 1117.25 | |||
| Transport | Travel to Gambia | 1 | 27,200 | 27,200 | 680 |
| Petrol | 20 | 750 | 15,000 | 375 | |
| Sub-Total | 42,200 | 1055.00 | |||
| Administration Printing & photocopying | |||||
| Questionnaire | 7 | 850 | 5,950 | 148.75 | |
| Consent form | 2 | 850 | 1,700 | 42.50 | |
| Assent Form | 1 | 850 | 850 | 21.25 | |
| Stationary | 4 packs | 750 | 3000 | 75 | |
| Final report Production | 10 copies | 650 | 6,500 | 162.50 | |
| Lockable Safe | 1 | 2500 | 2,500 | 62.50 | |
| Sub Total | 20,500 | 512.50 | |||
| Utilities | Phone Minutes | – | 1500 | 1,500 | 37.50 |
| Internet Connectivity | – | 1000 | 1,000 | 25.00 | |
| Sub Total | 2,500 | 62.50 | |||
| Miscellaneous | – | 2000 | 2000 | 50.00 | |
|
Grand Total |
111,890 |
2,797.25 |
|||
| Budget Summary | |||||
| Human Resources | 44,690 | 1117.25 | |||
| Transport | 42,200 | 1055.00 | |||
| Administration | 20,500 | 512.50 | |||
| Utilities | 2500 | 62.50 | |||
| Miscellaneous | 2000 | 50.00 | |||
|
Total |
111,890 |
2,797.25 |
|||
BUDGET NARRATION
Human Resources
Coordination: A coordinator is needed to facilitate the smooth running of the study, to link up with the schools, distribute the correspondence, the consent and assent forms prior to the start of the study. The coordinator will ensure the acquisition and printing of data collection tools and needed stationery. This coordinator is also responsible for securing the training ground, training the data collectors, and translation of tools into local languages for the understanding of the data collectors.
Data Collectors: 5 data collectors will administer the questionnaires, and conduct the FGDs.
The students will, in the end receive exercise books as tokens of appreciation for participation as study subjects.
Transport – transportation is relevant in the form of car rental and fuel for mobility of the research personnel and data collection tools to and from study sites for the duration of the study.
Administration – is another crucial component that includes the research tools, stationery for data collection, training, and pilot testing, as well as locks for safe keeping of all items. It also includes the cost of the production of the final report at the end of the study.
Utilities – mostly for communication (phone minutes and internet connection). This will be needed for communication between the researcher and supervisor(s) in Nigeria, as well as between the researcher and data collectors while in the field. Communication will bridge the gap and help sort things out and matters arising during the study period. It will also improve the ability to contact appropriate officials in the Ministry of Basic and Secondary Education of The Gambia, when necessary.
Miscellaneous – as the name implies is for standby in case of any unforeseen expenses during the study period.
Total – the final estimate of the budget after a sum of all the above is GMD 111,890, which is approximately USD 2,797.25. The exchange rate is the Dollar to the Dalasi is D40.00.
Appendix 1
PARTICIPANT INFORMATION SHEET
| Date |
Study Title: KNOWLEDGE, ATTITUDE AND PRACTICE ON FAMILY PLANNING AMONG SECONDARY SCHOOL STUDENTS IN THE GAMBIA: A COMPARATIVE STUDY
What is informed consent?
You are invited to take part in a research study. Before you decide you need to understand why the research study is being done and what it will involve. Please take time to read the following information or get the information explained to you in your language. Listen carefully and feel free to ask if there is anything that is not clear or you do not understand. You may also wish to consult your class teacher or principal before deciding to take part in the study.
If you decide to join the study, you will need to sign on a consent form saying you agree to be in the study.
What harm or discomfort can you expect in the study?
No invasive experiments will be used during the study. The entire study process will be discussed with the participants and emphasis will be made that there are no penalties for refusing to participate or withdraw from the study.
What benefits can you expect in the study?
There is no direct individual benefit to you. The study finding will become the bases for the design and implementation of an intervention. It will also help policy makers to make rightful decisions in the provision of qualitative Family Planning Services to students.
Will you be compensated for your child’s/ward’s participation in the study?
You will not get paid for participation of your child in the study, but you will get either transport by MRC or get the costs for the transport reimbursed.
What happens if you refuse to participate in the study or change your mind later?
You are free to participate or not in the study and you have the right to stop participating at any time without giving a reason.
In case you decide to withdraw your participation during the study I will not work on your questionnaire.
Should any new information become available during the study that may affect your participation, you will be informed as soon as possible.
How will your information be kept and who will be allowed to see it?
All information that is collected about you in the course of the study will be kept strictly confidential. Your personal information will only be available to the Principal Investigator and might be seen by some rightful persons from the Ethics Committees, Government authorities and sponsor.
Who should you contact if you have questions?
Please feel free to ask any question you might have about the research study.
Who has reviewed this study?
This study has been reviewed and approved by a panel of scientists at the University of Benin/UBTH and the Gambia Government/MRC Joint Ethics Committee, which consists of scientists and lay persons to protect your rights and wellbeing.
Appendix 2
Consent / Assent Form
Participant’s Name
Participant’s Identification Number: |__|__|__|__|__|__|__|__|__|__|
OR
(Printed name of class teacher) (Printed name of school principal)
I have read the written information OR
I have had the information explained to me by study personnel in a language that I understand, and I
- confirm that my choice to participate is entirely voluntarily,
- confirm that I have had the opportunity to ask questions about this study and I am satisfied with the answers and explanations that have been provided,
- understand that I grant access to data about me to authorised persons described in the information sheet,
- have received time to consider to take part in this study,
- agree to take part in this study.
Tick as appropriate
| I agree to further research on my questionnaire as described in the information sheet | Yes | No | ||||
| Participant’s signature for assent
(child aged 12-17 years) |
||||||
| Date (dd/mmm/yyyy) Time (24hr) | ||||||
| Participant’s principal/teacher signature | ||||||
| Date (dd/mmm/yyyy) Time (24hr) | ||||||
| Printed name of witness* | ||||||
| Printed Name of Person obtaining consent | ||||||
|
I attest that I have explained the study information accurately in _____________ to, and was understood to the best of my knowledge by, the participant/teacher/principal. He/she has freely given consent to participate *in the presence of the above named witness (where applicable). |
||||||
| Signature of Person obtaining consent | ||||||
| Date (dd/mmm/yyyy) Time (24hr) | ||||||
Appendix 3
QUESTIONNAIRE
Hello my name is —–, a student from the University of Benin, Nigeria working towards a Master Program in Reproductive and Family Health. The thesis is on KNOWLEDGE, ATTITUDE AND PRACTICE ON FAMILY PLANNING AMONG SECONDARY SCHOOL STUDENTS IN THE GAMBI: A COMPARATIVE STUDY and you are selected for this purpose. You are free to answer the questions listed below. Your identity will be kept confidential and will not be revealed to anyone. I am seeking your consent to participate in this study.
School ID: ………………………………… Date: ………………
Demographic Information
1. Gender [ ] Male [ ] Female
2. How old are you?………………
3. What grade are you? [ ] 12 [ ] 11 [ ] 10 [ ] 9 [ ] 8 [ ] 7
4. What is your religion? [ ] Islam [ ] Christian [ ] Africa Traditional Religion [ ] others specify ……………
5. What is your parents’ educational level?
| Option | Father | Mother | Guardian |
| No education | |||
| Primary | |||
| Secondary | |||
| Tertiary |
6. What is your parents’ occupation?
| Option | Father | Mother | Guardian |
| Farmer/gardener | |||
| Civil Servant | |||
| Business | |||
| Others (specify) |
7. Which of the following do you have at home?
[ ] TV [ ] Radio [ ] Smartphone [ ] Newspaper [ ] others (specify)
KNOWLEDGE
8. Do you have any Knowledge about family planning?
[ ] yes [ ] no [ ] I do know
9. Do you have access to family planning service?
[ ] yes [ ] no
10. What is your source of information on family planning?
[ ] Radio/TV [ ] Parents [ ] boy/girlfriend [ ] friends [ ] others (specify)
11. About which family planning method you have knowledge have more knowledge?
[ ] Oral Pills [ ] withdrawal [ ] IUD [ ] Condom (male and female) [ ] Injection [ ] others
12. What about other types of family planning, how much do you know about them?
————————————————————————————————————————————————————————————————————————
ATTITUDE
13. What is your attitude towards family planning?
[ ] favorable [ ] unfavorable [ ] I don’t know
14. Do you have any contact at the health center who helps you with family planning services?
[ ] yes [ ] no
15. Is your boy/girlfriend in favor of family planning?
[] yes [ ] no
16. If you want family planning services where do you go?
[ ] health center [ ] pharmacy [ ] my friend [ ] others
17. Have you ever experienced any problem in getting family planning commodities?
[ ] yes [ ] no
18. If yes, what was the problem?
[ ] Finance [ ] Age related [ ] Distance [ ] Others please specify ……………………………
PRACTICE
19. Do you practice family planning?
[ ] yes [ ] no
20. If yes, is it your own option?
[ ] yes [] no
21. If no, who advised you?
[ ] parents [ ] boy/girlfriend [ ] friend
22. What are the reasons from adopting a family planning method?
[ ] fear of being pregnant [ ] protection from STI [ ] was advised [ ] others please specify ………………………………………………………………………………………………
23. What is your source of information?
[ ] TV [ ] Radio [ ] Smartphone [ ] Newspaper [ ] others (specify)
24. If you don’t use any family planning method, what are the reason?
[ ] religious beliefs [ ] fear of side effects [ ] pressure from my boy/girlfriend
25. Are you currently using any family planning?
[ ] yes [ ] no
26. If yes, which method?
[ ] Oral Pills [ ] withdrawal [ ] IUD [ ] Condom (male and female) [ ] Injection [] others
27. Have you experienced side effects of family planning method after its application?
[ ] yes [ ] no
28. If yes, explain what happened. ………………………………………………………..
29. Have you ever had sexual intercourse?
[ ] Yes [ ] No
30. What age did you experience your first sexual intercourse? ………………………………
31. What was the reason for the sexual encounter? ………………………………………….
32. What was your relationship with the person with who you had sex with?
[ ] boy/girlfriend [ ] classmate/club mate [ ] teacher [ ] visitor [ ] others
33. In the event you do not have a condom, do you continue to have sex?
[ ] yes [ ] no
34. Have many sex partners do you have?
………………………………………………………………………………………………
FOCUS GROUP DISCUSSION CHECKLIST
- What is your understanding of family planning?
- What family planning method(s) do you know?
- What are the advantages and disadvantages of family planning?
- Does any of your friends use family planning?
- Do you think students have access to family planning services?
- What are the barriers that prevent students from utilizing family planning services?
Dear Sir/Madam,
KNOWLEDGE, ATTITUDE AND PRACTICE ON FAMILY PLANNING AMONG URBAN AND RURAL SECONDARY SCHOOL STUDENTS IN THE GAMBIA: A COMPARATIVE STUDY
I write to submit the above research proposal for ethical review by the Joint Gambia Government / MRC Ethics Committee. Attached are the following documents:
- A signed copy of my application form and the proposal
- The approval from the Research Ethics Committee of University of Benin
- A letter from the University Benin Teaching Hospital Health Research Committee, which has reviewed the study.
- Budget details – appendix 8
- Other Appendices
- Letters of support and permission, subject to approval
- Letter of consent
- Research questionnaire
Yours sincerely,
…………………………………..
Dear Sir,
PERMISSION TO CONDUCT THESIS RESEARCH IN SECONDARY SCHOOLS IN REGIONS II AND IV
I am a Gambian doing Master of Public Health in Reproductive and Family Health at the college of medical sciences, University of Benin, Nigeria. The research I wish to conduct for my Master’s thesis is on the ‘Knowledge Attitude and Practice on Family Planning among urban and Rural Secondary Schools in the Gambia: A comparative Study’. This research will be supervised by the University of Benin, Nigeria.
Attached is a copy of the proposal which includes copies of the questionnaire and consent form for the study and also a copy of the approval letter which I received from the University of Benin Teaching Hospital Research Ethics Committee.
Upon completion of the study, the Ministry of Basic & Secondary Education will be provided with a bound copy of the full research report.
In this end, I write seeking your permission to approach some secondary schools in Regions II&IV to serve as participants for my research.
Yours sincerely,
Dear Mr/Ms/Mrs _____________,
PERMISSION TO CONDUCT THESIS RESEARCH IN YOUR SCHOOL
I am a Gambian doing Master of Public Health in Reproductive and Family Health at the college of medical sciences, University of Benin, Nigeria. The research I wish to conduct for my Master’s thesis is on the ‘Knowledge Attitude and Practice on Family Planning among urban and Rural Secondary Schools in the Gambia: A comparative Study’. This research will be supervised by the University of Benin, Nigeria.
Attached is a copy of the proposal which includes copies of the questionnaire and consent form for the study and also a copy of the approval letter which I received from the University of Benin Teaching Hospital Research Ethics Committee.
Upon completion of the study, your administration will be provided with a bound copy of the full research report.
In this end, I write seeking your permission to use of your students to serve as participants for my research.
Yours sincerely,
REFERENCES
1. WHO | Family planning. WHO. 2016;
2. WHO | Contraception: past, present and future and why it matters. WHO. 2016;
3. Universal Access to Reproductive Health PROGRESS AND CHALLENGES. 2016;
4. WHO | Adolescent health. [cited 2016 May 26]; Available from: http://www.who.int/topics/adolescent_health/en/
5. WPRO | Fact sheet on adolescent health. [cited 2016 May 26]; Available from: http://www.wpro.who.int/mediacentre/factsheets/docs/fs_201202_adolescent_health/en/
6. Status Report: Adolescents and Young People in Sub-Saharan Africa, Opportunities and Challenges – status-report-youth-subsaharan-Africa.pdf. [cited 2016 May 26]; Available from: http://www.prb.org/pdf12/status-report-youth-subsaharan-Africa.pdf
7. EUROPEAN ACADEMIC RESEARCH, VOL – 1754.pdf [Internet]. [cited 2016 May 26]. Available from: http://euacademic.org/UploadArticle/1754.pdf
8. WHO | Adolescent pregnancy. WHO. 2016;
9. ADOLESCENT PREGNANCY : A Review of the Evidence ADOLESCENT PREGNANCY : A Review of the Evidence.
10. Unplanned-Pregnancy-Among-Unmarried-Adolescents-In-Urban-Gambia.pdf [Internet]. [cited 2016 May 26]. Available from: https://www.duo.uio.no/bitstream/handle/10852/45401/Unplanned-Pregnancy-Among-Unmarried-Adolescents-In-Urban-Gambia.pdf?sequence=1&isAllowed=y
11. SEXUAL REPRODUCTIVE HEALTH AND RIGHTS FOR ADOLESCENTS IN. :1–10.
12. Survey H. The Gambia. 2013;
13. UNFPA and Adolescents [Internet]. [cited 2016 May 27]. Available from: http://web.unfpa.org/public/cache/offonce/home/sitemap/icpd/International-Conference-on-Population-and-Development/unfpa_and_adolescents
14. Ganchimeg T, Ota E, Morisaki N, Laopaiboon M, Lumbiganon P, Zhang J, et al. Pregnancy and childbirth outcomes among adolescent mothers: a World Health Organization multicountry study. BJOG. 2014;121 Suppl:40–8.
15. WHO | Family planning/Contraception. WHO. 2016;
16. Gottschalk LB, Ortayli N. Interventions to improve adolescents’ contraceptive behaviors in low- and middle-income countries: A review of the evidence base. Contraception [Internet]. 2014;90(3):211–25. Available from: http://dx.doi.org/10.1016/j.contraception.2014.04.017
17. Nova Scotia Gambia Association Survey of knowledge and attitudes of students towards sexual and reproductive health , environmental , leadership and gender issues in The Gambia Final Report. 2009;(February):1–63.
18. Chaaban J, Cunningham W. Measuring the Economic Gain of Investing in Girls: The Girl Effect Dividend [Internet]. The World Bank; 2011 [cited 2016 Oct 19]. (Policy Research Working Papers). Available from: http://elibrary.worldbank.org/doi/book/10.1596/1813-9450-5753
19. The Gambia Demographic and Health Survey. 2013;
20. Anderson K, Strutt A, Caldeirinha V, Felício JA, Dionísio A, Environment NM, et al. New Microsoft Office Word Document [Internet]. Vol. 8, Smh. 2015. p. 2229–32. Available from: http://www.smh.com.au/world/philippines-and-china-clash-as-tensions-rise-over-oilrich-seas-20120411-1ws5q.html#ixzz2246vAQlQ http://www.sciencedirect.com/science/article/pii/S0742051X07000066 http://www.ncbi.nlm.nih.gov/pubmed/20431354 http://pubs.scie
21. Khan K. Unplanned pregnancy among unmarried adolescents in Urban Gambia. 2015;(May):1–119. Available from: http://docplayer.net/19344194-Unplanned-pregnancy-among-unmarried-adolescents-in-urban-gambia-kumba-khan.html#download_tab_content
22. Ministry of Health. Teenage pregnancy in Gambia: still too stubborn to ignore – The Torch [Internet]. 2015. Available from: https://torchongambia.wordpress.com/2015/09/29/teenage-pregnancy-in-gambia-still-too-stubborn-to-ignore/
23. Health Belief Model [Internet]. Available from: https://www.utwente.nl/cw/theorieenoverzicht/Theory Clusters/Health Communication/Health_Belief_Model/
24. B UD. Socio-Economic Status, Contraceptive Knowledge And Use Among Rural Women In Ikeji Arakeji, Osun State, Nigeria Background/Statement of the Problem. Afro Asian J Soc Sci. 2012;3(32).
25. WHO | Family planning in sub-Saharan Africa: progress or stagnation? WHO. 2011;
26. Of N. Knowledge and ever use of family planning 5.1. 2003;53–65.
27. Dangat CM, Njau B. Knowledge , attitude and practices on family planning services among adolescents in secondary schools in Hai District , northern Tanzania. 2013;15(1):1–8.
28. McDevitt MT, Adlakha A, Fowler BT, Al. E. Trends in adolescent fertility and contraceptive use in the developing world. United States Bur Census, Rep IPC. 1996;95(1):44–58.
29. Malleshappa K, Krishna S, Nandini C. Knowledge and attitude about reproductive health among rural adoles-cent girls in Kuppam mandal: An intervention study. Biomed Res. 2011;22(3):305–10.
30. Dudas R, Serwint JR. In Brief. Pediatr Rev [Internet]. 2006;27(6):45–6. Available from: http://www.guttmacher.org/pubs/FB-Adolescents-SRH.pdf
31. Planning and Reasons for Nonuse among Women with Unmet Need for Family Planning in Ethiopia.
32. Eltomy EM, Saboula NE, Hussein a a. Barriers affecting utilization of family planning services among rural Egyptian women. East Mediterr Health J [Internet]. 2013;19(5):400–8. Available from: http://www.ncbi.nlm.nih.gov/pubmed/24617117
33. Najafi-sharjabad F, Zainiyah S, Yahya S, Rahman HA, Hanafiah M. Barriers of Modern Contraceptive Practices among Asian Women : A Mini Literature Review. 2013;5(5):181–92.
34. Sreytouch V. Knowledge, Attitude and Practice (KAP) of Family Planning among Married Women in Banteay Meanchey, Cambodia.
35. Report C, Omishakin MYJ. Women ’ s Health & Gynecology Knowledge , Attitude and Practice of Family Planning among Healthcare Providers in Two Selected Health Centres in Osogbo Local Government , Osun State. 2015;1(2):2–5.
36. Sajid A, Malik S. Knowledge, Attitude and Practice of Contraception Among Multiparous Women at Lady Aitchison Hospital, Lahore. Ann Vol Oct – Dec. 2010;16(4):2008–11.
37. Gupta V, Mohapatra D, Kumar V. Family planning knowledge, attitude, and practices among the currently married women (aged 15-45 years) in an urban area of Rohtak district, Haryana. Int J Med Sci Public Heal [Internet]. 2015;5(4):1. Available from: http://www.scopemed.org/?mno=199530
38. Hoque ME, Ntsipe T. Journal of Social Aspects of HIV / AIDS Awareness and practices of contraceptive use among university students in Botswana. J Soc Asp HIV/AIDS [Internet]. 2016;0(0):1–6. Available from: http://dx.doi.org/10.1080/17290376.2013.869649
39. Laura B Motta Martins, a, Lúcia Costa-Paiva, b, Maria José D Osis, c, et al. Knowledge of contraceptive methods among adolescent students. Rev Saúde Pública [Internet]. 2006 [cited 2016 Oct 25];40(1). Available from: www.fsp.usp.br/rsp
40. Eniojukan Joshua F. Knowledge, Perception and Practice of Contraception among Staff and Students in a University Community in Delta State, Nigeria. UK J Pharm Biosci [Internet]. 2016 Feb 1 [cited 2016 Oct 25];4(1). Available from: http://www.ukjpb.com/pdf/UKJPB_SuperAdmin_1_168_1450418607.pdf
41. Ugoji FN. An Examination of University Students ’ Attitude to Contraceptive Use. 2013;2(1):18–22.
42. Liu Z, Zhu M, Dib HH, Li Z, Shi S, Wang Z. RH knowledge and service utilization among unmarried rural-to-urban migrants in three major cities , China. 2011;
43. Stephenson, R., & Hennink M. Barriers to family planning services amongst the urban poor in pakistan – ePrints Soton. Eprints.soton.ac.uk [Internet]. 2004; Available from: http://eprints.soton.ac.uk/34728/
44. Amentie, Muluwas , Abera M, Abdulahi M. Utilization of Family Planning Services and Influen cing Factors Among Women of Child Bearing Age in Assosa District, Benishangul Gumuz Regional State, West Et hiopia. Sci J Clin Med [Internet]. Vol. 4, No:52–59. Available from: http://article.sciencepublishinggroup.com/pdf/10.11648.j.sjcm.20150403.11.pdf
45. 2525.pdf.
46. Enuameh Y, Tawiah C, Afari-Asiedu S, Nettey OEA, Sulemana A, Mahama E, et al. Making Family Planning Services Relevant to Adolescents: Perspectives from Rural Communities in Central Ghana. Open J Prev Med [Internet]. 2014 [cited 2016 Oct 17];4(11):852–9. Available from: http://www.scirp.org/journal/PaperDownload.aspx?DOI=10.4236/ojpm.2014.411096
47. Access O. Factors influencing the uptake of family planning services in the Talensi District, Ghana. 2015;8688:1–9.
48. Ministry G, Education S, National G. Gambia Education for All 2015 National Review The Gambia National Education For All Review Report Prepared by : 2015;
49. REPUBLIC OF THE GAMBIA DEPARTMENT OF STATE FOR HEALTH NATIONAL REPRODUCTIVE HEALTH POLICY REPUBLIC OF THE GAMBIA NATIONAL REPRODUCTIVE HEALTH POLICY 2007 – 2014 Table of Contents. 2014;
50. Statistics E. 2014/2015. 2015;(May).
51. Khan ME, Anker M, Patel BC, Barge S, Sadhwani H, Kohle R. The use of focus groups in social and behavioural research: some methodological issues. World Health Stat Q [Internet]. 1991 [cited 2016 Oct 12];44(3):145–9. Available from: http://www.ncbi.nlm.nih.gov/pubmed/1949882
52. Williams A, Katz L. The Use of Focus Group Methodology in Education: Some Theoretical and Practical Considerations, 5(3).
53. Burns KEA, Duffett M, Kho ME, Meade MO, Adhikari NKJ, Sinuff T, et al. A guide for the design and conduct of self-administered surveys of clinicians. CMAJ [Internet]. 2008 Jul 29 [cited 2016 Oct 12];179(3):245–52. Available from: http://www.ncbi.nlm.nih.gov/pubmed/18663204
Cite This Work
To export a reference to this article please select a referencing stye below:
Related Services
View all


Related Content
All TagsContent relating to: "Health"
Health is the general condition of the body or mind. The World Health Organization defines health as “a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity.”
Related Articles

DMCA / Removal Request
If you are the original writer of this dissertation proposal and no longer wish to have your work published on the UKDiss.com website then please: