Improving Communication Skills in Preschool Students with Communication Delays
Info: 7954 words (32 pages) Dissertation
Published: 20th Aug 2021
Abstract
This study provides descriptive information on diagnoses, conditions and likelihood of later literacy learning difficulties as well as data to support the use of early childhood special education (ECSE) supports and services and the effects they have on children with Speech Language Impairments (SLI).
This study explores the experiences self-reported by current Speech Language Pathologists (SLPs) across Ohio. Surveys were sent to SLPs who served children ages 3-5. Respondents described materials and activities made available to children and the children’s communication behaviors at home as well as any medical/health information that was relevant for consideration by ECSE teachers. Respondents also gave information related to classroom supports for teachers as well as home supports for parents/guardians.
Language is the use of systematic, arbitrary, and socially agreed upon signals (words and sentences) to convey meaning within a group or community for purposes of communicating (Feldman, 2005). Receptive language refers to the ability to understand information communicated from an outside source (e.g. book, person) and expressive language refers to one’s ability to produce this symbolic communication. Developmental language disorders are persistent and present significant limitations on the ability to learn the language of the community. Characteristics of language disorders include limited understanding or production of vocabulary, misuse of words, difficulty expressing or following ideas, immature grammatical patterns, difficulty following directions, or altered patterns of conversation (Feldman, 2005).
The question addressed by this research was what are effective communication strategies for improving communication skills in preschool students with communication delays? The purpose was to a) determine types of communication disorders and the impact those disorders have on students, as well as to b) provide effective strategies for teachers, Speech Language Pathologists (SLPs), and parent/guardians. The literature review answers the following four main questions that present the rationale for this study: What is communication and effective communication skills? What are communication disorders, including types, symptoms, causes, treatments, prevalence? What are expectations for preschool children according to Early Learning Developmental Standards (ELDS)? And what are strategies for improvement?
Data to Support the Use of Early Childhood Special Education
Teachers in the professional community may learn helpful interventions they can use in the classroom to support students with communication delays. For example, teachers, SLPs, and parents may learn the importance of early detection and therapy services in early years. Speech or language impairments are the most prevalent disability category for children ages 3-5 served under the Individuals with Disabilities Education Act (2004) and the second most prevalent disability category for students ages 6 through 21 (American Speech-Language Hearing Association, 2016). Children ages 0-3 may be served for language delays through early intervention services of IDEA (i.e. Part B). Children as early as the age of three are referred for preschool services through parent referrals, community or government organization referrals (e.g., Help Me Grow, Department of Developmental Disabilities) or physician referrals. Often when intervention begins at this early age the need for speech-language therapy is diminished once the child has reached school age; in school-aged children who have no obvious genetic or neurologic condition, the prevalence of language disorders is only approximately 2% to 3% (Feldman, 2012). Many of these students have Individualized Education Plans (IEP) in the category of Speech-Language Impairment.
Effective Communication
Language is the expression of human communication, either spoken or written, through which ideas, information, emotions, and beliefs can be shared (oxforddictionaries.com, 2017). Children who are typically developing master the fundamentals of language and speech beginning at birth. Language and speech skills serve a pivotal role in learning and social relationships. Management and treatment can improve language and speech skills substantially and reduce the functional impact of persistent disorders. Speech problems can include stuttering, substituting, adding or dropping off sounds (e.g. “poo” for “spoon”), mispronunciations of words, and unintelligible language that is unable to be understood by listeners. Some examples of mispronunciations that may or may not be intelligible include making the “w” sound for an “r” sound (“wabbit” for “rabbit”), “d” for “th” (“dis” for “this”), or “t” for “c” (“tup” for “cup”) (American Speech-Language Hearing Association, 2016).
During the critical period of the first five years of life, children learn language by participating in back-and-forth interactions with the important adults and peers in their lives (Feldman, 2005). When a child sends a message, whether it be with a gesture, a sound, a word, or through Augmentative and Alternative Communication (AAC) guardians’ responses serve as helpful feedback in the language-learning process for every child. If a child is communicating less than others his age, he is unlikely to receive as much of this essential feedback. Because he is not talking, adults naturally communicate with him less, which means he does not get the optimal, helpful input he needs to build his language skills. This is why it’s so important not to ignore any sign that a child’s communication development may be delayed. Some parents are advised that their child will likely “grow out of it”, and they simply wait for the child to catch up. But a “wait and see” approach can be very detrimental during this critical learning phase. Since children with delayed speech or language delays cannot participate fully during activities and conversations, they may fall even further behind if they are not provided with the help they need. On the other hand, when a child with a speech delay or language delay receives extra support from the important adults in his life, he can make significant gains. Early speech therapy intervention is critically important for these children to develop the communication skills necessary for future success in their academic and personal lives (The Hanen Centre, 2016).
Risk Factors
Numerous factors can put infants and toddlers at risk for atypical developmental progress and outcomes. Some factors are well established; others continue to be identified. Some of the most common risk factors include genetic or congenital conditions (cleft palate, Down Syndrome, Fragile-X syndrome), severe sensory impairments (deafness, blindness), neuropsychiatric disorders (autism spectrum disorder [ASD]), and family history of disability. Biological/medical risk factors include conditions such as low birth weight, respiratory distress syndrome, severe asphyxia, fetal alcohol syndrome, or severe brain hemorrhage, may result in immediate or later difficulties. Environmental risk factors include conditions such as advanced or very young maternal age, parental substance use, parental psychiatric disorders, parental abuse or neglect, exposure to chemical toxins, or poverty. Risk factors can occur singly or in combination and can result in a range of developmental difficulties (Paul & Roth, 2011). Therefore, identifying children who have language and speech delays in toddler-preschool period should be a priority (Feldman, 2012).
If it is determined that the child is eligible for services by an SLP as a member of the comprehensive evaluation team, the student will begin receiving speech therapy services. Outside agencies may offer therapy services that take place in medical clinics and schools may offer school-based services during the day.
Communication Disorders
Effective communication includes verbal and nonverbal communication, body language, listening and speaking skills and visual communication. Characteristics of language disorders include limited understanding or production of vocabulary, misuse of words and their meanings, difficulty expressing or following ideas, immature grammatical patterns, and difficulty following directions, or altered patters of conversation (Feldman, 2005).
Speech disorders are persistent delays and deficits in the development of speech skills and voice quality. Speech disorders include problems in the production of speech sounds, disruptions in the flow or rhythm of speech, problems with voice pitch, volume or quality, and poor intelligibility (Feldman, 2012).
Some of the characteristics seen in students with language delays may include limited interest in social interactions, failure to respond when one’s name is called, babbling, limited use of gestures such as pointing, delayed acquisition of first words, slow growth of vocabulary or utterance length, poor speech intelligibility for development level and/or inadequate feeding and swallowing skills (Paul & Roth, 2011). Many times a child’s parent or primary caregiver is able to understand them and their wants and needs, but other listeners cannot. This is problematic because every child needs to be able to communicate his or her wants, needs and ideas effectively in all environments including home and school.
Table 1 summarizes typical language from birth to school age, according to Feldman and Boyse (2005) and Dosman et al. (2012). From infancy a child should reach developmental milestones. Some of these milestones include babbling beginning from three to six months; imitating sounds and saying one to two words at twelve months; between one and two years a child will begin to make his or her wants known and begin saying short sentences; and by preschool age a child should be able to recite nursery rhymes and tell short stories.
Table 1
Normal Milestones in the Development of Language and Speech from Birth to School aged.
| Age | Receptive Skills | Expressive Skills |
| Birth | Turns to source of sound
Shows preference for voices shows interest in faces |
Cries |
| 2 to 4 months | Engaging in interactions | Coos/babbling
Takes turns cooing |
| 6 months | Responds to name
Learns through vision and mouthing |
Babbles |
| 9 months | Understands verbal routines (wave bye-bye)
Maintaining memory, object permanence |
Points
Says ma-ma, da-da |
| 12 months | Follows verbal command
Gestures |
Uses jargon
Imitating sounds Says first word |
| 15 months | Points to body parts by name | Learns words slowly |
| 18 to 24 months | Understand sentences
Pretends Temper tantrums result from limitations |
Learns words quickly
Uses two-word phrases Saying short sentences |
| 24 to 36 months | Answers questions
Follows two-steps commands |
Phrases 50% intelligible
Builds three (or more) word sentences Asks “what” questions |
| 36 to 48 months | Understands much of what is said | Asks “why” questions
Sentences 75% intelligible Masters early sounds: m, b, y, n, w, d, p, and h |
| 48 to 60 months | Understands much of what is said, commensurate with cognitive level | Creates well-formed sentences
Tells stories Identify parts of body Combine verbs and nouns Recite nursery rhymes 100% intelligible |
In the past 20 years, researchers have studied the development of late talkers who are slow to develop expressive language skills in the absence of other identifiable disabilities. These children are typically identified to have speech or language delay between 18 and 30 months of age when parents become concerned that their child, who appears to be developing normally, fails to begin speaking or has a small expressive vocabulary (Paul & Roth, 2011). A variety of criteria have been used to identify these late talking toddlers; most commonly, children are identified because they have a vocabulary size below the 10th percentile for their age (Fenson et al, 2007; Rescorla & Lee, 2000). Studies following these children through the preschool years have shown they tend to combine words later than other children their age (Carson, Klee, Carson & Hine, 2003; Dale, Price, Bishop, & Plomin, 2003), have less advanced sentence structures than other children their age (Dale et al., 2003; Hadley & Holt, 2006; Paul, 1996; Paul & Riback 1993; Thal, Reilly, Seibert, Jeffries & Fenson, 2004), and are delayed in their development of speech sounds (Law, Boyle, Harris, Harkness & Nye, 2000; Paul & Jennings, 1992; Rescorla & Ratner 1996; Rice, Taylor & Zubrick, 2008; Thal, Oroz & McCaw, 1995). Zubrick, Tayor, Rice and Slegers (2007) also reported that late talkers were more likely to be male; to have a family history of language delay; and to have experienced prematurity, low birth weight, or other early neurological growth difficulties. Collectively, the research shows that more than 75% of the children who have been identified as late talking toddlers transitioned into the normal range for vocabulary by 3 years of age and performed within age-appropriate psychometric limits on standardized tests of grammar and discourse skills by kindergarten (Paul, 1996; Rescorla, Dahlsgaard & Roberts, 2000; Rescorla & lee, 2000; Rice et al., 2008; Roos & Weismer, 2008; Whitehurst & Fischel, 1994).
Expectations
On October 9, 2012, the Ohio Board of Education adopted Ohio’s Early Learning and Development Standards in all domains of school readiness. These standards reflect the comprehensive development of children beginning at birth and extending through kindergarten entry. Early Learning and Development Standards describe key concepts and skills that young children develop during the birth-to-five-year period. Their purpose is to support the development and well-being of young children and to foster their learning. The standards promote the understanding of early learning and development, provide a comprehensive and coherent set of early childhood educational expectations for children’s development and learning, and guide the design and implementation of curriculum, assessment and instructional practices with young children. Table 2 shows listening and developmental standards to support the development of children from birth to preschool. Because the infant and toddler years are marked by rapid developmental change, the standards for the first three years of life are divided into three meaningful transitional periods: Infants (birth to around 8 months), Young Toddlers (6 to around 18 months), and Older Toddlers (16 to around 36 months). The standards during the pre-kindergarten years (3-5), describe those developmental skills and concepts children should know and be able to do at the end of their pre-kindergarten (Pre-K) experience. The standards within each domain are organized according to strands (the developmental or conceptual components within each domain). Each strand contains one or more topics, the area of focus within each strand, and the standard statements: those concepts and skills children should know and be able to do for the different age groups. Some topics reflect learning and development across the birth-to-five continuum, with Standards for all age levels: infants, young toddlers, older toddlers and Pre-K, whereas other topics pertain only to a specific age. The Standards for Language and Literacy reflect knowledge and skills fundamental to children’s learning of language, reading and writing. Young children’s language competencies pertain to their growing abilities to communicate effectively with adults and peers, to express themselves through language, and to use growing vocabularies and increasingly sophisticated language structures. Early literacy skills include children’s developing concepts of print, comprehension of age appropriate text, phonological awareness, and letter recognition. Research has identified early skills of language and literacy as important predictors for children’s school readiness and their later capacity to learn academic knowledge (Ohio Department of Education, 2017).
Table 2
Birth to Preschool Listening and Speaking Developmental Standards in Ohio
| Infants
(Birth – 8 months) |
Young Toddlers
(6-18 months) |
Older Toddlers
(16-36 months) |
Pre-Kindergarten
(3-5 years) |
| Strand: Listening and Speaking | |||
| Topic: Receptive Language and Comprehension | |||
| Attend and respond to language and sounds. | Show understanding of simple requests and statements referring to people and objects around them. | Show understanding of requests and statements referring to people, objects, ideas and feelings. | Demonstrate understanding of increasingly complex concepts and longer sentences. |
| Demonstrate interest in and use words that are new or unfamiliar in conversation and play. | Ask meanings of words. | ||
| Topic: Expressive Language | |||
| Experiment intentionally with sound inflection and gestures in different ways to express wants, needs or feelings | Begin to use single words and conventional gestures to communicate with others. | Combine words to express complex ideas, or requests. | Use language to communicate in a variety of ways with others to share observations, ideas, and experiences; problem-solve, reason, predict and seek new information. |
| With modeling and support, describe experiences with people, places and things. | Speak audibly and express thoughts, feelings and ideas clearly (articulation). | ||
| Use drawings or other visuals to add details to verbal descriptions. | |||
| With modeling and support, use the conventions of standard English. (Grammar)
|
|||
| With modeling and support, use words acquired through conversations and shared reading experiences | |||
| With modeling and support, determine the meaning of unknown words/concepts using the context of conversations, pictures that accompany text or concrete objects (vocabulary) | |||
| Identify real-life connections between words and their use (vocabulary) | |||
| With modeling and support, explore relationships between word meanings | |||
| Topic: Social Communication | |||
| Attempt to respond to basic forms of social communication with the appropriate facial expression, vocalization and/or gesture | Participate in and often initiate basic communications with family members or familiar others | Participate in and often initiate communication according to commonly accepted expectations with family members and in social groups | With modeling and support, follow typical patterns when communicating with others |
| With modeling and support, continue a conversation through multiple exchanges | |||
Strategies for Improving Speech and Language Intelligibility
Squires and Hastings (2002) define Intelligibility as how well a person’s speech is understood by other individuals. While typical developing children of around 4 years of age are intelligible most of the time, children with moderate to severe speech-sound disorders (SSD) can show marked unintelligibility which can impact adversely on functional communication and social participation. Improving intelligibility is typically a key long-term aim for SLPs. One intervention used to improve intelligibility is Phonological Therapy (PT), which includes a combination of phonological awareness activities from Gillon and McNeill’s (2007) program and auditory discrimination and listening activities from Lancaster (2008). The activities include letter-sound knowledge, phoneme identity and phoneme matching, blending, segmentation and phoneme manipulation. Articulation Therapy (AT) is another improvement strategy to improve intelligibility. The principal aim is to develop the child’s ability to discriminate and articulate target sounds correctly in isolation, syllables, words, phrases and sentences (Lousada, et. al. 2014).
Purpose and Research Questions
This study explored the experiences reported to be available by current SLPs across Ohio. Participants described materials and activities made available to children as well as children’s communication behaviors at home and any medical information related to these behaviors. Participants gave information on classroom supports as well as supports for parents at home.
This study provided descriptive information on diagnosis, conditions and likelihood of later literacy learning difficulties, as well as data to support the use of early childhood special education and the effects it has on children with SLI.
Research questions were as follows. A copy of the questions and results can be found in Appendix A.
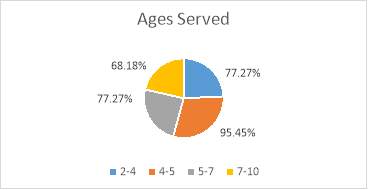
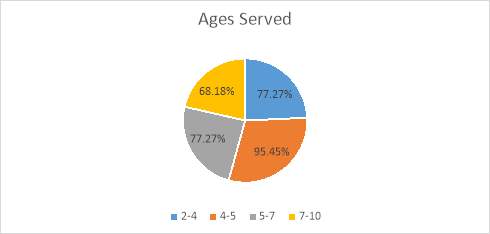
- What ages of children do you serve?
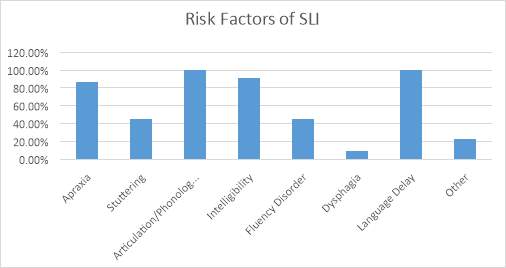
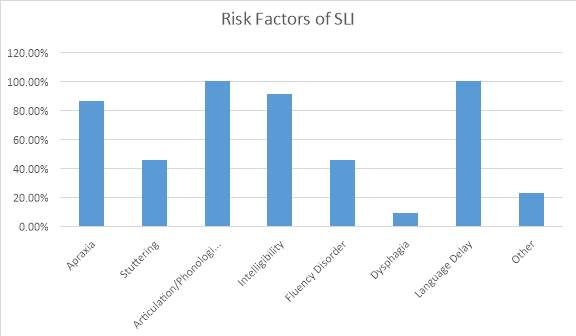
- What common risk factors do you see associated with SLI?
- What types of supports do you offer teachers to better serve children in the classroom with SLI?
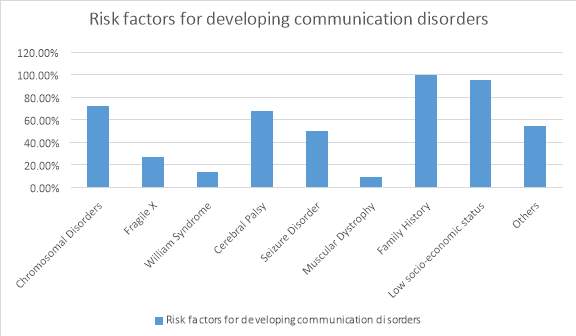
- What risk factors are associated with children developing communication disorders?
- What eligibility criteria or tool do you use for evaluation of young children?
- What percentage of children who you serve have another disability in addition to SLI?
- List any other relevant medical/health information that leads to SLI.
Method
Participants
The participants in the study include 22 female SLPs who were licensed in the State of Ohio and working with young children. These 22 SLPs served children ages 3-5 who have (a) a speech language impairment, (b) a disability other than Speech Language Impairment and who have speech/language needs, and (c) no disability or delay but who have speech/language needs.
Research Design
Survey research was used to collect information from interested SLPs. Questions were created in the form of an online questionnaire or survey and sent electronically to SLPs who were interested and met the qualifications to participate. Participants were able to complete the survey at a location of their choice (home or office). The questions were derived from the researcher and were in the form of yes/no or selecting text boxes for all answer that apply therefore, providing multiple answers to some questions. Participants were also asked to write in any other information that was relevant. Participant were required to answer each question in order to complete the survey. Appendix A includes a copy of the survey with results.
Measures
The survey consisted of eight questions answered by participants. Respondents described materials and activities made available to children and the children’s communication behaviors at home as well as any medical/health information that is relevant. Respondents also gave information on classroom supports as well as supports for parents/guardians at home.
Procedures
Ninety-nine potential participants were contacted via email to inquire if they wanted to participate in the study. Through email, participants were given a consent form which they signed and emailed back. Once consent was given, participants were emailed a web link to complete the survey online. Snowball sampling was used to obtain additional SLP contacts from those who had given consent to continue recruitment efforts. Social media was also used to recruit potential participants; interested participants were asked to send a private message for more information. Participants had the option to complete the survey at a site of their choosing (such as their home or at their office). Appendix B contains a sample of the informed consent document.
Data Analysis
The data for this study was collected using an 8-item questionnaire. Once surveys were completed they were compiled. The first question was to determine the SLP was licensed in Ohio. The following questions were related to diagnosis, risk factors and supports.
Results
The results for each question provided by the 22 Ohio licensed SLPS are listed below.
- What age(s) of children do you serve? (check all that apply)
- What common risk factors do you see associated with speech-language impairments?
(check all that apply).
- What types of supports can/do you offer teachers to better serve children in the classroom with SLI?
All 22 participants reported offering visual aids as a support for teachers. Eighty-one percent reported offering assistive technology as a support in the classroom. Less than fifty percent reported other types of support aids. Others offered were electronic tablets or computers, sign language and other variety of visuals.
- What risk factors are associated with children developing communication disorders? (check all that apply)
- What eligibility criteria or tool do you use for evaluation of young children?
Of the 22 SLPs who completed the survey seventy-two percent reported using the Goldman Fristoe Test of Articulation, Preschool Language Scale or some other form of evaluation too to assess their students. Eighty-one percent report using the Clinical Evaluation of Language tool and thirteen percent use the Boehm Test of Basic Concepts.
- What percentage of children on your current caseload have other disabilities in addition to SLI?
Forty-five percent of those SLPs reported that 51-75% of children served have other
disabilities in addition to SLI.
- List any other relevant health/medical information that leads to SLI?
SLPs who completed the survey reported that many other factors can play a role in a child developing SLI such as, intermittent hearing loss, Fetal Alcohol Syndrome, Autism, Attention Deficit Hyperactivity Disorder, Selective Mutism, limited exposure to language-rich environments, limited exposure to texts, Cleft Palate, drug addiction during utero, premature birth, chronic ear infections, abuse/neglect and anxiety.
Discussion
This study explored the experiences from current SLPs across Ohio. The purpose was to gain insight on materials and activities available to improve communication skills in children. Information on supports or interventions in the classrooms as well as for the parent/guardian in the home are also explored. While conducting this research data was discovered relating to diagnosis, risk factors, prevalence and risk for later literacy learning difficulties.
Similarities and Differences between Results and Previous Research
This study confirmed that early detection and intervention is key for success in a child with communication delays. The results of this study as well as others mentioned agree that family history, child illness and other disabilities play a primary role in a child developing communication delays. Pediatric clinicians as well as parents/guardians play a central role in the detection, evaluation and management of child who have these delays and disorders. Feldman (2012), points out that it remains unclear whether early language and speech therapy can prevent or reduce subsequent reading problems. Children who have reading disorders are likely to have difficulties manipulating speech sounds, such as subtracting a syllable or sound from a word. In a study by Jennifer Moore (1999), there was no evidence of a significant relationship between social skills of preschool children and their language delay. This was said to possibly be due to the restricted range of functioning in the children who participated.
Practical Recommendations
According to Paul and Roth (2011), research has demonstrated that Early Intervention (EI) services can prevent the impact of various risk factors and impairments in children. In some cases EI services can alter a child’s development trajectory; in others, EI services can prevent secondary complications or reduce the extent of the child’s disability. Yet, issues arise in allotting scarce EI resources. For children with identifiable medical conditions such as Downs Syndrome or deafness, EI services are generally mandated. However, access to EI services may be less available for many other children, including children who present with risk factors in the absence of documented delays (such as infant siblings of young children with Autism) as well as those who demonstrate relatively circumscribed delays in language in the absence of cognitive, motor and sensory delays. Availability of services varies from state to state. Some states require evidence of significant delays in several areas of development before a child can be determined eligible for services (Spiker et al., 2000).
Research Limitations
Of the one-hundred speech language pathologists who were contacted to complete the survey a total of twenty-two were able to do so. This is due to him/her not being licensed in the state of Ohio or a lack of interest in completing. Other limitations might include the lack of background knowledge about the 22 SLPs who participated such as their age, district or facility in which they practice, years of experience, etc.
In survey question #3 it is assumed that Autism Spectrum Disorder would be included in the “other” answer choice since it was not a choice. In question #4 it is unknown what other types of supports aside from those listed are provided from SLPs. This is key for parental involvement and student success in the classroom. The researcher should have included space for participants to write in other materials, activities or interventions that are helpful. In question #5 it is unknown what other factors are included in the fifty-four percent who answered “other.” The researcher should have allotted writing space to include a description from participants.
Conclusion
It is to be hoped that emerging research will, in the near future, assist SLPs in dealing with the wide range of issues and dilemmas faced in providing the highest quality services and in computing the cost-benefit relations that arise in EI practice (Paul and Roth, 2011).
References
ASHA.org (2016). Speech-Language Impairments Rank Frist, Second Highest by Age. The ASHA Leader, 21 (13).
Boyse, K., R.N. (2012). Speech and Language Delay and Disorder. Retrieved February 5, 2017, from http://www.med.umich.edu/yourchild/topics/speech.htm.
Carson, C., Klee, T., Carson, D., & Hine, L. (2003). Phonological profiles of 2-year-olds with delayed development: Predicting critical outcomes at age 3. American Journal of Speech-Language Pathology, 12, 28-39
Center for Parent Information and Resources (2015). Speech and Language Impairments. Retrieved February 5, 2017, from http://www.parentcenterhub.org/repository/speechlanguage/
Dale , P., Price, T. Bishop, D. & Plomin, R. (2003). Outcomes of early language delay: I Predicting persistent and transient language difficulties at 3 and 4 years. Journal of Speech, Language, and Hearing Research, 46, 544-560.
Dosman, C.F., Andrews, D., & Goulden, K. J. (2012). Evidence-based milestone ages as a framework for developmental surveillance. Pediatrics Child Health, 17(10), 516-568.
Feldman, H. M., (2005). Evaluation and management of Language and Speech Disorders in Preschool Children. American Academy of Pediatrics, Pediatrics in Review, 26 (4).
Feldman, H. M., (2012). Evaluation and Management of Language and Speech Disorders in Preschool Children. American Academy of Pediatrics, Pediatrics in Review, 26, 131-140.
Fenson, L. Marchman, V., Thal, D., Dale, P., Reznick, S., & Bates, E. (2007). The MacArthur-Bates Communicative Development Inventories. Baltimore, MD: Brookes.
Gillion, G. T. & McNeill, B. C. (2007). Integrated Phonological Awareness: An Intervention Program for Preschool Children with Speech-Language Impairment. Canterbury: University of Canterbury.
Hadley, P., & Holt, J. (2006). Individual differences in the onset of tense marketing: A growth curve analysis. Journal of Speech, Language and Hearing Research, 49, 984-1000.
IDEA. (2004). Individuals with Disabilities Education Act. Retrieved July 31, 2017, from http://idea.ed.gov/explore/home.html
Lancaster, G., (2008). Developing Speech and Language Skills. London: Routledge.
Law, J. ,Boyle, J., Harris, F., Harkness, A., & Nye, C. (2000). Prevalence and natural history of primary speech and language delay: Findings from a systematic review of the literature. International Journal of Language and Communication Disorders, 35, 165-188.
Lousada, M., Luis, M.. Jesus, T., Hall, A., and Joffe, V (2014). Intelligibility as a clinical outcome measure following intervention with children with phonologically based speech-sound disorders. International Journal of Language and Communication Disorders, 49, 5, 584-601.
Moore, Jennifer (1999). The relationship between speech/language and social skills in preschool children with developmental delays. Washington, DC: ERIC Clearinghouse.
Ohio Department of Education (2017). Birth through Kindergarten Entry – Learning and Development Standards. Retrieved July 2, 2017 from http://education.ohio.gov/Topics/Early-Learning/Early-Learning-Content-Standards/Birth-Through-Pre_K-Learning-and-Development-Stand
Oxford. Definition of language. (2017). Retrieved May 22, 2017, from https://en.oxforddictionaries.com/definition/language
Paul, R (1996). Clinical implications of the natural history of slow expressive language development. American Journal of Speech-Language Pathology, 5, 5-30.
Paul, R., & Jennings , P. (1992). Phonological behavior in normal and late talking toddlers. Journal of Speech and Hearing Research, 35, 99-107
Paul, R., & Riback, M. (1993). Sentence structure development in late talkers. Poster session present at the Symposium for Research in Child Language Disorders, Madison, WI.
Paul, R., & Roth, F. (2011). Characterizing and Predicting Outcomes of Communication Delays in Infants and Toddlers: Implications for Clinical Practice. Language, Speech and Hearing Services in Schools, 42, 331-340.
Rescorla, L., Dahlsgaard, K., & Roberts, J. (2000). Late-talking toddlers: MLU and IPSyn outcomes at 3;0 and 4;0. Journal of Child Language, 52, 16-30.
Rescorla, L., & Lee, E. C. (2000). Language impairments in young children. In T. Layton & L. Watson (Eds.), Handbook of early language impairment in children (pp. 1-38). New York, NY: Delmar.
Rescorla, L., & Ratner, N. (1996). Phonetic profiles in toddlers with specific expressive language impairment. Journal of Speech and Hearing Research, 39, 153-166
Rice, M., Taylor, C., & Zubrick, S. (2008). Language outcomes of 7-year-old children with or without a history of late language emergence at 24 months. Journal of Speech, Language and Hearing Research, 51, 394-407.
Roos, E., & Weismer, S. (2008). Language outcomes of late talking toddlers. Perspectives in Language Learning Disorders, 15, 119-126.
Spiker, D., Hebbeler, K., Wagner, M., Cameto, R., & McKenna, P. (2000). A framework for describing variations in state early intervention systems. Topics in Early Childhood Special Education, 20, 195-207.
Squires, A. & Hastings, M. (2002). Rehabilitation of the Older Person: A Handbook for the Interdisciplinary Team. (3rd ed.). Cheltenham, UK: Nelson Thornes, Ltd.
Thal, D., Oroz, M., & McCaw, V. (1995). Phonological and lexical development in normal and late-talking toddlers. Applied Psycholinguistics, 16, 407-424.
Thal, D., Reilly, J., Seibert, L., Jeffries, R., & Fenson, J. (2004). Language development in children at risk for language impairment: Cross-population comparisons. Brain and Language, 88, 167-179.
The Hanen Centre (2016). Communication Development in Children with Language Delays. Retrieved February 5, 2017, from http://www.hanen.org/About-Us/What-We-Do/Early-Childhood-Language-Delays.aspx
Whitehurst, G. J., & Fischel, J. E. (1994). Early development language delay: What, if anything, should a clinician do about it? Journal of Child Psychology and Psychiatry, 35, 613-648.
Zubrick, S., Taylor, C., Rice, M., & Slegers, D. (2007). Late language emergence at 24 months: An epidemiological study of prevalence, predictors and covariates. Journal of Speech, Language, and Hearing Research, 50, 1562-1592.
Appendix A
- Are you a Licensed Speech Language Pathologist in the State of Ohio?
- Yes – 100%
- No
- What age(s) of children do you serve? (check all that apply)
- What common risk factors do you see associated with speech-language impairments? (check all that apply).
- What types of supports can/do you offer teachers to better serve children in the classroom with SLI?
All 22 participants reported offering visual aids as a support for teachers. Eighty-one percent reported offering assistive technology as a support in the classroom. Less than fifty percent reported other types of support aids. Others offered were electronic tablets or computers, sign language and other variety of visuals.
- What risk factors are associated with children developing communication disorders? (check all that apply)
- What eligibility criteria or tool do you use for evaluation of young children?
Of the 22 SLPs who completed the survey seventy-two percent reported using the Goldman Fristoe Test of Articulation, Preschool Language Scale or some other form of evaluation too to assess their students. Eighty-one percent report using the Clinical Evaluation of Language tool and thirteen percent use the Boehm Test of Basic Concepts.
- What percentage of children on your current caseload have other disabilities in addition to SLI?
Forty-five percent of those SLPs reported that 51-75% of children served have other disabilities in addition to SLI.
- List any other relevant health/medical information that leads to SLI?
SLPs who completed the survey reported that many other factors play a role in a child developing SLI such as, intermittent hearing loss, Fetal Alcohol Syndrome, Autism, Attention Deficit Hyperactivity Disorder, Selective Mutism, limited exposure to language-rich environments, limited exposure to texts, Cleft Palate, drug addiction during utero, premature birth, chronic ear infections, abuse/neglect and anxiety.
Appendix B
Ohio University Adult Consent Form with Signature
Title of Research: Speech Language Pathologist practices
Researcher: Monica Gwilym, Early Childhood Intervention Specialist
You are being asked to participate in research. For you to be able to decide whether you want to participate in this project you should understand what the project is about, as well as possible risks and benefits in order to make an informed decision. This process is known as informed consent. This form describes the purpose, procedures, possible benefits and risks. It also explains how your personal information will be used and protected. Once you have read this form and you questions about the study are answered, you will be asked to sign it. This will also your participation in this study. You should receive a copy of this document to take with you.
Explanation of Study
For parents of children with speech-language impairments (SLI) the assumption that a child may grow out of their speech delay and be on target when compared to other children their age, is not always true. This study explores the services and supports reported to be available by current Speech Language Pathologists (SLPs) across Ohio. I will use this information to describe children served, the likelihood of later literacy learning difficulties, as well as strategies that early childhood special education (ECSE) teachers can use with children with SLI.
If you agree to participate you will be asked to complete a survey. Surveys will be sent to SLPs who serve children ages 3-5 who have 1) a speech language impairment, 2) a disability other than Speech Language Impairment and who have speech/language needs, and 3) no disability or delay but who have speech/language needs. Respondents will describe the materials and activities made available to children. Respondents will describe the children’s communication behaviors at home as well as any medical/health information that is relevant. Respondents will give information on their own practices as well as classroom supports.
Risk Discomforts
No risks or discomforts are anticipated.
Benefits
Teachers in the professional community may learn helpful interventions they can use in the classroom to support students with communication delays. Teachers, participants and others may learn the importance of early detection and therapy services in early years.
Confidentiality and Records
While every effort will be made to keep your student-related information confidential, there may be circumstances where this information must be shared with:
- Federal agencies, for example the Office of Human Research Protections, whose responsibility is to protect human subjects in research;
- Representatives of Ohio University (OU), including the Institutional Review Board, a committee that oversees the research at OU.
By signing below you are agreeing that:
- You will read this consent form (or it has been read to you) and have been given the opportunity to ask questions and have them answered;
- You have been informed of potential risks and they have been explained to your satisfaction;
- You understand Ohio University has no funds set aside for any injuries you might receive as a result of participating in this study;
- You are 18 years of age or older;
- Your participation in this research is completely voluntary;
- You may leave the study at any time;
- If you decide to stop participating in the study, there will be no penalty to you and you will not lose any benefits to which you are otherwise entitled.
Signature _______________________________________________ Date ________________
Printed name ____________________________________________________
Version Date: 03/27/2017
Cite This Work
To export a reference to this article please select a referencing stye below:
Related Services
View all


Related Content
All TagsContent relating to: "Learning"
Learning is the process of acquiring knowledge through being taught, independent studying and experiences. Different people learn in different ways, with techniques suited to each individual learning style.
Related Articles

DMCA / Removal Request
If you are the original writer of this dissertation and no longer wish to have your work published on the UKDiss.com website then please: