An Exploration of the Nurses’ Role in Improving Quality of Life (QoL) in Patients with Motor Neurone Disease (MND)
Info: 7561 words (30 pages) Dissertation
Published: 9th Dec 2019
An exploration of the nurses’ role in improving quality of life (QoL) in patients with motor neurone disease (MND)
What is motor neurone disease and why is this a topical issue
Harris et al (2018) describe motor neurone disease (MND) as a neurological disease of the central nervous system, with a quick and complex progression. This definition implies the brief window of opportunity that healthcare professionals have, to deliver the correct care.
Ramanathan and Rana (2018) report the average age of symptom onset as 58.6 years, their oldest case being 86 years. Hobson et al (2017) reported on a 17-year-old male with a nine-month history of swallowing difficulties, who died. This appears to suggest that age onset of MND is variable. Khadilkar et al (2018) propose the incidence of MND as 1.5-2/100,000 each year, this statistic is validated by the MND association.
A minority of cases of MND are familial, however most cases are sporadic in nature, (Talbot 2002, Khadilkar et al 2018). Burchardi et al (2005), although dated remains true, that MND can present in different ways, however the trajectory of the disease is predictable and usually terminal; with the majority of MND patients dying of respiratory related complications. The authors indicate that if symptoms begin in the patients’ limbs then this is termed ‘limb onset’ whereas if symptoms start with speech and swallowing difficulties, this is termed ‘bulbar onset’.
Harris et al (2018) propose that MND results in a patient having multiple complex needs. The general trajectory is to disrupt the motor neurons that connect the brain to the muscles of the body, this results in muscles weakness, spasticity and fasciculations. Over a period of time, the patient will lose ability to control the muscles in their body, leading to mobility issues, dysphagia, dysarthria, respiratory failure and eventually death.
Morley et al (2018) propose that the prognosis in MND is three years, the progression is rapid and predictable, however there are exceptions. Albert et al (1999) found that over 50% of their follow up visits of MND patients died after one year. Possibly, Albert et al (1999) had a cohort of people with advanced disease anyway, however this demonstrates the dramatic and variable timeline of MND.
Dawson et al (2002) proposed that advances in technology mean that MND patients are living longer and therefore reliant on others for longer periods of time. Dawson’s dated observation is supported by Kiernan (2017) who discusses therapies in development targeted at MND, for example, physiotherapy, massage and meditation. In a resource-led climate, at this time, this may imply future challenges for health professionals when supporting patients with MND.
As mentioned above, MND is a somewhat predictable disease, however with modern advances there is a shift in attitude from one of nihilism to one of optimism and patients are surviving longer. MND patients will be dependent on others for an extended period of time as their bodies fail. For this reason, planning for this eventuality is a topical health issue which must be addressed in order to avoid crisis-led decision management. This review aims to explore the nurses’ role in improving QoL in MND patients.
What is the concept of quality of life and why is it important?
Marcia and Simonson (1996) describe how in 1948 The World Health Organisation (WHO) defined health as not only physical, but also psychological and spiritual. In 1973 a database search of Medline showed five articles with quality of life (QoL) as a keyword, this then grew exponentially in the subsequent five years to 1252; demonstrating the growing interest in the concept.
Cella (1993) supports the theory that after many years of being considered less important than physical health, that QoL is now considered more seriously. She proposes that rather than the absolute traditional goal of symptom management, that a patient’s QoL is starting to take a front seat in treatment goals.
In relation to MND, QoL now appears to be emerging as good practice as proposed by Harris et al (2018). The authors purport that MND management should focus around QoL, however, to date, more importance has been placed on the physical side of treatment.
Leigh et al (2003) expand on this and note that a lot of progress has been made between 1990-2000 in the field of MND, and there has been an attitude shift from one of nihilism to one of optimism. In 2005, the National Service Framework for long term conditions was released and this brought about a change in the concept of caring for people with long term conditions.
Simmons et al (2000) conducted a study that discovered MND patient’s did not measure their QoL by their physical weakening but rather their psychological and existential factors. Simmons is supported by Goldstein (2002) who proposes that QoL in MND patients should not be entirely based on physical ability and should take into account their support systems.
Oberstadt et al (2018) support both Simmons and Goldtein, and propose that a person diagnosed with MND will most probably experience a vast array of emotions including hopelessness and despair, and therefore interventions to supports psychological wellbeing are essential.
Arguably a person’s QoL is subjective, because it is a lived experience that no other person will experience in the same way; a person may find contentment in spiritual aspects as opposed to physical aspects. Skevington and Bohnke (2018) propose a definition of a persons’ subjective wellbeing and quality of life as concepts describing experiences, capacities, states and behaviours.
A person’s experience of MND is somewhat predictable due to the nature and trajectory of the disease, therefore it could be argued that a person’s QoL in MND maybe predictable to an extent.
Harris et al (2018) propose that current research in the field of QoL in MND places emphasis on wellbeing issues of the patient and their carers’. Harris et al (2018)’s observation suggests that research is person centred as it seems to place the patient at the centre of their care, and address issues of relevance for the patient on an individual basis, as well as holistic in approach because it addresses broader issues than the physical aspects.
Arguably this shift from medicalised treatment to more person centred and individualised treatment is an example of the social model of care.
Synthesis indicates that QoL appears to be important in relation to MND management in recent years and this should be taken into consideration in the management plan of patients, as MND patients live longer. This review will explore the role of the nurse and how they may be ideally placed to improve QoL in MND patients.
Review aim and design
The aim of this review is to discover how nurses can improve quality of life (QoL) for patients living with motor neurone disease (MND), as outlined above. This will be achieved by an integrative review process which refers to identification of relevant studies (quantitative and qualitative), analysis of the findings, followed by synthesis (Burns and Grove, 2010). The authors indicate that an integrative review process allows us to find the most relevant information. Burns and Grove argue that the value of the integrative review is underpinned by rigor of the methodical process.
Search method
Grewal et al (2016) proposes that databases are a key component to utilise to ensure relevant information is obtained. This marries with Bramer et al (2017) who encourages multiple databases to be used to ensure relevant data is obtained.
A comprehensive literature search was conducted using electronic databases: CINAHL, Ovid, Science Direct and Internurse. The database search was conducted using keywords which narrowed down the results, these included: Motor Neuron Disease OR MND, Advance care plan OR ACP, nurs*, quality of life OR QOL. See table 1.1 below.
The table below shows the databases accessed and the final number of papers included from each database.
| Database: | CINAHL: 2 |
OVID: 1 |
ScienceDirect: 1 | Internurse: 1 |
Total: 5 |
The table below contains the keywords and Boolean phrases that were used in this review.
| Motor Neurone Disease OR MND |
| Quality of Life OR QoL |
| Advance Care Plan OR ACP |
| NURS* |
After the databases were searched using the keywords and Boolean phrases a list of inclusion and exclusion criteria was applied. See table 1.2 below.
| Inclusion | Exclusion |
| Must originate from an academic database.
Papers must contain more than one keyword or Boolean phrase. Papers must have been published after 2005. Papers must be published in English. |
Papers originating from other sources than an academic database.
Papers that contain one or less keyword or Boolean phrase. Papers published prior to 2005. Papers written in a language other than English. |
The decision was taken to exclude articles published prior to 2005 because evidence suggests that a focus on a MND patient’s QoL is a recent development. In 2005, the DoH released a National Service Framework for Long Term Conditions which affected the field of MND. This review is looking at an exploration of the nurses’ role and how they can impact a MND patient’s QoL, therefore it is logical to use the most up-to-date information.
Reliability and type of research paper
It is vital to obtain data that are reliable and valid in nature, this is achieved by a comprehensive searching approach (Smith and Nobel 2015). Leung (2015) agrees with Smith and Nobel’s (2015) proposal that a robust and comprehensive search method should be utilised to avoid undependable results.
Leung (2015) discusses the two types of research that may be found. Firstly, qualitative research uses distinct terminology to quantitative research. Qualitative research gravitates around recognising patterns or themes to establish a meaningful concept or idea whereas quantitative research uses statistics and numeric values.
Qualitative research is used more to influence primary healthcare because of the desire to capture the patients lived experience. MND patients may be likely to access primary healthcare due to the nature of the disease (Leung, 2015).
The table below details the papers collected from the comprehensive database search.
| Paper title | Author(s) | Year | Methodological Approach |
Sampling size | database |
| The meaning of living with uncertainty for people with motor neurone disease | Harris, D
Jack, K Wibberly, C |
2018 | Qualitative | 4 | CINAHL |
| Assisting patients with motor neurone disease to make decisions about their care. | Gale, C | 2015 | Qualitative | 1 | Internurse |
| Assessing social isolation in motor neurone disease: A Rasch analysis of the MND Social Withdrawal Scale | Gibbons, C
Thornton, E Ealing, J Shaw, P Talbot, K Tennant, A Young, C |
2013 | Quantitative | 298 | ScienceDirect |
| Developing hospice-based, nurse-led clinics to improve care for patients with MND |
Bennett, W Mitchell, D Callagher, P Jones, R |
2009 | Qualitative | 55 | CINAHL |
| Comparison of Mood and Quality of Life Among People with progressive neurological illness and their caregivers. |
McCabe, M Firth, L O’Connor, E |
2009 | Quantitative | 753 | Ovid |
Appraisal of papers collected
The databases search yielded 1,013 papers as demonstrated in the bar chart.
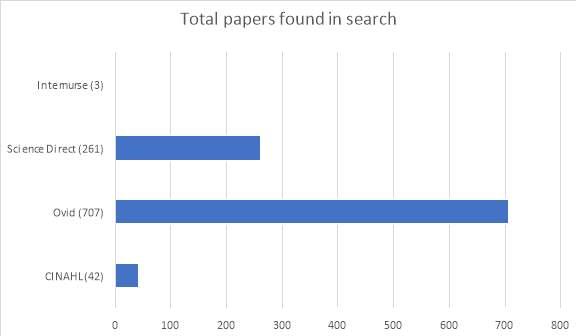
Abstracts of the papers were screened for relevance as well as duplications removed, after which papers deemed of little to no importance were disregarded. This process dramatically reduced the total number of papers. The funnel chart below demonstrates this process using the database which yielded the largest number of papers (n).
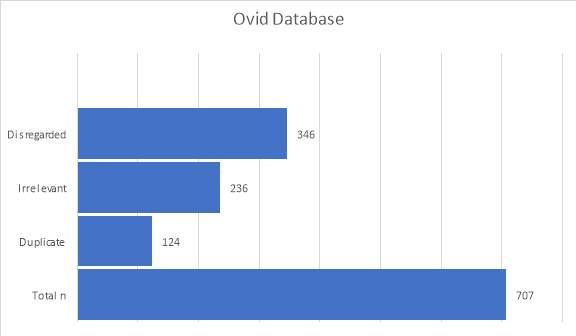
The table above is a visual representation of the robust search process used in the Ovid database. CINAHL, Science Direct and Internurse databases were also used, however, did not yield as high a number of search results and therefore no table has been created.
The number of papers remaining after the search and screening processes were performed was five; three qualitative papers and two quantitative papers.
Appraisal considerations
This review utilises an adapted version of the CASP framework and Caldwell’s framework (2005) with the aim of appraising the papers. These frameworks helped the author to comprehensively appraise each of the papers because of the rigor of the questions and considerations.
Qualitative appraisal
There were three qualitative papers used: Bennett et al (2009), Gale (2015) and Harris et al (2018). The papers used qualitative methodologies because they are based on lived experiences and subjectivity rather than statistics and numeric data.
Hammarberg and Kirckman (2016) propose that qualitative methodologies can be juxtaposed against quantitative methodologies for this reason. Furthermore, there is an increasing recognition of the role that qualitative research plays in nursing, for example, in primary care services because of the need to capture the lived experienced of individuals (Houghton et al 2013).
Methods and data collection of the qualitative papers
Bennett et al (2009) and Gale (2015) utilise case studies as the basis of the paper. Houghton et al (2013) states that this method of data collection often focuses on an individual or experience in a local arena, and therefore transferability may not be possible in a broader context. Yin (2013) proposes that case studies pose many challenges in terms of validity and generalisability because of the highly- limited case numbers, and can be based entirely on one case; this may reduce credibility.
However, Lincoln and Guba (1985) propose that an extended period of monitoring will allow for greater credibility and dependence. Yin (2013) also recognises that case studies can have grater validity by using triangulation, for example identifying two or more cases that report the same outcome.
Denzin and Lincoln (2005) further elaborate and propose that a researcher should remain in the case study site until saturation has occurred, or in other words, until they feel satisfied that all of the themes are discovered. Saunders et al (2018) explains that the concept of saturation is widely accepted, however the authors warn that a structured approached should be used with the concept to ensure it doesn’t lose coherence in its’ application.
A critique of Gale (2015) may be that her paper lacks completeness and confirmability due to the decision to use a single case study over a minimum period of one year. However, as proposed by Denzin and Lincoln (2005) an author may feel that saturation point has been achieved thus making the case study more credible and increasing transferability.
Crowe et al (2011) propose that a case study must lend itself to the research question, which suggests that the emphasis lies here rather than on the time covered. Gale (2015) has been deemed as relevant because it appears to lend itself well to the research question and contains multiple keywords and Boolean phrases. Bennett (2009) bases the paper on a case study over 8 years, therefore having high credibility, dependability and possible transferability to a broader context.
Harris et al (2018) employ interviews as a method of data collection, that were later subjected to interpretive analysis. Green and Thorogood (2018) recognise that interviews can be a robust way of data collection; however, they state that there are many types of interview technique, for example, guided interviews, face to face interviews, telephone interviews or email correspondence; which provide advantages and disadvantages.
Harris et al (2018) utilise open ended questions and does not interrupt the speaker until they have finished. Rapley (2001) proposes that open ended interviews are very dependable, however, emphasises that no one method of data collection is better than another.
A critique of Harris et al (2018) may be that the author carried out the interviews personally. Green and Thorogood (2018) propose that it may be inappropriate to perform interviews personally due to bias. The consequence of having bias from an author or participant may mean that internal and external validity are affected.
Rapley (2001) recognise the potential for bias when using interviews, and states that both the interviewee and interviewer work to construct themselves within the interview itself via reflexivity. Arguably, reflexivity is the unintended influence that the author or the participant has on the outcome of the study.
Sampling appropriateness
Green and Thorogood (2018) recognise that there are many different sampling techniques, for example, purposive sampling whereby the investigator will use predefined criteria to find a sample, or convenience sampling where a sample is selected because of mere convenience.
Green and Thorogood (2018) propose that research protocol indicates that the logic and sampling strategy should be disclosed for transparency. Sheldon (1983) proposed that budget and time constraints will always be an influencing factor on sampling. Robinson (2014) proposes that sampling is central to qualitative research and that to obtain trustworthy data, sampling must be correct. The consequence of erroneous sampling may be untrustworthy data.
Pannucci and Edwin (2010) propose that bias is any tendency which prevents unprejudiced consideration of a question, for example, if monitory value could be gained from a specific outcome was identified. The authors propose that there is usually always minor bias in a published article, of one kind or another. Smith and Nobel (2014) substantiate this discourse and suggest that bias is difficult to eliminate. Pannucci and Edwin (2010) propose that one way of avoiding bias is by disclosing any associations.
Bias in qualitative papers can be categorised differently than that of quantitative papers due to the nature of the research being subjective and experienced based (Hammarberg and Kirkman, 2016). Chenail (2011) proposes that bias and its management is a large issue within qualitative research, the author suggests that any data collection method should be tested to ensure it works as envisaged.
Qualitative papers
Bennett (2009) and Gale (2015) appear to employ a convenience sampling method. Convenience sampling is termed as such because of the ease of accessibility in relation to the researcher (Etikan et al 2016). Brodaty et al (2014) recognise that a convenience sampling approach may be inappropriate because of the risk of bias from the author or participant. Schwarcz et al (2017) appear to agree with Brodaty’s (2014) proposal because the author sates that the representativeness of the sample may be compromised by using a convenience sampling method. Arguably, a convenience sample may not include the necessary individuals to achieve the desired outcome. It could therefore be argued that the trustworthiness of the paper is reduced.
However, the decision was taken to include these papers because of its’ relevance to the line of enquiry. It was felt that the papers provided realistic material qualitatively.
Harris et al (2018) employ a purposive sampling method. Etikan et al (2016) propose that this method of data collection differs from a convenience sampling approach because it indicates that the researcher has selected the participants because they meet a set of criteria. Robinson (2014) refers to an inclusion and exclusion criteria as defining a target population.
Harris et al (2018) utilise a purposive sample size of four. Robinson (2014) proposes same sizes for qualitative research should be sufficiently small so that participants have a voice and suggests a guideline of 3-16. Emmel (2013) proposes that to obtain realistic explanations of phenomena, purposive sampling is ideal and more than abstract ideas are needed.
Ethical considerations.
Rensik (2015) proposes that ethics is a branch of philosophy that encompasses morals, in research, it tries to ensure that researchers are accountable for their work and to promote collaborative working. The author suggests that a paper can be ethically correct however be morally wrong, or visa versa.
Casey and Shaw (2010) highlight the many potential ethical issues with qualitative research which include consent and research-participant relationship. Pannucci and Edwin (2010) recommend disclosures as a way to avoid bias.
Bennett (2009) and Gale (2015) have an ethical issue of researcher-patient relationship because they are both clinical nurse specialists and provide services to the patient involved in the research. It appears that the papers have a solid moral stand point in their aim, however risk ethicality.
Toombs et al (2017) acknowledge this interaction however propose that for this reason the researcher must engage with authenticity in all their actions, for example, being transparent and genuine in their work. Goldstein (2017) also acknowledges this entanglement and further proposes that this reflexivity can bring meaningful findings. Arguably, if an author or participant is creating bias, then the external validity may be compromised.
Both papers were included because they appear to be authentic and provide meaningful findings, and they will likely triangulate with the other papers’ themes. Bennett (2009) and Gale (2015) disclose full consent in their papers with no conflicts of interest, or potential funding influences, which further increases dependability.
Harris et al (2018) produced a paper that has been independently funded, however, this was in fulfilment of a Ph.D for a University. Arguably, a university may want research of a certain type or a specific line of inquiry and therefore influence outcomes. Posselt (2018) discusses the importance of safeguarding for any potential bias in doctoral research.
It does not appear that this paper’s line of inquiry is bias nor the data collection method. The second possible ethical issues with this paper is the element of reflexivity due to the fact that the interviewer positioned themselves within the interviews. This appears to have been counteracted to the best of the researcher’s ability because they allowed the interviewee to tell their story and did not interrupt them until the end. This appears to increase the level of authenticity of the paper because outcomes are less likely to be bias.
Informed consent was obtained and disclosed therefore increasing dependability. The paper states that beneficence was one of the researchers concerns and it detailed how it would safeguard this, this disclosure demonstrates that the researchers were acting with authenticity.
Appraisal of the quantitative papers
Amira and Elsaid (2018) propose that research is fundamentally about trying to discover the world in a structured way. The author suggests that people approach research assuming characteristics which has developed into two distinct types: qualitative and quantitative approaches. They also propose that qualitative and quantitative methods can complement each other, for example, quantitative research may show that a type of dressing is more effective and qualitative research may identify that patients find a type of dressing easy to manage and more comfortable.
There is one quantitative paper which was published in Australia, it was decided to include this paper because MND is a global issue and therefore requires us to work collaboratively across countries (Feigin et al 2017).
Methods and data collection of the quantitative papers
Gibbons et al (2013) and McCabe et al (2009) both utilise a self-administered questionnaire as the method of data collection. Gibbons et al (2013) document that they administered these to patients who attended a clinic on a certain day, arguably this could miss many patients as not all patients attend the clinic every day, and therefore this method potentially excludes many patients and causes potential issues which may affect the outcomes of the paper.
Gibbons et al (2013) acknowledges that in cases where the patient is unable to complete the questionnaire, that a carer may do this on their behalf. Debatably, this may not reflect the true feelings of the patients due to potential carer bias.
McCabe et al (2009) documented that participants were recruited by responding to an email and asking to be involved. Possibly, not every person uses email and therefore this potentially excludes many participants. McCabe et al (2009) documents how after email contact a questionnaire was then posted which must have been completed in 6 weeks or the participant wasn’t included. Reasonably, everything must have a deadline or cut of point, however this may have excluded a patient if they were travelling or away for a period of time.
However, there were no guidelines for completion of the questionnaire. Therefore, the patient may not have been the one to complete the questionnaire, for example, if they had a carer. This may have affected the outcome.
Bryman (2016) proposes that self-administered questionnaires are less reliable because it is unknown who is completing them and there may be missing data. Sudman et al (1965) proposed that self-administered questionnaires are an effective data collection method because of a high cooperation rate. Gibbons et al (2013) did have a high cooperation number of 298. McCabe et al (2009) also had a high cooperation rate of 423 patients and 335 caregivers.
Sampling of the quantitative papers
Gibbons et al (2013) details that he recruited the participants from five different regional locations, and who conformed to preselected criteria. This sampling technique appears to be purposive in nature.
Emmel (2013) proposes that to capture realistic data purposive sampling is required. It was decided that the high cooperation rate, alongside the sampling method and the large sampling areas would increase generalisability and reliability.
McCabe et al (2009) states that participants from different illness groups were recruited but not from varying locations across the region, therefore this may decrease reliability because the author is not using samples from many different locations. Possibly, one location may show different traits than another location, therefore it is important to use samples from varying locations. McCabe et al (2009) did have a high cooperation rate, and therefore it was decided that generalisability may remain.
Ethics of the quantitative papers
Gibbons et al (2013) appears to have an ethical issue in the fact that the paper was funded by 17 bodies. The funding parties are broad in range from a statistician, to an R&D Manager to Consultants and Nurses. There may be room for bias to occur between all the different avenues of funding.
Gibbons et al (2013) has ethical approval confirmed, and has disclosed no conflicts of interest. It was decided that the paper appears reliable because of the ethical approval status and no disclosure of conflict of interest.
McCabe et al (2009) declares limitations on itself, which appears to be transparent. Carr et al (2018) propose that a researcher must be able to recognise the limitations of their research as it is critical to implement appropriate strategies.
McCabe et al (2009) has ethical approval, has no conflicts of interest and is funded by the Australian Research Council. It was decided that this paper was reliable for these reasons.
Thematic Analysis
Braun and Clarke (2008) propose that within qualitative research especially, that thematic analysis is used as analytical method. In this review, thematic analysis has been used on each of the papers, for continuity. Each of the articles were analysed to note the patterns of regularly occurring words. The same process was applied to each of the papers used in this review.
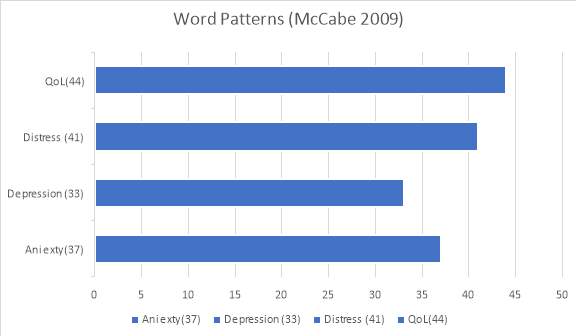
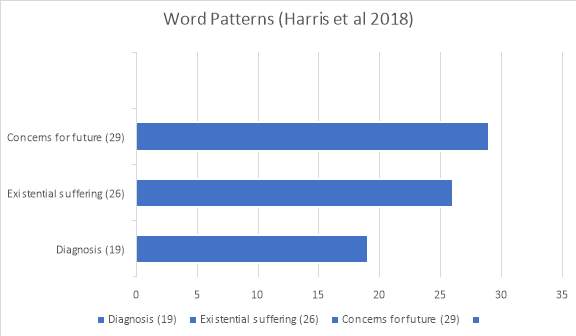
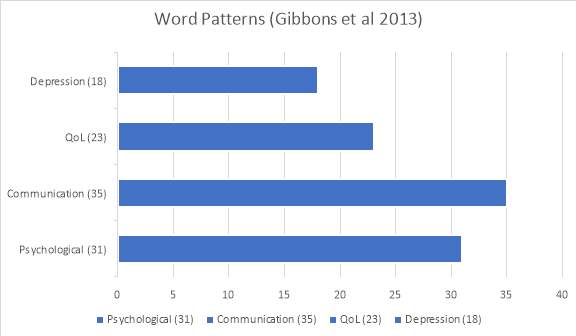
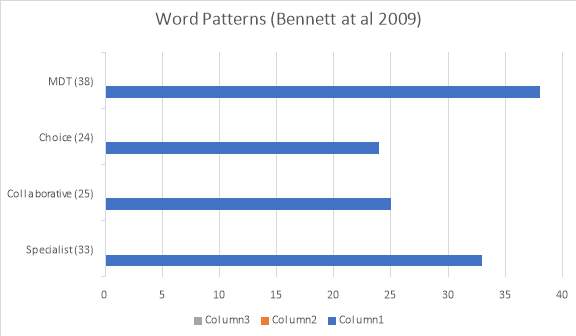
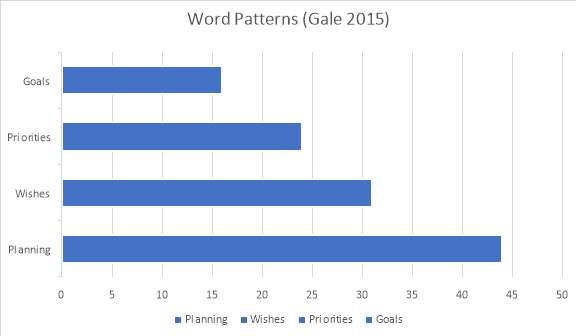
After the thematic analysis process was applied to each of the papers, themes were deciphered from the patterns of reoccurring words. See table below for the themes that were decided upon.
| Themes: | McCabe (2009) | Harris et al (2018) | Gibbons et al (2013) | Bennett et al (2009) | Gale (2015) |
|
x | x | |||
|
x | x | x | ||
|
x | x | x | ||
| (3a) Advance care planning. | x | x | x | ||
| (3b) Speech and swallowing. | x | x |
Communication of diagnosis delivery (1)
MND affects the motor neurones, and therefore mobility and functionality of the body. Kent (2012) and Galvin et al (2017) propose that diagnosis of MND relies on clinical presentation of the disease, and it is proposed that diagnosis is easier when symptoms are established.
Baxter and McDermott (2017) acknowledge that it may be challenging to reach a diagnosis of MND based on clinical presentation, however highlight that GPs most commonly cite fasciculations as the principle reason for a referral onwards to diagnostic services. The authors state that speech problems is the least common referral reason.
Baxter and McDermott’s (2017) proposal is curious as Barber (2015) proposes that people who experience MND will experience many symptoms and Speech and Language Therapists will play a large role in their care. The author proposes that 86% of MND patients will experience dysphagia. McDermott and Shaw (2008) proposed that slurring of speech is often the first symptom to present and orthopnoea is least likely.
It appears there may be a lack of education surrounding the diagnostic characteristics of MND. A package of education aimed at nursing and medical staff may be beneficial to overcome this, with the intention of ensuring that characteristics are not overlooked.
Baxter and McDermott (2017) highlight that nursing and medical staff in a surgery setting perceive their role as to refer onwards rather than attempt a diagnosis and that only one third of them are aware of a decision-making tool ‘Red Flags’ to aid with MND diagnosis. Arguably, if staff adopt an indifferent attitude towards diagnosis, this may cause delays.
Galvin et al (2017) states the median time from first symptoms to diagnosis is 12 months. Donaghy et al (2007) proposed a similar figure of 15.6 months, the author added that over the previous 40 years there had been negligible change.
Time to diagnosis appears to be influenced by many factors as proposed by Soundy and Condon (2015), including a lack of understanding of behalf of the general public or nursing and medical staff. Kent (2012) states that a nurse practitioner or GP is likely to see between one and two cases of MND in their career and therefore may be lacking in skills for diagnosis.
Kent (2012) proposes that a later diagnosis may be because a patient does not recognise symptom onset or even denies that they have symptoms. It appears that the onus is on the patient in the first instance to recognise the onset of symptoms, to be able to report to primary care services. Baxter and McDermott (2017) propose that if the nursing or medical team refers to a secondary service that is not an MND specialist neurologist then delays are likely to occur.
Evidence suggests that when minor symptoms emerge they may not be recognised or it may be a lengthy process to reach a formal diagnosis. Kent (2012) reports that MND is a relatively rare disease. Hogden (2017) suggests the lifetime risk of acquiring MND is 1:400. The rare occurrence of the disease may mean that nurse practitioners and GPs are unfamiliar with the clinical presentation. McDermott and Shaw (2008) state that there is lack of a definitive test for MND and therefore this may hinder a diagnosis because it relies on interpretation of clinical presentation.
It may be beneficial to engage the general public with a campaign surrounding MND which would increase awareness within communities and encourage people to make an appointment with their nurse practitioner or GP if they are concerned.
Aoun et al (2017) proposes that many patients report dissatisfaction with their care due to lack of compassion and blunt communication styles. Auon et al (2016) proposes that up to 70% of nursing and medical staff that work within the speciality of MND reported that MND diagnosis delivery was ‘somewhat to very difficult’ and that up to two thirds of the participants were interested in more training.
Aoun et al (2017) explains that often long term emotional distress is engendered from the poor communication. Tools to aid communication strategies already exist in practice, for example, the SPIKES model, therefore it may be that nursing and medical staff are choosing to ignore them. This is a barrier to practice and may be detrimental for patients.
Nurse and mental health in MND. (2)
Sandy and Condon (2015) propose that research into mental health within MND is needed because of lack of visibility at this time. Gluyas et al (2017) further propose that mental health of both patient and informal caregivers needs to be researched in depth because there has been a lack of attention paid to this area, historically. Arguably, the role of research nurse is ideally placed access this cohort of people.
Hogg et al (1994) identified that there were high levels of depression among MND patients, and that acceptance of the disease was related with symptomology. Gluyas et al (2017) further explains that social isolation and income-isolation may occur due to mobility and lifestyle restrictions as the disease progresses. Harris et al (2018) proposes that psychological distress may be caused because of the time-consuming nature of MND as the disease progresses and bodily function is lost.
There is a gap in research that may be filled with the role of research nurse, recruiting a sample of MND patients and their caregivers to explore mental health. This will help to answer the question if nurses are able to improve and QoL in MND patients. Mental health arguably contributes to QoL in any patients and therefore merits attention.
Skelton (2005) states that post diagnosis is it essential that the district nurse visit the patient in order to establish a therapeutic relationship. Skelton (2005) proposes that the nurses’ initial role is to monitor and provide psychological support to the patient and that best management of MND is to adopt an MDT approach. Arguably, the nurse will play a central and important role in the disease journey of the patient.
The National Institute for Health and Clinical Excellence has guidelines for the management of MND, and it recommends that care should be organised via a MDT approach in a clinic environment, either in a hospital or community setting; at intervals of 2-3 months. Evidence indicates that mental health is a dominant issue within MND at this time.
Maybe there is a correlation between the frequency of supportive interventions provided by the MDT nursing teams and the severity of any mental health issue. If the nurse can identify a need to change their practice then maybe part of the workload can be delegated to other healthcare professionals, for example, care assistants. This may allow more frequent contact to be established with the MND patient and in turn this may help their psychological health by providing more opportunity to share concerns and information.
Palliative concerns in MND (3)
Advance care planning (3a)
Brinkman-Stoppelenburg et al (2014) proposes that ACP is discussing and recording a patients’ wishes and preference in relation to health goals, especially in patients who may lose capacity. Michael et al (2017) further explain that ACP brings patient satisfaction through enhancing QoL and can allow for prompt palliative and end of life care when the time comes. Makaroun et al (2018) proposes that ACP must be an early intervention because as an illness enters its final stages or there is a transition to end of life care in the last three days of a persons’ life without an ACP, this can lead to poor quality of care. Ingravallo et al (2017) agrees with Makaroun’s proposal however further explains that by meeting a patients’ wishes and preferences we can achieve a better quality of care and avoid potentially detrimental care. It appears that ACP is seen a positive concept in a lot of the literature.
Brinkman-Stoppelenburg et al (2014) highlights that there must be more research into ACP and how this improves QoL. There is a gap in research which could be filled by a research nurse. A nurse is ideally placed to access cohorts of people who will utilise ACP, and to be able to extract pertinent information which could add to the exploration of improving QoL in patients with MND.
Schickedanz et al (2008) proposed patient-identified barriers to ACP which included perceiving ACP as irrelevant, personal barriers and needing more information. The author also identified that up to 90% of the participants did not document ACP wishes, which may have led to care goals not being met. The literature states that a barrier to ACP can be family members and their dynamics, (Poole et al 2017; Boerner et al 2013). This identifies that in some situations family education is essential and must be provided.
Seymour et al (2010) proposes that nurses generally see ACP as a celebration of good nursing care and that policymakers are keen to expand its’ use. The author highlights that nurses view barriers to practice as: when to initiate ACP, differences in people, resources and talking about death. Fan and Rhee (2017) further state that nurses are well positioned to initiate ACP, and have a positive attitude towards it. Interestingly, Fan and Rhee (2017) propose good documentation as a barrier to practice with patient education.
Nurse educators could play a role in overcoming these barriers to practice by way of education. Nurse educators must provide more robust training for documentation as all nurses currently have their own way of documenting events (NMC, 2015).
Speech and language (3b)
Whitehead et al (2012) propose that MND is a terminal disease, therefore it is important to pay attention to end of life care, and that currently more input is needed from palliative care teams. Arguably, a holistic approach should be combined with a MDT approach to try and minimise the risk of overlooking any aspect of the patient. Vesey (2017) proposes that speech and language problems are likely to arise as MND progresses. The author states that dysarthria can often lead to anarthria which will result in reliance and even total reliance on augmented and alternative communication (AAC).
Murphy (2009) proposes that despite many patients relying on AAC to communication appropriately, that many patients are determined to use their own voice as they see the technology as a defeat. Possibly, admitting defeat would be detrimental from a patient’s perspective and may lead to increased morbidity and mortality. Murphy (2009) explains that it is difficult to know at what point AAC may be introduced, however it is important to introduce it whilst the patient is still able to learn how to use it.
It appears important for nurses to have education in specialist areas in order to make appropriate referrals for early interventions. As part of the MDT, Speech and Language therapists are important, however nurses are positioned very well to continue working with the patient alongside this type of supportive intervention.
Regular e-learning updates or training days for nursing staff would ensure that the frontline staff have the necessary knowledge to be able to provide care for patients. A barrier to this nursing practice may be a lack of resources or funding, especially in a community setting.
Recommendations for nursing practice
A recommendation to change nursing and medical practice should be to introduce a checklist for MND screening with advice to refer to an MND specialist neurologist directly. This suggestion may decrease unnecessary referrals and subsequent delays in treatment. Barriers to this change in practice may be that professionals do not conform to the checklist for personal reasons, therefore an audit may be useful to ensure its’ implementation.
If nursing and medical staff can improve the communication style around diagnosis of MND then this may provide relief and avoidance of emotional distress that potentially can be engendered from poor communication styles. Therefore, a recommendation to change nursing and medical practice should be to ensure communication strategies are in place and being used by professionals correctly. Further research must be conducted into communication styles around diagnosis delivery in MND patients, to note if there can be any improvements made.
This review has shown that research into mental health within the field of MND is limited, and therefore a recommendation to nursing practice must be that more research into mental health within MND needs to be conducted in order to improve the QoL of MND patients.
Secondly, research must be conducted to discover if there is link between frequent nursing interventions and mental health outcomes. A change to nursing practice may be to increase the frequency of MND patient visits or contact and this may improve QoL for the MND patient. A barrier to this change in practice may be the workload that nurses and care assistant’s already have.
This review has highlighted that ACP is a large issue within MND and a recommendation to change nursing practice must be that nurses need to help people overcome barriers to ACP; as there are many. School nurses may be ideally positioned to disseminate information tailored younger children in a child friendly way, to introduce the concept of ACP in schools, with a focus on its’ relevance in adulthood. This new practice may increase awareness and general acceptance of the concept of ACP. There are likely to be barriers to implementing this new way of working, for example, parental criticism or scepticism and therefore no funding.
Recognition of limitations of this review
A limitation of this review is that not all papers were retrievable with the authors undergraduate access clearance. If the author were to start this review again, he would have conducted a scoping review to narrow down the keywords and Boolean phrases used which would in turn increase dependability of the review.
Cite This Work
To export a reference to this article please select a referencing stye below:
Related Services
View all


Related Content
All TagsContent relating to: "Nursing"
Nursing involves providing care for people and families, whether that be during bad physical or mental health, illness or injury. Nurses are compassionate and empathetic, supporting people during their time of need.
Related Articles

DMCA / Removal Request
If you are the original writer of this dissertation and no longer wish to have your work published on the UKDiss.com website then please: