Critical Analysis of Early Interventions for Autism Spectrum Disorder
Info: 9410 words (38 pages) Dissertation
Published: 10th Dec 2019
Introduction to ASD:
Autism Spectrum Disorder is defined as a range of conditions characterized by challenges with social skills, repetitive behaviors, speech and non-verbal communication.[1] Autism Spectrum Disorder can be diagnosed as early as 18 months, with most cases being diagnosed between 2 and 3 years of age. The types of symptoms can be classified into different categories, mainly behavior, speech, language and interaction with others. For children below 18 months of age, some symptoms include the lack of vocal sounds.[2] For children above 18 months of age, some symptoms that indicate ASD include lack of non-verbal communication with peers, delayed speech development, difficulty in social interactions. In terms of interaction with others, children with Autism Spectrum Disorder tend to have difficulties maintaining eye contact and involving the use of body language and gestures in their interaction with others. They prefer to play by themselves, with little interest in playing and interacting with other people, especially peers. In terms of speech and language, children with ASD often have a reduced vocabulary, preferring to communicate using repetition of short, single words. With regards to their behavior, children with ASD tend to repeat certain movements such as flicking their fingers and prefer to have a familiar playing routine, often getting upset if their routines are altered. They tend to have uncommon interests involving their five senses and have a lack of awareness of personal space.[3] Since the beginning of 1900s, many extensive research has been done to find out the causes of Autism Spectrum Disorder. Unfortunately, due to the complexity of the condition, the exact cause has yet to be discovered. However, most researchers believe that genetic make-up inherited from previous generations may lead one to be more vulnerable to developing ASD. In fact, research has shown that the likelihood of one developing ASD is increased if there are cases of ASD in the family. Also, some researchers believe that environmental conditions play a part in affecting a child’s vulnerability to ASD, for example, exposure to medication and alcohol during pregnancy. [4]However, these are based on some researchers’ hypothesis with little evidence the back up their claims, concrete evidence has yet to be discovered due to lack of funding dedicated to this domain of research. According to NHS, it is estimated that about 1 in every 100 people in the United Kingdom suffers from Autism Spectrum Disorder, with about 700,000 people on the Autism Spectrum, this value does not include people with ASD that are not diagnosed. [5]According to Autism Speaks, tens of millions are affected by ASD worldwide. [6]These statistics shows us that many families in the UK and around the world are affected by ASD, and therefore it is a pressing issue that needs to be tackled.
Why Early Intervention?
With Autism Spectrum Disorder being so prevalent in the world today, it is important to access its impacts on the rest of the human population and how it can be avoided. Unfortunately, there is not one specific cure that can eradicate ASD forever, however, there are many interventions that have been invented to help minimize the effects of ASD.[7] Unarguably, it is extremely important for intervention to begin as early as possible. Research has shown that early intervention has a positive impact on a child’s development with improved outcomes for intelligence, increased social interaction skills, minimizing the negative effects of ASD in their adulthood.[8] Early intervention is shown to have improved outcomes in the long-run, with maximized learning potential. This is due to the children being more impressionable at a younger age of below 4 years. Research has shown that the neural plasticity of the brain is maximal in the first 4 years of life and starts to reduce thereafter.[9] Therefore, below the age of 4, the human brain is the most malleable and thus will be able to retain more skills taught, such as communication and interaction skills. Also, starting intervention earlier would indicate longer years of positive reinforcing, addressing the child’s difficulties with behavior typically accepted by the norm, ensuring quick and positive changes.[10] In this essay, I will be defining early intervention as intervention that is implemented from the age of below 4 years old.
History of Autism Interventions:
In the 21st Century, the different types of intervention methods can be classified into two main categories. [11]One set of interventions focusses on specific interventions designed to produce certain behavioral or developmental outcomes for children with ASD. Such examples would include discrete trial teaching, peer mediated interventions, prompting. Typically, these types of interventions are applied for short periods of time, hoping to promote a specific change in targeted behavior. The second set of intervention is formed by comprehensive treatments. Comprehensive treatments are designed with the intent of achieving a broader, wider learning and developmental impact on the main characteristics of ASD. Typically, these types of interventions are applied for prolonged periods of time and they tend to focus on a range of target behaviors, instead of specific ones. Such examples include the TEACCH. [12]The type of interventions I shall be focusing on in this essay is comprehensive treatments.
In this essay, I will be attempting to analyze each intervention method holistically and based on the core principles of each intervention method. The criteria for topics for analyzation of the intervention methods are listed below:
- Treatment Integrity
- Core principles and values
- Treatment Characteristics
- Time frame
- Family Involvement
- Agents
- Effectiveness
Applied Behavior Analysis:
One of the most commonly applied interventions is the Applied Behavior Analysis (ABA).[13]
Applied behavior analysis is a theory which was developed by Ivar Lovaas in the early 1960s, and even after more than 50 years later, it is still one of the commonly used techniques.[14] “Behavior” refers to one’s actions, “Analysis” refers to a detailed examination. In this context, “behavior analysis” refers to the detailed investigation of one’s actions. Behavior analysis involves the use of a scientific approach to understand behavior and the different factors that play a role in affecting it, such as physical and social factors. In relation to Autism Spectrum Disorder, behavior analysis focuses on the principles that explain how learning takes place. [15]Some of the core principles include positive reinforcement and prompting. Applied Behavior Analysis (ABA) is the use of behavior analysis in hopes of achieving positive and impactful change in one’s behavior. In the 21st century, the majority of behavioral interventions are based on ABA.
Principles of ABA:
According to the BACB[16], there are four core principles of ABA.
- Assessment and observation of conditions should be done via observing how the environment affects the child’s behavior.
- Emphasis should be placed on attempting to understand the context of the behavior and the behavior’s value to the individual, the family, and the community.
- Principles and procedures of behavior analysis should be accurately carried out, ensuring the child’s health, independence and quality of life are improved.
- There should be consistent, ongoing, objective assessment and data analysis to aid decision making and alteration of treatment plans.
In ABA intervention, emphasis is placed on the following items:
- Ability to adapt to different situations and self-care skills
- Cognitive functioning
- Community participation
- Coping and tolerance skills
- Family relationships
- Language and communication
- Reductions of inappropriate behaviors
- Independence
- Self-management
- Social relationships
- Vocational skills
- Positive reinforcement
These components have been selected as a result of detailed research, with the conclusion that the above components, if mastered, will help a child with ASD to integrate into our society and reduce the effects of ASD.
One of the areas ABA emphasis in is positive reinforcement. Positive reinforcement is defined as the process of encouraging and establishing a pattern of behavior by offering some form of reward when that particular desired behavior is exhibited.[17] An example of positive reinforcement in ABA would be to reward the individual with ASD a token or a prize when a particular behavior is observed. This teaches the individual that by doing the right thing, acting a certain way, he will be rewarded. This increases the chances of the individual exhibiting the same behavior. A research study investigating the effectiveness of positive reinforcement in ABA was done.[18] 3 individuals were given interventions which took the positive reinforcement approach. For each correct response, the individuals were given a small amount of edible treat or received access to an item for 1 min. For every wrong response, corrective feedback was given. Results showed that there was a general improvement observed in the accuracy of generalization tasks. This proves that positive reinforcement does work in the case of ABA. This might be because positive reinforcement stimulates the individual to remember each time he was rewarded upon good behavior and attempt to display it more often to earn more rewards. This will ensure that the areas taught in contact time with agents will be reinforced in the individuals’ mindsets and they will display positive behavior more often. This increases the effectiveness of the intervention.
Treatment Integrity:
Treatment integrity refers to how accurate is the implementation of the intervention and how closely the practice follows the treatment plan. A lack of treatment integrity means the failure to follow closely to treatment guidelines and plans. As a result of failure to control treatment integrity, there are many negative consequences that can occur.[19]
According to the data released on child studies published in the Journal of Applied Behavior Analysis between 1980 and 2005, only 71 out of the 311 child studies systematically measured and reported levels of treatment integrity. [20][21]This is shown in figures 1 and 2 below.

Figure 1: Number of studies in Which Treatment Integrity Was Measured and Reported (by year)
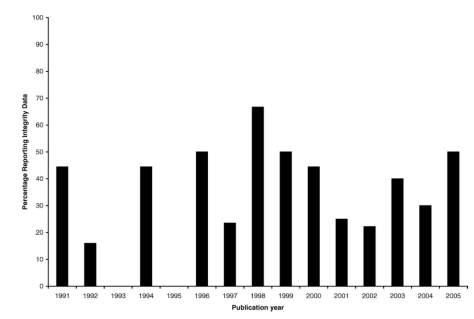
Figure 2: Percentage of JABA school-based studies reporting treatment integrity data by year (1991 to 2005)
The failure to report data on the treatment integrity for more than 75% of the child studies reported by JABA indicates a discrepancy in the treatment integrity due to the lack of control over treatment integrity. With a lack of valid data, it would be impossible to determine whether the Applied Behavior Analysis intervention program was conducted following guidelines closely and if not how would treatment effects be affected. As such, this highlights the possibility of inaccurate measurement of effectiveness in the intervention program. This will result in a decrease in confidence in the ability of the intervention in helping children with Autism Spectrum Disorder their development. However, it is important to note that out of those who measured and recorded treatment integrity values, the majority of studies bad reported procedural fidelity of 90% or greater. This high level of procedural fidelity indicates high levels of treatment integrity. This tells us that the procedures and characteristics of ABA are effective in ensuring a generally high treatment integrity, but may have difficulties ensuring the same level of treatment integrity for all the children experiencing the intervention.
Agents:
One of the components that affects treatment integrity is agent competence. With regards to Applied Behavior Analysis, emphasis has been placed on the training of agents as an attempt to increase agent competence.[22] A study done focused on evaluating the training of agents in ABA. The training participants undergo to get certified as an Applied Behavior Analysis Treatment agent is standardized with only a few minor differences between approaches. Generally, the curriculum will cover three modules. The first module will be Basic Learning Principles, covering aspects such as defining behavior, positive and negative reinforcement, observation, measurement, data collection, functional assessment. The second module is based on instructional strategies, focusing on aspects such as discrete trial instruction, incidental teaching and task analysis. The last module focuses on prompting and prompt-fading methods, with emphasis placed on physical prompting, verbal prompting and methods to withdraw prompts. Six group of participants had received standardized training on basic ABA principles and theory.[23] Before the training, the participants were given an “Assessment of Knowledge (AOK)” test. The test had 10 multiple questions. After doing the pre-training test, the participants were then administered ABA training. They were given 2 sessions of training, with the first session being 2.5 – 3 hours focusing on module 1 and the second session being 2 hours focusing on modules 2 and 3. Results indicated that for module 1, there was an increase of 34.3% on average percentage scores from 52% to 86.3% before and after the training. For module 2, there was an increase of 24.9% on average percentage scores from 64% to 88.9%. For module 3, there was an increases of 23.8% on average percentage scores from 64% to 87.8%. [24]This gives indication that the training sessions were effective in ensuring the participants’ knowledge on the 3 modules were expanded. This shows us that the training agents undergo to be certified in conducting the ABA intervention does indeed fulfill its criteria of ensuring the agents are well equipped with basic ABA principles. This is a positive indication that the agents are competent in their knowledge. With agents being more competent, it increases the confidence in ensuring the agents carry out the interventions accurately according to its basic principles and reduces the risk of lack of treatment adherence due to lack of knowledge. This helps to promote treatment integrity, allowing the intended effects of the intervention to occur.
Also, according to the BACB, a behavior analyst agent must undergo supervision by a BACB certified agent for a minimum of 5% of the hours spent conducting the applied behavior analytic services on children with ASD. This helps to ensure agents undergo close supervision and thus the likelihood of the agents disregarding treatment integrity decreases. [25]This helps to ensure proper guidelines are met and the children undergoing the programs are not being short-changed. This regulation also helps to ensure the treatment program is being conducted accurately, allowing for intended outcomes to occur.
According to the BACB, with the conduction of ABA intervention, parents and care-givers are required to undergo training and consultation to help facilitate and reinforce techniques and procedures outside of treatment hours. The reasons for this approach were that caregivers and family members have more contact hours with the child and thus have the ability to develop a stronger relationship with the child. This helps the child to learn in an environment that is comfortable and promote healthy learning habits. The children are comfortable with their parents and thus it encourages them to have positive improvement towards the intervention program.
Time frame of the Intervention Program:
Another subject that may increase the risk of lack of treatment integrity is the time frame of the intervention program.[26] An increased required time frame may be the catalyst for not following guidelines that might be deemed long-winded and troublesome. This will affect the treatment integrity and eventually the effectiveness of the intervention. According to the practice guidelines released by the Behavior Analyst Certification Board, services will be suspended when the child has achieved treatment goals, when the child no longer falls under the criteria for ASD, when the child does not indicate any progress and development towards the goals set for successive periods or when the parents or guardians indicate their interest to suspend services. This essentially means the time frame for the intervention program defers for each child, depending on the progress and the severity of the conditions. In the manual of guidelines, the board also highlights that on average, treatment involves between 30 and 40 hours of direct one to one treatment between the agent and the child. [27]A research comparing the effectiveness of high intensity and low intensity ABA treatment with children between the ages of 2.6 and 4 years old was done in 2007. They defined high intensity as programs offering training of between 20 and 40 hours per week and low intensity as programs offering training of between 10 and 20 hours per week. [28]The characteristics of the high and low intensity interventions are illustrated in the table below.
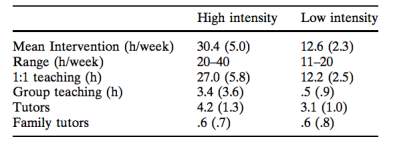
Figure 3: Table showing characteristics of high and low intensity interventions
Results indicated that participants that underwent high intensity ABA intervention on average had produced better results, indicating an increase in effectiveness. The guidelines for ABA being based on high intensity hours between 30 and 40 hours helps to ensure that the children receiving this particular intervention program will not be negatively impacted due to lack of treatment hours and will be guided to ensure the best outcomes. [29]
Effectiveness of the intervention Program:
I will be evaluating effectiveness based on how well did the intervention address the core deficits in autism. Based on 11 research studies done on the effectiveness of ABA, results had shown that individuals who underwent ABA intervention generally outperformed other individuals undergoing different treatments. [30]This is supported by a general increase in non-verbal IQ, receptive, expressive language and other areas such as adaptive behavior, communication, daily living skills and more. Across the 11 research studies, there were 334 children involved. The individuals’ average age ranged from 33.56 months to 65.68 months, with an average IQ ranging from 27.52 to 76.53. The experimental group consisted of individuals who underwent high intensive intervention for between a time period of 10 months and 2 years. There was a control group which involved less intensive interventions with different treatment approaches. As mentioned earlier, results had indicated positive effects with the experimental group, indicating the effectiveness of the intervention. The experimental group showed an improvement of 11.98 points more than in the control groups in terms of IQ. Average increases in receptive and expressive language by 13.94 and 15.21 points respectively was observed. Improvement in other areas of interest such social interaction was also observed. The results of the 11 research studies on early intervention in children using ABA has proved that ABA is indeed effective, as it can improve the core deficits in autism. The general results of 8 out of 11 studies are included in the table below.[31]
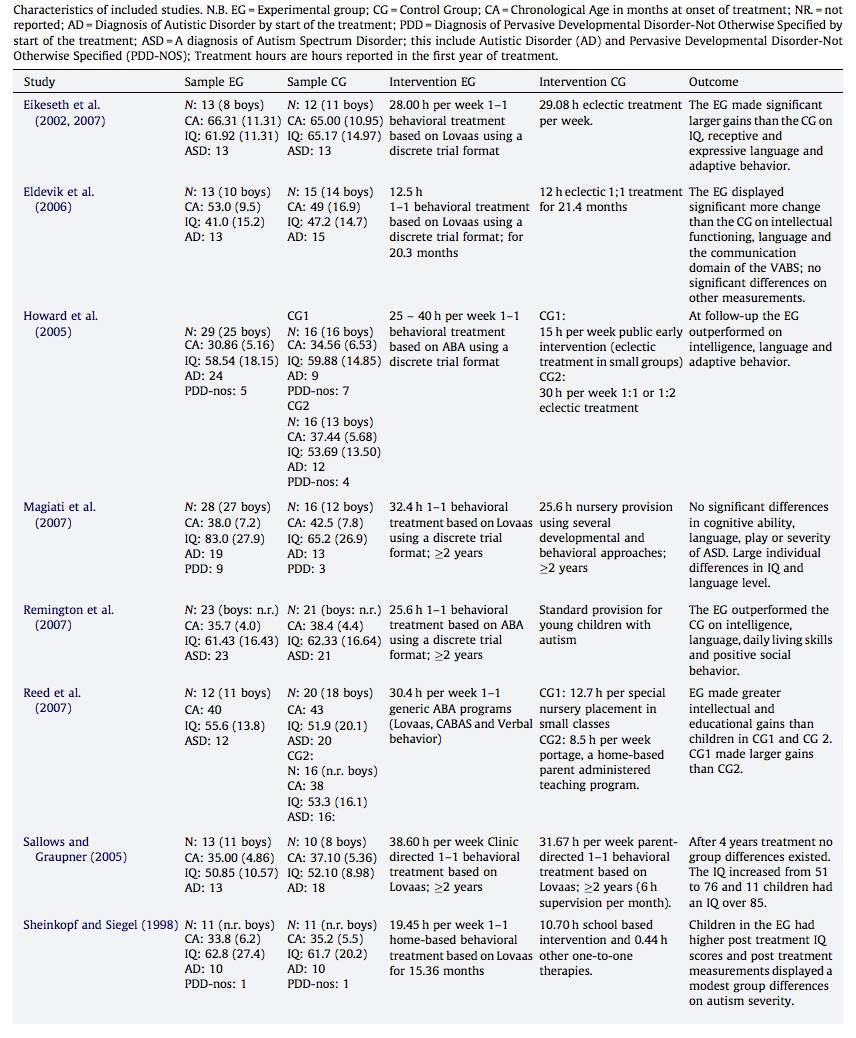
Figure 3: Table showing results of 8 early intervention using ABA research studies
TEACCH (Treatment and Education of Autistic and Communication related handicapped children):
Another commonly applied intervention for children with Autism Spectrum Disorder is TEACCH. TEACCH was invented in 1972 by the Department of Psychiatry, University of North Carolina, initially beginning as a child research project. [32]TEACCH is a school-based intervention. Some of the core characteristics of TEACCH include the ability to understand the effects of autism on individuals and thereby using assessments to plan structured treatment programs designed around the individuals. The approach TEACCH emphasizes on is the use of structured TEACCHing.[33] According to the University of North Carolina, structure TEACChing is to recognize and acknowledge the strengths and challenges faced by individuals, and using their profiles to provide support to address each individuals’ needs, with the goal of helping them integrate back into the society. Also, the purpose of structured TEACCHing is not to cure autism but to help individuals learn how to lead independent lives, integrating back into the society. The core values of TEACCH are:[34]
- Teaching – To share knowledge of ASD and increase the skill level of others through education and demonstration
- Exapanding – To expand their own knowledge, ensuring the highest quality service is being offered
- Appreciating – Understanding and appreciating the unique strengths of the individuals
- Collaborating and Cooperating – Collaborating with colleagues, individuals and their families
- Holistic – Emphasis is placed on the importance of looking at the whole person, their families and communities throughout the lifespan
Core characteristics:
As mentioned earlier, the approach taken by TEACCH is through structured teaching, or commonly referred to as structured TEACCHing. Structured teaching places emphasis on principles and intervention strategies that are based on the individuals’ needs, skills and interests. It places strong emphasis on developing the individual’s current skill set as well as expanding their knowledge and learning different skills. It can be used to target any form of lacking with regards to behavioral, academic, communication and more.
TEACCH emphasizes on the use of visual aids which can be adapted for different age groups to help tackle behavioral and educational challenges. Visual aids include visual schedules, which highlight clearly to the individuals to understand the process and what will be coming next. This eliminates the consequence of lack of understanding coming from the individual due to having to rely on other sources of communication such as speaking. Also, the use of visual schedules will allow the individual to learn how to take responsibility over the intervention program, promoting independence. This is a skill which is very important as it will allow an easier transition back into the society for the individuals.
Another type of visual support used is the use of visual cues which may involve the use of objects, photographs, drawings and more, depending on the individual. These cues are used to ensure individuals understand what stage they are at and what will be happening from this stage on. Also, these visual cues can be used during the teaching itself, using them to represent a certain activity or idea.
According to various studies done, children with ASD tend to be visual learners, often demonstrating difficulties in processing information presented in verbal format, for example language and face-to-face communication. Visual learners refer to individuals who learn best using the format of visual items, such as words and pictures. By placing emphasis by using visual supports, TEACCH program aims to help tackle problems by adjusting treatment plans to best suit each individual with ASD. By implementing this, the individuals with ASD will learn in the most effective way for themselves.
TEACCH also places strong emphasis on utilizing the strengths each individual has and to help combated other areas that the individual might be lacking in. For example, using the individual’s strength to motivate them to work on other areas. In the beginning of the process, agents will need to use the information gathered on the individual to create a treatment plan designed around the individual’s needs, strengths, unique traits, making a very individualized plan.
In order to combat the issue about individuals’ frequent lack of communication skills, TEACCH uses visual systems to pave a solution for the individual to express their opinions and feelings based on the visual items they have. This serves as the foundation for communication skills to be expanded. By teaching the individuals to express themselves in a way that is most comfortable for them, it enables the individual to develop the understanding in communicating with others.
Also, TEACCH interventions places emphasis on imparting more than just social and communication skills to individuals but also addressing other skills that will be useful in allowing a smooth transition into society again such as writing, mathematics, academic skills and more.
The approach TEACCH has taken, through the implementation of structured teaching, has resulted in individuals understanding clearly what is the next step in the process and how to go about doing it. Having this clear structure is proven to be extremely useful for the individuals, also giving them the opportunity to take charge of their own life and condition. This gives them an opportunity to practice responsibility, a very important skill needed to survive in this society without any help.
Agent Competence:
According to the Inventors of TEACCH program, the criteria to be certified to practice TEACCH as a TEACCH certified practitioner is listed below:[35]
- Participate in a Five-Day University of North Carolina TEACCH Autism Program training led by TEACCH staff
- Complete s TEACCH Beyond the Basics: Advanced Applications of TEACCH Principles and Practices Seminar
- Implement one year of TEACCH principles in one’s work setting
- Passing an on-line written and a Skype oral examination
Also, re-certification is required every 3 years, including attending 16 contact hours of continuing education activities in ASD. This shows that the TEACCH program acknowledges that agent competence is a very important factor in ensuring a correctly carried out intervention and promoting the effectiveness of an intervention. By ensuring certified practitioners undergo re-certification every 3 years allows practitioners to revise basic TEACCH principles and correct any previous wrong principles and approaches. Re-certification also helps the TEACCH programmers assess practitioners’ competence and pick out practitioners with lacking skills and train them to equip them in this particular lacking area. This helps to prevent continuous wrong application of TEACCH principles and ensure that the children undergoing the intervention program are not short-changed in any way and gearing intended treatment outcomes.
Family involvement:
Family involvement is one of the fundamental principles of TEACCH. Parents are viewed as experts on their children, information that is gathered from parents’ observations together with agent’s observations will be used to provide a better diagnose and design a more individualized treatment plan. Studies supports the use of TEACCH interventions in home and school, citing these 2 environments as most natural environments for the children and thus it would be extremely useful to conduct the interventions in these comfortable environments as the children will tend to be more impressionable and will accept teachings and learn new things. Also, studies have proven that parent training can possibly contribute to reducing parents’ depressive symptoms, encouraging positive family interactions between parent, siblings and the individual with ASD. [36]
Effectiveness:
I will be evaluating effectiveness based on how well did the intervention address the core deficits in autism. Based on 13 research studies done on TEACCH intervention, results showed a slight improvement in certain areas such as motor skills, adaptive behaviors, language and cognition and more. Over the 13 research studies, 172 individuals with ASD had received TEACCH intervention. The intensity of the intervention varied from 1.5 hours to 30 hours per week.[37] They were compared against a control group, which did not receive TEACCH treatment, instead receiving normal treatment or were placed in normal schools. Results had shown improvements in motor skills, adaptive behaviors and more. However, the improvement shown was minimal and were comparable to those in the control group. This highlights the possibility that TEACCH treatment does indeed target the core deficits in autism, however since the improvement made is minimal and increases at a slow pace, the ability of the treatment program to effectively and efficiently improve the characteristics of ASD is low. However, based on a longitudinal study conducted on 34 children with autism on the effectiveness of TEACCH, results indicated that significantly more improvement in perception, fine motor and gross motor skills and more was observed in individuals that received TEACCH treatment.[38] On comparison with the various studies, I realized that the intensity of the TEACCH treatment varied in the studies. In the earlier studies, the children were exposed to on average about 14 hours of treatment per week for on average 4 months. However, in the latter study, children were exposed to on average about 50 hours of treatment per week for 12 months. This difference in intensity might have been one of the reasons the treatment outcomes were so different. With more time invested into the treatment, the agents will have more time to teach the individuals and ensure individuals understand before moving on. As mentioned earlier, research on the intensities of interventions indicated that interventions with higher intensities tend to be more effective.[39] Therefore, I believe that while TEACCH is effective in treating the core deficits of ASD, a huge aspect of its effectiveness is reliable on the intensity of the treatment.
What makes an effective intervention?
Based on the analysis of the two widely accepted interventions mentioned above, I have made my own opinion as to what makes an effective intervention. I will be defining effective intervention as an intervention which manages to fulfill their intended outcome. Intended outcomes of the interventions should ensure improvement of the challenges faced by individuals with ASD with the intention that these individuals will be ready to integrate back into society after undergoing the treatment.
Treatment Integrity:
Firstly, in order to ensure that solutions produce the intended results, treatment integrity must be placed as priority, ensuring that the integrity of the treatment plan is not jeopardized. Treatment integrity refers to how accurate is the implementation of the intervention and how closely the practice follows the treatment plan. A lack of treatment integrity means the failure to follow closely to treatment guidelines and plans. As a result of failure to control treatment integrity, there are many negative consequences that can occur. Firstly, the effectiveness of the intervention program cannot be realistically evaluated and thus will have an impact on the confidence in a particular intervention. Secondly, failure to control treatment integrity may lead to a reduction of improvement among the children with Autism Spectrum Disorder. Another consequence that may occur is the potential catalyst for legal problems regarding ethical concerns.[40] Therefore, it is extremely important that treatment integrity is maintained throughout the implementation of the intervention. An effective intervention should take into account factors to ensure treatment integrity is maintained throughout the entire intervention process, from diagnosing to termination.
Agent competence:
Another factor that affects the effectiveness of an intervention is the ability of the agents. Many different agents conduct the same intervention programs. The agent competence can have an effect on the way the program is conducted and may have an impact on the results and the effectiveness of the intervention.[41] For example, an agent who is more competent might be able to follow closely to guidelines and this might have a positive impact on the results as compared to an agent who is less competent, failing to comply to instructions and as a result negatively affecting the development of a child with Autism Spectrum disorder. Both interventions mentioned above, ABA and TEACCH, has some sort of prevention mechanism placed to ensure that the agents conducting the sessions are competent and by ensuring they have a detailed level of understanding of the individual interventions. As mentioned earlier, with regards to TEACCH, re-certification is needed every 3 years.[42] This ensures that current agents will be competent and the intended outcomes of the treatments will not be affected negatively. Therefore, an effective intervention will include some sort of mechanism to ensure agents that are carrying out the interventions will be competent.
Treatment complexity:
Treatment complexity is often measured by the number of components of a particular treatment program.[43] Research done has shown us that treatment complexity does indeed have a possibility to affect the intervention programs’ treatment integrity. [44]Treatments being too complex might act as a catalyst for complex programs to be applied without integrity and may be altered to ensure easier conduct of the treatment. This will have an effect on the results of the intervention. Without proper execution of the procedure of the intervention program, it would be difficult to determine accurately the success of a particular intervention program. Most “successful” interventions tend not be to be overly complicated, often opting for simpler options such as visual supports. This is to ensure that the individual with ASD fully understands the process and the procedures with regards to the intervention, increasing the chances of susceptibility of the intervention. Also, with a less complicated treatment, it reduces the likelihood of agents disregarding guidelines and plan due to lack of understanding the treatment process, avoiding affecting the treatment integrity. Therefore, to ensure effectiveness of an intervention, interventions should include a high level of detail, but not involve the use of overcomplicated ideas and approaches.
Treatment adherence:
Another factor which can affect the effectiveness of an intervention, is the intervention’s ability to ensure adherence to the treatment. Treatment adherence is the degree of accurateness of execution of the intervention program. [45]Research has shown that treatment adherence plays an important role in the measurement of the effectiveness of an intervention. If treatment adherence is weak, treatment integrity will be negatively impacted and the effectiveness of the intervention will weaken. As mentioned above, with regards to the use of ABA as an ASD treatment, 5% of the contact hours with the agent within the week needs to be supervised by a certified ABA professional, this ensures that the treatment conducted closely follows the plan, with little or no deviation. [46]This shows us that treatment adherence can be enforced by implementing some form of supervision when the intervention is carried out.
Target outcomes:
Target outcomes of different interventions tend to differ, some by slight margins, some which have wide variations. In my opinion, an effective solution is one which takes a holistic approach to ASD as a whole. Often, individuals with ASD tend to have challenges with more than one aspect of life. Some have difficulties tackling social interactions with others, at the same time lack the ability to communicate clearly and efficiently with others. The many different challenges are what makes up the spectrum of ASD. Interventions which tend to focus solely on one or two aspects of the challenges faced by individuals with ASD will result in an improvement of that particular difficulty faced. However, this will not help the individuals’ integration back into society as most of the challenges faced needs to be tackled. Therefore, it is important for the intervention to treat ASD as a whole and not focus on only certain aspects. I feel this is key to an effective intervention.
Approach taken:
In my opinion, it is important for the intervention applied to recognize the individuals’ talents and strengths and to work on it, to improve them. As mentioned earlier, the main purpose of an intervention is to help overcome certain challenges faced by the individual with ASD and help them such that they are able to integrate back into society with minimal or no help. By focusing on expanding the individual’s current skillset as well as imparting new skills, it gives the individual confidence in themselves. Working on what they do best provides participants with a skill to live on as they integrate back into society. For example, an individual with ASD who is particularly brilliant in mathematics. An effective intervention would include encouraging the individual in their mathematics and expanding their knowledge on what they are good at. Using what they are naturally talented at and expanding their knowledge would be useful in many ways, for example, landing them a job in the future. Therefore, I believe an intervention should recognize the individuals’ strengths to increase effectiveness of the solution.
Flexibility of the interventions:
Every individual with ASD face different challenges, thus it is extremely important that interventions are adapted such that it best suits that one particular individual. Flexibility of the interventions play a big part in the effectiveness of an intervention. Based on the analysis of both interventions listed above, both indicate that the interventions are adapted to suit a particular individual based on the diagnosis and progress of the individual. This is useful as placing every individual in groups varying in severity of ASD and planning the intervention based on that would not be effective. The treatment plans received in these cases may not be applicable for the individual and therefore would be a waste of resources, time and effort. Therefore, I believe that flexibility in the interventions should be placed as a matter of priority in order for an intervention to be effective.
Time frame of the intervention:
Another factor which can affect the effectiveness of an intervention is the time frame of the intervention. Based on the analysis of the two different interventions listed above, the interventions with high intensities, meaning 30 – 40 hours a week proves to be more effective. With high intensive interventions, it allows more to be covered within a few sessions, it also allows time for reinforcement of ideas and knowledge. Research has shown that interventions with generally higher intensities tend to result in an increase in effectiveness of the solution.[47] Conducting the treatment plan at lower intensities may result in individuals being on the losing end. Therefore, I believe that incorporating high intensity hours into the treatment program will be useful in ensuring an increase in effectiveness of the intervention.
Family involvement:
Based on the research done on two considerably successful interventions, both of the interventions had many common aspects. One of which was both placed heavy emphasis on family involvement. [48]This is a key aspect in creating an effective intervention. Family members are the people closest to the individual with ASD. They are the people with most contact, therefore it is important that family members learn how to reinforce ideas and knowledge learnt in the contact time between agents and the individuals. Therefore, I believe that incorporating family involvement into an intervention helps to improve the effectiveness of the intervention.
Summary:
In this essay, I have covered an analysis on 2 different interventions, ABA and TEACCH, both of which are considered to be successful interventions and socially valid interventions. I have also made my own analysis as to what contributes to making an effective solution. Autism Spectrum Disorder consists of a wide spectrum and therefore different ends of the spectrums may require different approaches to treatment plans. In reality, how effective an intervention is will also be heavily dependent on the challenges faced by the individual and the individual’s characteristics. The topics I have covered in this essay definitely do not cover all there is to ASD interventions. However, these are what I believe are the key aspects of ASD interventions.
[1] Autism Speaks. What is Autism? Autism Speaks. Available from: https://www.autismspeaks.org/what-autism (Accessed on 29/8/2017)
[2] NHS Choices. Autism Spectrum Disorder. 06/01/2016 Available from: http://www.nhs.uk/conditions/autistic-spectrum-disorder/Pages/Introduction.aspx (Accessed on 29/8/2017)
[3] NHS Choices. Autism Spectrum Disorder. Autism Spectrum disorder symptoms. 06/01/2017 Available from: http://www.nhs.uk/Conditions/Autistic-spectrum-disorder/Pages/Symptoms.aspx (Accessed on 29/8/2017)
[4] Chaste, P, & Leboyer, M. Autism risk factors: genes, environment, and gene-environment interactions. 2012. Dialogues in Clinical Neuroscience, 14(3), 281–292.
[5] The NHS Information Centre, Community and Mental Health Team. Brugha, T. et al (2012). Estimating the prevalence of autism spectrum conditions in adults: extending the 2007 Adult Psychiatric Morbidity Survey. NHS Information Centre for Health and Social Care
[6] Autism Speaks. Frequently Asked Questions. Autism Speaks. Available from: https://www.autismspeaks.org/what-autism/faq (Accessed on 29/8/2017)
[7] The National Autistic Society. What are the causes and is there a ‘cure’? 2016. Available from: http://www.autism.org.uk/about/what-is/causes.aspx (Accessed on 02/09/2017)
[8] Camarata S. Early Identification and early intervention in autism spectrum disorders: Accurate and effective? International Journal of Speech-Language Pathology. 2014. 16(1), 1-10.
[9] Mundkur N. Neuroplasticity in Children. Indian Journal of Pediatrics. 2005. 72(10), 855-857.
[10] Lynn Kern Koegel PhD. Claire Lazebnik. Overcoming autism: Finding the Answers, Strategies, and Hope That Can Transform a Child’s Life. Viking Penguin. 2004.
[11] Autism Speaks. Treatments and Therapies. Autism Speaks. Available from: https://www.autismspeaks.org/family-services/tool-kits/100-day-kit/treatments-therapies (Accessed on 29/8/2017)
[12] Goldstein, S, Naglieri, JA. Interventions for Autism Spectrum Disorders. 2013. 1(1):10-14.
[13] Child Autism UK. Applied Behavior Analysis (ABA) and Autism. Available from: https://www.childautism.org.uk/about-autism/applied-behaviour-analysis-aba-and-autism/ (Accessed on 04/09/2017)
[14] Baer, DM. A brief, selective history of the Department of Human Development and Family life at the University of Kansas: The early years. Journal of Applied Behavior Analysis. 26(4):569-570.
[15] Ted Talks. Autism and Wandering: How ABA can help keep kids safe, Kupferschmidt S. July 1st, 2015. Available from: https://www.youtube.com/watch?v=CFWo0wMjdzo
[16] Applied Behavior Analysis Treatment of Autism Spectrum Disorder: Practice Guidelines for Healthcare Funders and Managers. Behavior Analyst Certification Board, Inc. 2014. 2nd Edition.
[17] Dictionary.com [internet]. Dictionary.com’s 21st Century Lexicon. Dictionary.com, LLC. Positive Reinforcement. [cited 30/8/2017]; [about 1 screen]. Available from: http://www.dictionary.com/browse/positive-reinforcement
[18] Baltruschat, L, Hasselhorn, M, Tarbox, J, Dixon, RD, Najdowski, CA, Mullins, DR, Gould, RE. Further analysis of the effects of positive reinforcement on working memory in children with autism. Research in Autism Spectrum Disorders. 2011. 5(2):855-863.
[19] Wilkinson, LA. Assessing Treatment Integrity in Behavioral Consultation. International Journal of Behavioral Consultation and Therapy. 2007. 3(3):420-432.
[20]Gresham, MF, Gansle ,AK, Noell, HG. Treatment Integrity in Applied Behavior Analysis with Children. Journal of Applied Behavior Analysis. 1993. 26(2):257-263.
[21] Gresham, MF, McIntyre, LL, DiGennaro, DF, Reed, DD. Treatment Integrity of School-Based Interventions with Children 1991-2005. Journal of Applied Behavior Analysis. 2007 40(4):659-672.
[22] Goldstein, S, Naglieri, JA. Interventions for Autism Spectrum Disorders. 2013. 1(1):23-24.
[23] Luiselli, JK, St. Amand, C, MaGee, C, Sperry JM. Group training of Applied Behavior Analysis (ABA) Knowledge Competencies to Community-Based Service Providers for Adults with Developmental Disabilities. International Journal of Behavioral Consultation and Therapy. 2008. 4(1):41-47.
[24] Luiselli, JK, St. Amand, C, MaGee, C, Sperry JM. Group training of Applied Behavior Analysis (ABA) Knowledge Competencies to Community-Based Service Providers for Adults with Developmental Disabilities. International Journal of Behavioral Consultation and Therapy. 2008. 4(1):41-47.
[25] Applied Behavior Analysis Treatment of Autism Spectrum Disorder: Practice Guidelines for Healthcare Funders and Managers. Behavior Analyst Certification Board, Inc. 2014. 2nd Edition.
[26] Goldstein, S, Naglieri, JA. Interventions for Autism Spectrum Disorders. 2013. 1(1):25.
[27] Applied Behavior Analysis Treatment of Autism Spectrum Disorder: Practice Guidelines for Healthcare Funders and Managers. Behavior Analyst Certification Board, Inc. 2014. 2nd Edition.
[28] Reed, P, Osborne LA, Corness, M. Brief Report: Relative Effectiveness of Different Home-based Behavioral Approaches to Early Teaching Intervention. Journal of Autism and Developmental Disorders. 2007. 37:1815-1821.
[29] Linstead, E, Dixon, DR, French, R, Granpeesheh, D, Adams, H, German, R, et al. Intensity and Learning Outcomes in the Treatment of Children with Autism Spectrum Disorder. Behavior Modification. 2017. 41(2):229-252.
[30] Peters-Scheffer, N, Didden, R, Korzilius, H, Sturmey, P. A meta-analytic study on the effectiveness of comprehensive ABA-based early intervention programs for children with Autism Spectrum Disorders. Research in Autism Spectrum Disorders. 2011. 5(1):60-69.
[31] Peters-Scheffer, N, Didden, R, Korzilius, H, Sturmey, P. A meta-analytic study on the effectiveness of comprehensive ABA-based early intervention programs for children with Autism Spectrum Disorders. Research in Autism Spectrum Disorders. 2011. 5(1):60-69.
[32] University of North Carolina School of Medicine. TEACCH Professional Certification Program. TEACCH Autism Program. Available from: http://teacch.com/trainings/teacch-professional-certification-program Accessed on: 2/09/2017
[33] Mesibov, GB, Shea, V, & Schopler, E. The TEACCH Program in the Era of Evidence-Based Practice. Journal of Autism and Developmental Disorders. 2010. 40(5):570-579.
[34] University of North Carolina School of Medicine. Our Mission and Vision. TEACCH Autism Program. Available from: https://www.teacch.com/about-us/mission-st Accessed on: 02/09/2017
[35] University of North Carolina School of Medicine. TEACCH Certified Practitioner Level. TEACCH Autism Program. Available from: http://teacch.com/trainings/teacch-professional-certification-program/teacch-certified-practitioner-level Accessed on: 2/09/2017
[36] Field, S, Hoffman, A. The importance of Family Involvement for Promoting Self-Determination in Adolescents with Autism and other Developmental Disabilities. Focus on Autism and Other Developmental Disabilities. 1999. 14(1):36-41.
[37] Virues-Ortega, J, Julio, FM, Pastor-Barriuso, R. The TEACCH program for children and adults with autism: A meta-analysis of intervention studies. Clinical Psychology Review. 2013. 33(8):940-953.
[38] Tsang, SKM, Shek, DTL, Lam, LL, Tang, FLY, Cheung, PMP. Brief Report: Application of the TEACCH Program on Chinese Pre-School Children with Autism-Does Culture Make a Difference? Journal of Autism and Developmental Disorders. 2007. 37(1):390-396.
[39] instead, E, Dixon, DR, French, R, Granpeesheh, D, Adams, H, German, R, et al. Intensity and Learning Outcomes in the Treatment of Children with Autism Spectrum Disorder. Behavior Modification. 2017. 41(2):229-252.
[40] Goldstein, S, Naglieri, JA. Interventions for Autism Spectrum Disorders. 2013. 1(1):20-21.
[41] Perepletchikova. F. & Kazdin. AE. Treatment integrity and therapeutic change: Issues and research recommendations. Clinical Psychology: Science and Practice. 2005. 12(4):365–383.
[42] University of North Carolina School of Medicine. TEACCH Certified Practitioner Level. TEACCH Autism Program. Available from: http://teacch.com/trainings/teacch-professional-certification-program/teacch-certified-practitioner-level Accessed on: 2/09/2017
[43] Zarcone, J, Hagopian, L, Ninci, J, et al. Measuring the Complexity of Treatment for Challenging Behavior using the Treatment Intensity Rating Form. International Journal of Developmental Disabilities. 2016. 62(3):183-191.
[44] Goldstein, S, Naglieri, JA. Interventions for Autism Spectrum Disorders. 2013. 1(1):24-25.
[45] Johns Hopkins Center for Health Equity. Treatment Adherance. Available from: https://www.jhsph.edu/research/centers-and-institutes/johns-hopkins-center-for-health-equity/about/influences_on_health/treatment_adherence.html (Accessed on 22/09/2017)
[46] Applied Behavior Analysis Treatment of Autism Spectrum Disorder: Practice Guidelines for Healthcare Funders and Managers. Behavior Analyst Certification Board, Inc. 2014. 2nd Edition.
[47] Linstead, E, Dixon, DR, French, R, Granpeesheh, D, Adams, H, German, R, et al. Intensity and Learning Outcomes in the Treatment of Children with Autism Spectrum Disorder. Behavior Modification. 2017. 41(2):229-252.
[48] Field, S, Hoffman, A. The importance of Family Involvement for Promoting Self-Determination in Adolescents with Autism and other Developmental Disabilities. Focus on Autism and Other Developmental Disabilities. 1999. 14(1):36-41.
Cite This Work
To export a reference to this article please select a referencing stye below:
Related Services
View all


Related Content
All TagsContent relating to: "Health"
Health is the general condition of the body or mind. The World Health Organization defines health as “a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity.”
Related Articles

DMCA / Removal Request
If you are the original writer of this dissertation and no longer wish to have your work published on the UKDiss.com website then please: