CaHA as a Biostimulatory Agent
Info: 8270 words (33 pages) Dissertation
Published: 17th Dec 2019
Tagged: Biosciences
CONSENSUS RECOMMENDATIONS FOR THE USE OF HYPERDILUTED CALCIUM HYDROXYAPATITE (RADIESSE®) AS A FACE AND BODY BIOSTIMULATORY AGENT
BACKGROUND: Calcium hydroxyapatite (CaHA) is a well stablished collagen stimulator. In the recent past years it has been increasingly used in a hyperdiluted way as a biostimulatory agent, rather than a volumizer filler to improve skin quality and firmness both in facial as well as in corporal areas. However, guidelines on the techniques required to achieve optimal results are still lacking.
OBJECTIVE: To develop consensus recommendations for the safe and effective use of hyperdiluted CaHA for face and body biostimulation.
METHODS: A team of ten experts with extensive experience in dermal fillers and biostimulatory treatments for facial and body rejuvenation convened for a live meeting. Consensus was defined as approval by 70% to 89% of all participants, whereas agreement of 90% denoted a strong consensus.
RESULTS: For most items, the group achieved a majority consensus. Recommendations have been provided for the face, neck, décolletage, buttocks, thighs, arms, abdomen, knees and elbows, providing detailed injection techniques, including information on insertion points, dosage and volume for both needle and cannula injections as well as number of treatment sessions and intervals.
CONCLUSION: Experts consensus support and provides a guidance for the use of CaHA as a biostimulatory agent for face and body rejuvenation. However further clinical studies are necessary to provide physicians with the best evidence for the best treatment practices.
Nowadays there is a growing demand for rejuvenation methods for nonfacial areas following the successful noninvasive boom of aesthetic procedures in the face. Among these procedures, are the use of energy-based, like microfocused ultrasound, radiofrequency and lasers devices, as well as the injection of microparticles capable of induce tissue remodelling and improvement of skin quality, smoothness and firmness. Radiesse® (Merz Pharmaceuticals) is a biocompatible, biodegradable, resorbable and biostimulatory filler that contains CaHA microspheres which can stimulate the endogenous production of collagen. It is a unique product that provides both volume replacement and collagen biostimulation as a primary mechanism of action.1 The product has a similar texture to human tissue and migration is minimal. Initial augmentation is afforded by the presence of the carrier carboximetylcelulosis (CMC) gel with the implant itself, but around 9 to 12 months the CaHA particles are degraded as calcium and phosphate and eliminated through the renal system.2-5 Highly viscoelastic, CaHA is well suited for supraperiosteal, subdermal, and deep dermal placement but, when diluted, may also be injected more superficially for dermal rejuvenation.1,2When used undiluted, or with small dilutions, treatment provides immediate correction that is gradually followed by new tissue formation through neocollagenesis, elastin production, dermal cell proliferation, and angiogenesis. The result is a long-lasting aesthetic improvement of 18 months or longer with tight and elastic skin, and increased skin thickness.5,6 Radiesse® received a Conformité Européenne (CE) certification mark (medical device class 3) for plastic and reconstructive surgery, including deep dermal and subdermal soft tissue augmentation of the facial area in 2003.1 In 2006, Radiesse® received FDA approval for the correction of moderate-to-severe facial wrinkles and folds, such as nasolabial folds, and/or the correction of the signs of facial fat loss in people with human immunodeficiency virus1 and in 2015 Radiesse® received FDA approval for extra-facial treatment of the hands.
When used in a hyperdiluted fashion (i.e:1,5cc of product plus 1,5cc or more of diluent) Radiesse® has minimal or absent immediate volumizing effect due to the CMC gel dispersion, generating only the long-term tissue remodeling by the CaHA microspheres.
This article presents consensus recommendations for hyperdiluted application of calcium hydroxylapatite (Radiesse®) in the face as well as in nonfacial areas, providing detailed injection techniques, including information on insertion points, dosage and volume for injections and also required treatment sessions and intervals between them.
Methods
A team of ten experts in the fields of Dermatology and Plastic Surgery with extensive experience in dermal fillers for facial and body rejuvenation, convened in November 2017 for a full-day meeting in São Paulo, Brazil. A questionnaire distributed before the meeting and answered by the experts, served as the basis for the knowledge of medical management with this product and subsequent discussion. The meeting followed a structured consensus approach by an experienced moderator.
Consensus was defined as approval from 70% to 89% of all participants, whereas agreement of 90% denoted a strong consensus.
Recommendations and suggestions had focus in providing directions for hyperdiluted use of CaHA for face, neck, décolletage, buttocks, thighs, arm, abdomen, knee and elbow providing detailed injection techniques, including information on insertion points, dosage and volume for both needle and cannula. It is our hope that this article will aid physicians in making decisions about the best practice for skin rejuvenation with this biostimulatory filler.
CaHA as a Biostimulatory Agent
Since 2004 evidence exists that the long lasting effect of calcium hydroxyapatite is secondary to a controlled inflammatory process that generates a predominantly fibroblastic reaction with replacement of the aqueous gel by dense deposit of collagen.7 Berlin and coworkers3 observed that the main deposit is given by type 1 collagen, associated to the improvement of the mechanical properties of the skin, rather than type III collagen, which may be associated with fibrotic processes. It was also observed that CaHA produced more type 1 collagen, elastin and generated a greater proliferation of fibroblasts after 7 months when compared to hyaluronic acid.8 Couderot and coworkers9 noticed that in addition to fibroblasts proliferation, CaHA also improved its contractile function, which is important for the product’s tightening effect. Another study10 using CaHA diluted 1:1, found that, when associated to MFU (microfocused ultrasound), there was larger production of type 1 collagen after just one single session. One subject scheduled for thighplasty received treatment with 6 different CaHA dilutions followed by MFU with visualization (MFU-V). Tissue specimens from each dilution site were examined under polarized light microscopy to assess neocollagenesis. At 90 days, histologic analysis showed peak neocollagenesis in samples treated with the 1:1 dilution, whether with CaHA alone or in combination with MFU-V. Yutskovskaya and Kogan6 observed that even when used in large dilutions (1:2 – 1:6), Radiesse® was effective in increasing the production of type 1 collagen and elastin, 7 months later, as well to improve neck and décolletage laxity after 2 sessions, with a 4-months interval. Subjects also received same dilution deep subdermal injection of CaHA (~0.1 mL) in the peri-auricular area for skin biopsies. Tissue samples were obtained at baseline, after 4 and 7 months for immunohistochemical evaluation of neocollagenesis. Immunohistochemical analysis of collected tissue demonstrated significant increases in type 1 collagen expression at 4 (P<0.05) and 7 months (P<0.00001) compared with baseline. Staining for elastin and angiogenesis significantly increased at 4 (P<0.05 and P<0.01, respectively) and 7 months (P<0.00001 for both) compared with baseline. Clinically, Silvers and coworkers5 demonstrated an increase in skin thickness by 50% after 3 months of application, which was maintained for the 12 months evaluation period. Pavicic11 observed soft tissue enlargement at MRI (magnetic resonance imaging) examination, even after complete absorption of CaHA particles. Wasylkowski12 reported the improvement of laxity and dermal thickness in the treatment of abdominal region, arms and thighs. Also in 2015, Amselem13 observed improvement of arms laxity after 2 treatment sessions spaced monthly. To conclude, in 2016 two consensus on combination of procedures for face and body suggested the use of hyperdiluted CaHA (1:1 or 1:2) for dermal rejuvenation in large areas.2,14
Anesthesia and Dilutions
Pain management is an important issue to consider during aesthetic procedures. Pain is a subjective experience, and each individual’s need for pain relief should be assessed.15 In 2009, the FDA approved a protocol for mixing CaHA with lidocaine on a concentration of 0,3% to improve patient comfort during injection. Diluted CaHA has become widely used by injectors as it expands the range of indications for which CaHA can be used. Many experts developed techniques for using the higher diluted CaHA taking advantage of its collagen-stimulating effects to reduce skin laxity, but without the volumizing effect.6Some injectors use lidocaine for the initial dilution to reduce discomfort with further dilutions achieved by the addition of normal saline. Others prefer the use exclusive of preserved saline, which itself has local anesthetic properties. Dilutions can be titrated depending on the thickness of patient’s skin and the degree of tissue laxity to ensure smooth product placement.6
Needle or Cannula
Dermal fillers may be injected using either needles or blunt-tip microcannulas. Needles have the advantages of extreme movement precision, possibility of intradermal injection, and requirement of smaller injection volumes. Disadvantages include pain, bruising, and the possibility of nerve/vessel injury. Cannulas cause less trauma, pain, and bruising and allow treatment of large areas at the chosen injection depth. Van Loghem and coworkers16 compared in cadaver specimens, the precision difference between supraperiosteal filler placement using a sharp needle and a non-traumatic cannula. The latter resulted in product being confined to the deep anatomic layers. In contrast, with the sharp needle technique, material was placed in multiple anatomic levels, from the periosteum to more superficial skin layers. The authors concluded that cannula showed more accuracy in product placement. The sharp needle technique also showed a higher complication risk of intra-arterial injection occurrence, even though the needle tip was positioned on the periosteum and the product was injected with the needle in constant contact with the periosteum. In another recent study,17 ten fresh-frozen cephalic foreheads (9 male and 1 female) were injected with radiopaque material using both needles and cannulas. Additional computed tomography and magnetic resonance imaging were performed to confirm results. In 60% of injections using a needle, the implanted material changed its plane; this was not observed when using the cannula (0%; P=0.003). Therefore, using cannulas resulted in a more precise placement of the injected material as compared to needles. The authors of the consensus considered the possibility of use of blunt cannula or sharp needle, keeping in mind that with the use of needle, there is a greater risk of superficial placement of the product and therefore this procedure must be carried out very carefully.
General Consensus Statements on Aims of Treatment with CaHA According to consensus members, the following general guidelines for treatment with hyperdiluted CaHA were established. These statements reached strong consensus (agreement of 90% or more) by the expert group members (TABLE 1).
- For CaHA biostimulation/skin tightening, 2 to 3 sessions are usually recommended spaced at 1-2 months intervals.
- The preferred CaHA dilution for biostimulation/skin tightening treatment may change according to the treated area, degree of laxity and skin thickness.
- The higher the dilution used, the lower the immediate volumizing effect.
- It is possible that when used more diluted CaHA distributed into large areas further treatment sessions will be required.
- It is possible that higher dilutions imply in a lower risk of nodule formation due to product accumulation.
- The literature shows that CaHA acts as a collagen and elastin biostimulator when used undiluted or diluted up to 1:6 (9 mL of diluent to 1.5 mL of product). However, the existing data are insufficient to certify that one dilution is superior to the other in the final collagen stimulus.
- The size relation between area to be treated and product amount may vary according to local tissue, anatomical peculiarity and local degree of laxity. Usually 1 syringe (1.5 mL) is used to treat an area of 100 to 300 cm2.
- For dilution of CaHA, 0.5 to 1.5 mL of 1% lidocaine with or without epinephrine may be used. If larger dilutions are needed, then saline solution is added to complete the desired final volume.
- The recommended cannulas are usually 22 to 25 gauge.
- The recommended needles are usually 27 to 30 gauge.
TABLE 1: General Consensus Statements.
Face
Soft tissue fillers offer a versatile, nonsurgical option for facial augmentation and contouring with a multitude of potential aesthetic applications.18 The face is prone to early manifestations of aging, due to intrinsic factors and specially the higher exposition to extrinsic factors, compared to other body areas. Degenerative changes occur in nearly every anatomic component of the face.19 Volume loss and displacement of facial fat pads associated with laxity of ligaments cause skin drooping over a changing bony skeleton.20 The skin aging is related to an increased activity of endogenous enzymes (i.e: metaloproteinases), among other factors, that rise the breakdown of collagen and elastin fibers, turning the skin prone to wrinkling and sagging and highlighting the changes of the deeper structures. With time, the heart-shaped face of youth becomes distinctly pear shaped with a sunken midface, a lower face becoming more squared than oval and a deepening of lines and folds.21,22 The classic use of CaHA was considered very effective for restoring volume loss of midface, filling of nasolabial folds and improving jawline contour in routine practice and was associated with high levels of physician and patient satisfaction as shown in the literature. Adverse events were mostly mild and related to either the procedure or injection technique.23,24 The properties of Radiesse® provide it with great versatility and make it suitable for most aspects of facial rejuvenation, volume contouring and skin tightening. On the authors experience, the hyperdiluted use of Radiesse®, allows the HCP to give the patient a more global treatment, rather than a local filling/volumization, as the product can more easily be spread on the skin, providing a general skin tightening with progressive, natural and discrete volume gain.
Current Practice and Consensus Statements for Face Treatment
According to experts, the following guidelines for face treatment with CaHA were established. The product can be applied in retroinjection using cannulas in fanning or “asterisks” techniques with 2 to 4 entry points in each hemiface. With needles, short linear threading technique is preferred (FIGURE 1, TABLE 2). For face treatment, the choice is to use a dilution of 1:1 (1.5 mL of diluent) and usually 1 syringe per session is indicated (TABLE 2).
| STATEMENTS FOR USE ON THE FACE | |
| Strong consensus | Agreement |
| Product application can be performed in retroinjection using cannula in fanning or asterisks technique with 2 to 4 entry points per facial side | 100% |
| For face treatments, the preferred dilution is 1:1 (1.5 mL of diluent) | 90% |
| Short linear threading technique can be used with needle | 90% |
| Consensus | Agreement |
| Usually 1 syringe per session is indicated | 80% |
TABLE 2: General consensus statements for use on the face.
Neck and Décolletage
Rejuvenation procedures for the neck and décolletage had a great increase in recent years with the awareness that these areas can reveal a person’s age as reliably as the face. Whilst the use of CaHA for neck and décolletage treatment is off-label, its ability to induce extracellular matrix remodeling after subdermal injection could have significant impact to promote local skin tightening.14,25 Fat accumulation, skin laxity, and ptosis of the underlying anatomical structures, coupled with the regular twisting and swiveling motions as well as platyma contractions, often contribute to neck senescence, manifested by prominent platysmal bands, horizontal rhytides (so-called necklace lines), and sagging skin.14,26,27 CaHA hyperdiluted with lidocaine and/or preserved saline may be used to stimulate neocollagenesis, reducing fine wrinkling and improving skin quality.14 The chest and décolletage are particularly susceptible to the collective damage from UV exposure. Photodamage amplifies the effects of intrinsic aging producing skin laxity and atrophy, visible lines and wrinkles, skin roughness, hyperpigmentation and telangiectasias.14,28 The décolletage skin has a thinner epidermis and dermis compared to the face, with variable distribution of subcutaneous fat and a relative paucity of pilosebaceous units, making deep or ablative treatments not often indicated.28 In one study25, the authors describe a simple and effective technique for addressing horizontal neck lines by the injection of hyperdiluted CaHA.Another trial6 evaluated the collagen- and elastin-stimulating effects of diluted CaHA in subjects with skin laxity in the neck and décolletage. Twenty subjects received at baseline and after 4 months, multiple, linear, subdermal injections of CaHA with different dilutions of preserved saline, according to the skin thickness: 1:2 dilution (normal skin), 1:4 (thin skin), and 1:6 (atrophic skin). Changes to skin mechanical properties were measured by ultrasound scanning and cutometry. Subject and investigator satisfaction were evaluated using the Global Aesthetic Improvement Scale. Immunohistochemical data on increased collagen and elastin production correlated with improvement in skin elasticity and pliability evaluated by cutometry, and with ultrasound-assessed increase in dermal thickness. Subject and investigator satisfaction were high, and the procedure was well tolerated. The authors concluded that injection of diluted CaHA is very effective for skin tightening of neck and décolletage areas.
Current Practice and Consensus Statements of Neck Treatment
According to experts, the following guidelines for neck treatment with CaHA were established. Product application can be performed by cannula in retroinjection (fanning or asterisks technique) with 3 to 5 entrance points (FIGURE 1, TABLE 3). The short linear threading technique with needle is an alternative technical option. For neck treatment the dilution of 1:2 to 1:4 (3 to 6 mL of diluent) is usually indicated according to patient’s skin thickness. Usually 1 syringe in each session is indicated (TABLE 3).
| STATEMENTS FOR NECK TREATMENT | |
| Strong consensus | Agreement |
| Usually 1 syringe per session is indicated | 100% |
| Product application can be performed by cannula in retroinjection (fanning or asterisks technique) with 3 to 5 entrance points | 100% |
| Consensus | Agreement |
| For neck treatment the dilution of 1:2 to 1:4 (3 to 6 mL of diluent) is usually indicated according to patient’s skin thickness | 80% |
| Short linear threading technique with needle is an alternative option | 80% |
TABLE 3: General consensus statements for neck treatment.
Current Practice and Consensus Statements of Décolletage Treatment
According to experts, the following guidelines for CaHA décolletage treatment were established. It can be performed by short linear threading technique with needle or in retroinjections (fanning or asterisks) with cannula (FIGURE 1, TABLE 4). Commonly the dilution of 1:2 to 1:4 (3 to 6 mL of diluent) is indicated according to patient’s skin thickness. Usually 0.5 to 1 syringe per session is indicated (TABLE 4).
| STATEMENTS FOR DÉCOLLETAGE TREATMENT | |
| Strong consensus | Agreement |
| Décolletage treatment can be performed by short linear threading with needle or by cannula retroinjections (fanning or asterisks) | 100% |
| Usually 0.5 to 1 syringe per session is indicated | 100% |
| Consensus | Agreement |
| For décolletage treatemtn the dilution of 1:2 to 1:4 (3 to 6 mL of diluent) is indicated according to patient’s skin thickness | 80% |
TABLE 4: General consensus statements for décolletage treatment.
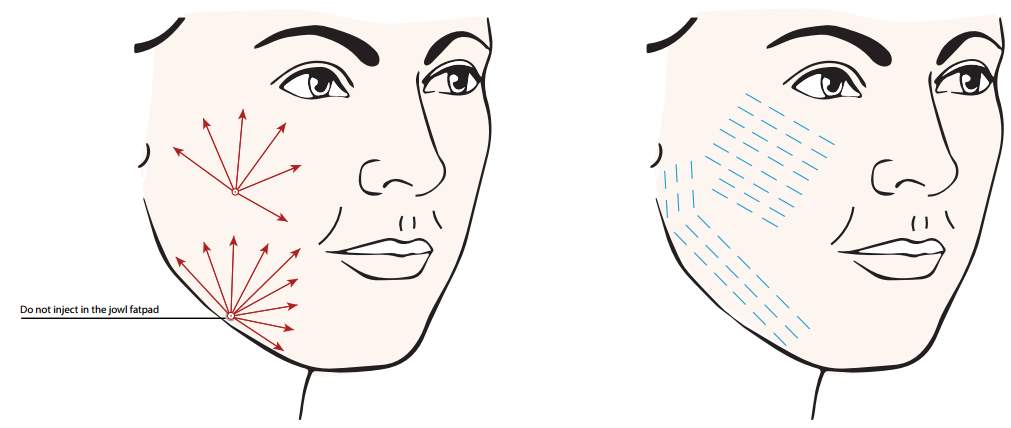
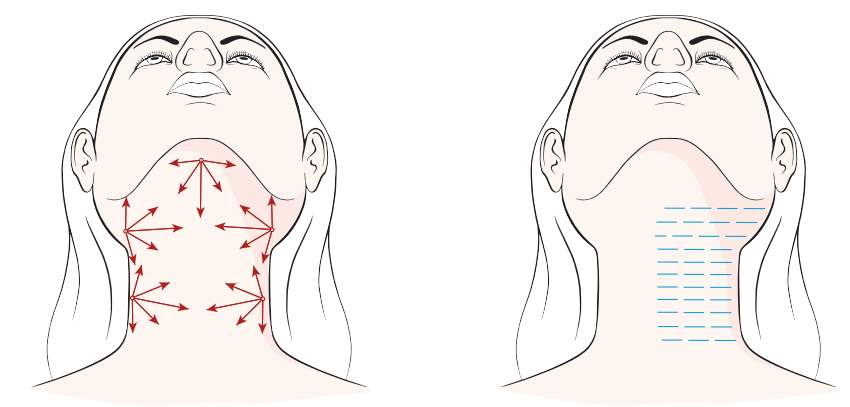
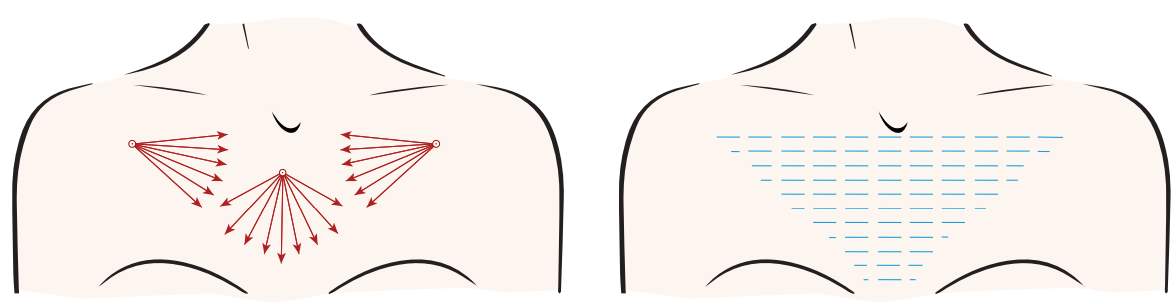
FIGURE 1: Techniques for CaHa biostimulation of face, neck and décolletage.
Buttocks and Thighs
Buttocks and thighs play an important role in maintaining or improving body contours. Individuals present with a wide range of complaints: generalized lipohypertrophy or lipohypotrophy, skin-contour irregularities, gluteal sagging (ptosis), localized fat atrophy due femoral bone compression in individuals who remain seated for long periods, age-related discolorations, and cellulite-induced skin-surface irregularities.14 Different fillers may be used alone for augmentation and improvement of irregularities of the skin surface.29-31 Increasing strength and elasticity of the dermis and superficial fascia are important aims when treating skin laxity and also cellulite dimples. Such approaches require stimulation of new collagen formation and subsequent dermal remodeling. One procedure that has unequivocally demonstrated collagen-stimulating properties and improvements in skin laxity in different aesthetic indications is CaHA injections.10 When associated to microfocused ultrasound, the biostimulatory effect of both treatments can be synergic. One study10 evaluated the effects of microfocused ultrasound with visualization (MFU-V; Ultherapy-Merz Pharmaceuticals GmbH) in combination with diluted Radiesse® on cellulite appearance. Twenty women with skin laxity and moderate-to-severe cellulite on the buttocks and thighs were retrospectively enrolled. MFU-V was applied and immediately followed by subdermal CaHA injection (1.5 cc/buttock or thigh). Two independent evaluators reported statistically significant improvements 90 days after the treatment for each item of the cellulite severity scale (P < 0.001). Both procedures were well tolerated, and subject satisfaction was high. In conclusion, combination treatment with MFU-V and diluted CaHA was considered effective for improving skin laxity and the appearance of cellulite on the buttocks and upper thighs.
Current Practice and Consensus Statements on Buttocks Treatment
According to experts, the following guidelines for CaHA buttocks treatment were established. For buttocks skin laxity the product can be applied of a cannula in fanning or asterisks technique. The product should be applied mainly on the upper and lateral portions of the buttocks and also on the cellulite dimples (FIGURE 2, TABLE 5). Short linear threading technique may also be used with needles. Usually 1 syringe per buttock’s side per session is indicated. For buttocks’s skin laxity the dilution may range from 1:1 to 1:4 (1.5 mL to 6 mL of diluent), while for the cellulite dimples lower dilutions (1:1 or 1:2) can be used (TABLE 5).
| STATEMENTS FOR BUTTOCKS TREATMENT | |
| Strong consensus | Agreement |
| For buttocks skin laxity the suggested technique is cannula fanning or asterisk injection | 100% |
| The product should be applied mainly on the upper and lateral portion of the buttocks and on cellulite dimples | 100% |
| Usually 1 syringe per buttock’s side per session is indicated | 100% |
| For buttocks’s skin laxity the dilution may range from 1:1 to 1:4 (1.5 mL to 6 mL of diluent) | 100% |
| For cellulite dimples lower dilutions (1:1 or 1:2) can be used | 90% |
| Short linear threading technique can be option used with needles | 90% |
TABLE 5: General consensus statements for buttocks treatment.
Current Practice and Consensus Statements on Thighs Treatment
According to experts, the following guidelines for CaHA thigh treatment were established. The product can be applied to the inner as well as to the posterior thigh areas. The most used technique for skin laxity is multiple cannula passes in fanning or asterisks injections (FIGURE 2, TABLE 6). Short linear threading technique can also be used with needle. Usually 1 syringe per thigh area (inner or posterior) is indicated. The recommended CaHA dilution may range from 1:1 to 1:4 (1.5 to 6 mL of diluent) according to the degree of laxity (TABLE 6).
| STATEMENTS FOR THIGHS TREATMENT | |
| Strong consensus | Agreement |
| The product can be applied to the inner as well as to the posterior thigh areas | 100% |
| Usually 1 syringe per thigh area (inner or posterior) is indicated | 100% |
| The recommended CaHA dilution may range from 1:1 to 1:4 (1.5 to 6 mL of diluent) according to the degree of laxity | 100% |
| The most used technique for skin laxity is multiple cannula passes in fanning or asterisks injections | 90% |
| Short linear threading technique can also be used with needle | 90% |
TABLE 6: General consensus statements for thighs treatment.
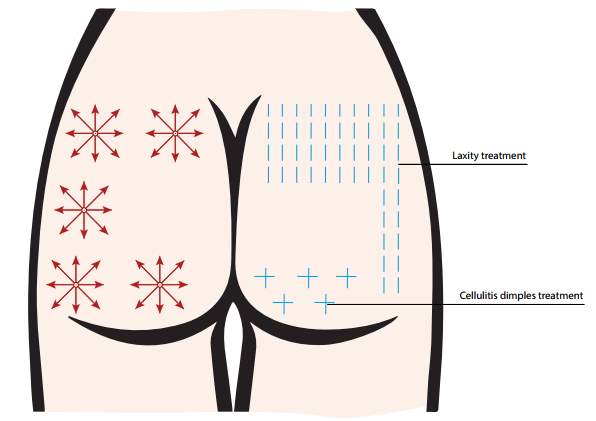
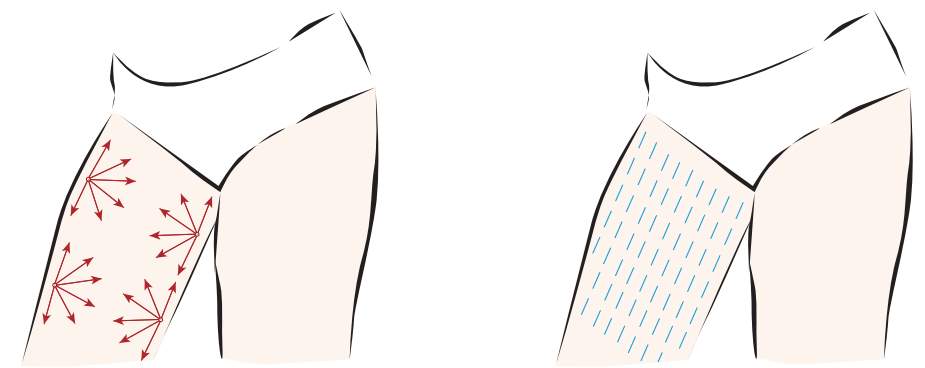
FIGURE 2: Techniques for buttocks and thighs CaHA application.
Abdomen (stomach)
The abdomen appearance over the years suffers the influence of several external variables like diet, exercise and, in women, pregnancy, along with genetics and intrinsic age-related changes. A body-vectoring technique using lidocaine-diluted CaHA injections demonstrated notable reductions in skin flaccidity and increases in skin density and thickness in the abdomen and thighs.32 In 2017, Lapatina and Pavlenko33 evaluated the effectiveness and safety of hyperdiluted CaHA for skin tightening in a case series of 10 women with skin laxity in the abdomen using ultrasound. CaHA diluted 1:4 with saline solution was injected subdermally using a linear-threading technique. The authors conclude that CaHA improved skin elasticity and increased abdominal dermal thickness after only a single treatment and that the procedures were well tolerated.
Current Practice and Consensus Statements of Abdomen Treatment
According to experts, the following guidelines for CaHA abdomen treatment were established. The product application can be performed both by cannula (fanning or asterisk technique) and needles (short linear threading), distributed to the four stomach quadrants (FIGURE 3, TABLE 7). Short Needle linear threading technique is particularly indicated for the periumbilical region. Product dilution can range from 1:1 to 1:4 (from 1.5 to 6 mL of diluent). Usually 1 syringe is indicated for the upper abdominal region and another one is needed for the lower half per session (TABLE 7).
| STATEMENTS FOR ABDOMEN TREATMENT | |
| Strong consensus | Agreement |
| Product dilution can range from 1:1 to 1:4 (from 1.5 to 6 mL of diluent) | 100% |
| CaHA injections can be performed by cannula (fanning or asterisk technique) distributed to the four stomach quadrants | 90% |
| Short linear threading technique may also be used with needles | 90% |
| Needle short linear threading technique is particularly indicated for the periumbilical region | 90% |
| Consensus | Agreement |
| Usually 1 syringe is indicated for the upper abdominal region and another one is needed for the lower portion | 80% |
TABLE 7: General consensus statements for abdomen treatment.
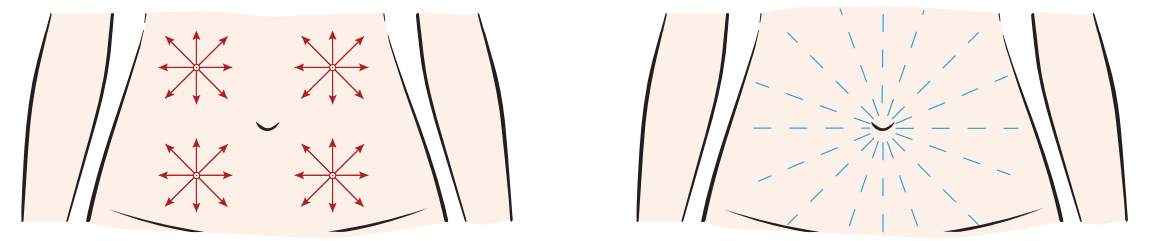
FIGURE 3: Technique for application of CaHA on the abdomen.
Arms
As part of the natural aging process, skin elasticity and firmness of the upper arms begin to decrease, and the underlying layers of fat, muscle, and bone also suffer atrophic changes.13 These biological alterations frequently induce local flaccidity, along with visible signs of aging, such as loose-hanging skin and wrinkles of the upper arms. While exercising may be helpful in improving muscle tone and strength, it will not improve arm fat volume changes and skin laxity, which have traditionally been corrected by subcutaneous fat and excessive skin removal by surgery.13,14 In a prospective and open-label study13 30 subjects seeked improvement in the esthetic appearance of their upper arms. They received CaHA injections (1.5 mL/arm/visit) at two separate visits, 1 month apart. Subjects returned for a follow-up visit 4 months after the second treatment. Assessments of flaccidity and volume improved significantly compared with baseline at the post-treatment visit and also between visits. Compared with baseline, 77% of subjects were rated as considerably improved (good or great improvement). In another study,33 an improvement in skin elasticity of the arms was observed by cutometry after hypediluted CaHA injection (1:2 dilution with normal saline solution and 2% lidocaine) subdermally using a short, linear-threading technique.
Current Practice and Consensus Statements on Arm Treatment
According to experts, the following guidelines for CaHA arm treatment were established. The usually recommended technique is retroinjection with cannula in 2 to 4 fannings distributed along the inner arm (FIGURE 4, TABLE 8). Usually 0.5 to 1 syringe per arm, is indicated in each session. The preferred dilution range is 1:2 to 1:4 (3 to 6 mL of diluent) (TABLE 8).
| STATEMENTS FOR ARM TREATMENT | |
| Strong consensus | Agreement |
| Usually 0.5 to 1 syringe per arm is indicated in each session | 100% |
| Preferred dilution range is 1:2 to 1:4 (3 to 6 mL of diluent) | 90% |
| Recommended technique is retroinjection with cannula in 2 to 4 fannings distributed along the inner arm | 90% |
TABLE 8: General consensus statements for arm treatment.
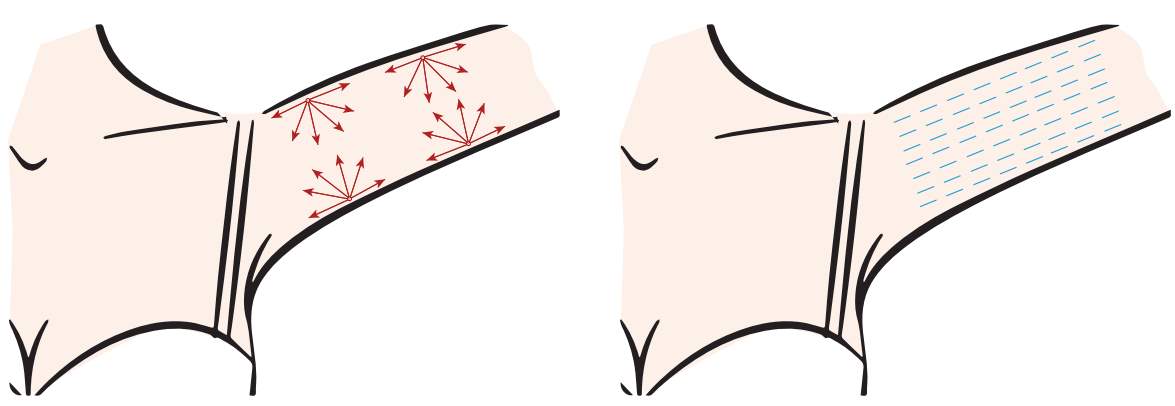
FIGURE 4: Technique for CaHA arm application.
Knees and Elbows
The knees and elbows show increased laxity with age. Although there are no clinical studies with CaHAtreatment of these areas, in the authors’ experience the local aged appearance can be improved with the CaHA-generated collagen stimulation.
Current Practice and Consensus Statements on Knee Treatment
According to experts, the following guidelines for CaHA knee treatment were established. Product application can be performed by fanning retroinjection with cannula or by short linear threading technique with needles. Treatment is suggested mainly for the region located above the patella. Recommended dose per session is 1 syringe in total (half per side) (FIGURE 5, TABLE 9). There was no consensus on the dilution used in the knees, but the authors presented experience with different dilutions, ranging from 100% (1.5 mL) to 400% (6 mL).
| STATEMENTS FOR KNEE TREATMENT | |
| Strong consensus | Agreement |
| Product application can be perfomed by fanning retroinjection with cannula or by short linear threading technique with needles | 100% |
| Treatment is suggested mainly for the region located above the patella | 100% |
| Consensus | Agreement |
| Recommended dose per session is 1 syringe in total (half per side) | 80% |
TABLE 9: General consensus statements for knee treatment.
Current Practice and Consensus Statements on Elbow Treatment
According to experts, the following guidelines for CaHA elbows treatment were established. Product application can be performed by injecting the product in a short linear threading technique with needle. It is suggested treatment mainly of the superior region of the elbow with 1 syringe in total (half per side) in each session (FIGURE 5, TABLE 10).
| STATEMENTS FOR ELBOW TREATMENT | |
| Strong consensus | Agreement |
| It is suggested treatment mainly of the superior region of the elbow | 100% |
| Product application can be performed by injecting the product in a short linear threading technique with needle | 90% |
| It is recommended 1 syringe in total (half per side) per session | 90% |
TABLE 10: General consensus statements for elbow treatment.
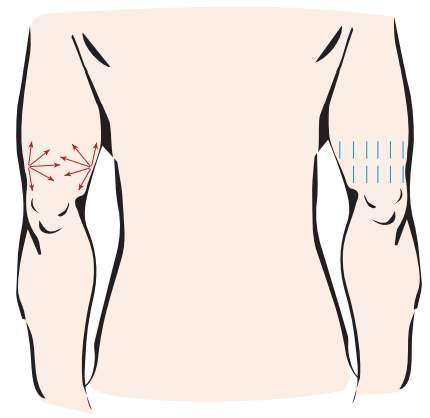
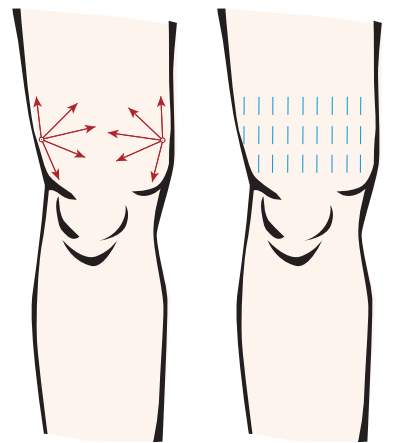
FIGURE 5: Techniques for knees and elbows CaHA application.
Post-procedure and Follow-up Instructions
Patient counseling and education by the physician about the procedure as well as consistent adherence to pretreatment and post treatment self-care practices by the patient, are critical for optimal results. In general, exposure of the treated area to excessive sun, heat, and ultraviolet light should be minimized for approximately 24 hours or until any initial swelling and erythema have faded. An ice or cold pack can be used to minimize tenderness, swelling and bruising. During the treatment session, massage of the treated area may be required to ensure that CaHA is distributed evenly.34 If nodules develop, they may be treated with lidocaine or saline followed by vigorous massage. Nodules that do not resolve may respond to series of three or more injections of 5-fuorouracil (5-FU), triamcinolone, and lidocaine, or 5-FU and lidocaine.35 The follow-up treatment and periodic maintenance treatments may also be needed. Treatment longevity depends on many factors, such as the patient’s age and metabolism, and the relative dynamic motion of the area in which the implant is placed. Many published reports state that results remain almost unchanged until 12-18 months, though some results can be noted 24 months post injection.36
Current Practice and Consensus Statements
According to experts, the following guidelines for follow-up treatment and massage were established. After initial treatment cicle, one maintenance session is suggested, within a range of 12 to 18 months. The initial massage should be performed by the physician right after the procedure aiming the evenly spread of the product in the treated area. It can also be recommended for the patient’s own performance at the injection site, 2 times a day for 3 to 7 days (TABLE 11).
| FOLLOW-UP TREATMENT | |
| Strong consensus | Agreement |
| After initial treatment cicle, 1 follow-up session is suggested, within a range of 12 to 18 months | 100% |
| MASSAGE | |
| Strong consensus | Agreement |
| The initial massage should be performed by the physician after the procedure with the aim of an even spread of the product in the treated area | 100% |
| Consensus | Agreement |
| Self massage can be recommended for the patient at the injection site (2 times a day for 3 to 7 days) | 80% |
TABLE 11: General consensus statements for follow-up treatment and massage.
Summary
Radiesse® (calcium hydroxylapatite – CaHA, Merz Pharmaceuticals) is a very effective agent for many areas of facial soft tissue augmentation and is associated with a high and well-established safety profile. The rising popularity of noninvasive or minimally invasive aesthetic procedures in the face over the last decade has led to greater demand for body rejuvenation interventions, particularly in neck, décolletage, arms and other corporal areas in order to minimize the discrepancy between body and face appearance.The characteristic of Radiesse® of long-term collagen stimulator provide it with great versatility of use.This consensus provides recommendations for the use of hyperdiluted CaHA as a biostimulatory agent for face and body rejuvenation improving skin quality and firmness.
References
- Loghem JV, Yutskovskaya YA, Werschler W. Calcium hydroxylapatite over a decade of experience. J Clin Aesthet Dermatol. 2015;8:38-49.
- Carruthers J, Burgess C, Day D, Fabi SG, Goldie K, Kerscher M, Nikolis A,Pavicic T, Rho NK, Rzany B, Sattler G, Sattler S, Seo K, Werschler WP, Carruthers A. Consensus Recommendations for Combined Aesthetic Interventions in the Face Using Botulinum Toxin, Fillers, and Energy-Based Devices. Dermatol Surg. 2016 May;42(5):586-97.
- Berlin AL, Hussain M, Goldberg DJ. Calcium hydroxylapatite filler for facial rejuvenation: a histologic and immunohistochemical analysis. Dermatol Surg 2008;34(Suppl 1): S64-7.
- Tzikas TL. A 52-month summary of results using calcium hydroxylapatite for facial soft tissue augmentation. Dermatol Surg. 2008;34(Suppl 1):S9-15.
- Silvers SL, et al. Prospective, Open-Label, 18-Month Trial of Calcium Hydroxylapatite (Radiesse) for Facial Soft-Tissue Augmentation in Patients with Human Immunodeficiency Virus–Associated Lipoatrophy: One-Year Durability. Plast Reconstr Surg. 2006;118:34S.
- Yutskovskaya YA, Kogan EA. Improved Neocollagenesis and Skin Mechanical. Properties After Injection of Diluted Calcium Hydroxylapatite in the Neck and Décolletage:A Pilot Study. J Drugs Dermatol. 2017 Jan 1;16(1):68-74.
- Coleman KM, et al. Neocollagenesis after Injection of Calcium Hydroxylapatite Composition in a Canine Model. Dermatol Surg. 2008;34:S53-S55.
- Yutskovskaya Y, et al. A Randomized, Split-Face, Histomorphologic Study Comparing a Volumetric Calcium Hydroxylapatite and a Hyaluronic Acid-Based Dermal Filler. J Drugs Dermatol. 2014;13(9):47-52.
- Courderot-Masuyer C, et al. Evaluation of lifting and antiwrinkle effects of calcium hydroxylapatite filler. In vitro quantification of contractile forces of human wrinkle and normal aged fibroblasts treated with calcium hydroxylapatite. Journal of Cosmetic Dermatology. 2016: 1-9.
- Casabona G, Pereira G. Microfocused Ultrasound with Visualization and Calcium Hydroxylapatite for Improving Skin Laxity and Cellulite Appearance. Plast Reconstr Surg Glob Open. 2017 Jul 25;5(7):e1388.
- Pavicic T. Complete biodegradable nature of calcium hydroxylapatite after injection for malar enhancement: an MRI study. Clinical, Cosmetic and Investigational Dermatology. 2015;8:19-25.
- Wasylkowski VC. Body vectoring technique with Radiesse® for tightening of the abdomen, thighs, and brachial zone. Clinical, Cosmetic and Investigational Dermatology. 2015;8:267-273.
- Amselem M. Radiesse®: a novel rejuvenation treatment for the upper arms. Clin Cosmet Investig Dermatol. 2015 Dec 29;9:9-14.
- Fabi SG, Burgess C, Carruthers A, Carruthers J, Day D, Goldie K, Kerscher M, Nikolis A, Pavicic T, Rho NK, Rzany B, Sattler S, Seo K, Werschler WP, Sattler G. Consensus Recommendations for Combined Aesthetic Interventions Using Botulinum Toxin, Fillers, and Microfocused Ultrasound in the Neck, Décolletage, Hands, and Other Areas of the Body. Dermatol Surg. 2016 Oct;42(10):1199-1208.
- Dallara JM, Baspeyras M, Bui P, Cartier H, Charavel MH, Dumas L. Calcium hydroxylapatite for jawline rejuvenation: consensus recommendations. J Cosmet Dermatol. 2014 Mar;13(1):3-14.
- van Loghem JA, Humzah D, Kerscher M. Cannula Versus Sharp Needle for Placement of Soft Tissue Fillers: An Observational Cadaver Study. Aesthet Surg J. 2016 Dec 16. pii: sjw220. [Epub ahead of print] PubMed PMID: 27986754.
- Pavicic T, Frank K, Erlbacher K, Neuner R, Targosinski S, Schenck T, Gotkin RH, Cotofana S. Precision in Dermal Filling: A Comparison Between Needle and Cannula When Using Soft Tissue Fillers. J Drugs Dermatol. 2017 Sep 1;16(9):866-872.
- Beer K. Dermal Fillers and Combinations of Fillers for Facial Rejuvenation. Dermatol Clin. 2009;27:427-432.
- Presti P, Yalamanchili H, Honrado CP. Rejuvenation of the aging upper third of the face. Facial Plast Surg. 2006;22:91-6.
- Carruthers J, Carruthers A. Botulinum toxin A in the mid and lower face and neck. Dermatol Clin. 2004;22:151-8.
- Baspeyras M, Dallara JM, Cartier H, Charavel MH, Dumas L. Restoring jawline contour with calcium hydroxylapatite: A prospective, observational study. J Cosmet Dermatol. 2017 Sep;16(3):342-347.
- Graivier MH, Bass LS, Busso M, et al. Calcium hydroxylapatite (Radiesse) for correction of the mid- and lower face: consensus recommendations. Plast Reconstr Surg. 2007;120(6 Suppl):55S-66S.
- Rohrich RJ, Pessa JE. The fat compartments of the face: anatomy and clinical implications for cosmetic surgery. Plast Reconstr Surg. 2007; 119:2219-27.
- Rohrich RJ, Pessa JE, Ristow B. The youthful cheek and the deep medial fat compartment. Plast Reconstr Surg. 2008;121:2107-12.
- Chao YY, Chiu HH, Howell DJ. A novel injection technique for horizontal neck lines correction using calcium hydroxylapatite. Dermatol Surg. 2011 Oct;37(10):1542-5.
- Dayan SH, Arkins JP, Chaudhry R. Minimally invasive neck lifts: have they replaced neck lift surgery? Facial Plast Surg ClinNorth Am. 2013;21:265-70.
- Prager W, Bee EK, Havermann I, Zschocke I. IncobotulinumtoxinA for the treatment of platysmal bands: a single-arm, prospective proof-of concept clinical study. Dermatol Surg. 2015;41(Suppl 1):S88-92.
- Peterson JD, Goldman MP. Rejuvenation of the aging chest: a review and our experience. Dermatol Surg. 2011;37:555-71.
- Mazzuco R, Sadick NS. The use of poly-L-lactic acid in the gluteal area. Dermatol Surg. 2016;42:441-3.
- Goldberg DJ, Hornfeldt CS. Safety and efficacy of microfocused ultrasound to lift, tighten, and smooth the buttocks. Dermatol Surg. 2014;40:1113-7.
- Sasaki G, Tevez A. Microfocused ultrasound for nonablative skin and subdermal tightening to the periorbitum and body sites: preliminary report on eighty-two patients. J Cosmet Dermatol Sci Appl. 2012;2:109-16.
- Cogorno Wasylkowski V. Body vectoring technique with Radiesse for tightening of the abdomen, thighs, and brachial zone. Clin Cosmet Investig Dermatol. 2015;8:267-73.
- Lapatina NG, Pavlenko T. Diluted Calcium Hydroxylapatite for Skin Tightening of the Upper Arms and Abdomen. J Drugs Dermatol. 2017 Sep 1;16(9):900-906.
- Day D. Counseling patients on facial volume replacement and adherence with post treatment instructions. Patient Preference and Adherence. 2010;4: 273-281.
- Funt D and Pavicic T. Dermal fillers in aesthetics: an overview of adverse events and treatment approaches. Clin Cosmet Investig Dermatol. 2013;6: 295-316.
- Jacovella PF. Use of calcium hydroxylapatite (Radiesse®) for facial augmentation. Clinical Interventions in Aging. 2008;3(1):161-174.
Cite This Work
To export a reference to this article please select a referencing stye below:
Related Services
View all


Related Content
All TagsContent relating to: "Biosciences"
Bioscience is a field of study that focuses on various aspects of natural and life sciences. Bioscience consists of subjects such as cell and molecular biology, environmental biology, genetics, marine biology, physiology, zoology, and much more.
Related Articles

DMCA / Removal Request
If you are the original writer of this dissertation and no longer wish to have your work published on the UKDiss.com website then please: