Do Psychopaths Have Abnormal Brains?
Info: 9257 words (37 pages) Dissertation
Published: 28th Feb 2022
Tagged: PsychologyNeurology
Abstract
The neurobiology concept behind psychopathy has not been fully understood as of yet. There are very few studies that examine the structural and function of the brain in psychopaths. The aim of this article is to review the research on the neurodevelopment of psychopaths in order understand the biology behind psychopathy a bit clearer. The studies report a reduction in grey matter in the prefrontal and temporal cortex; dysfunction in the ventromedial prefrontal cortex; reduction in the bilateral amygdala volume; reduction of activity in the amygdala and a reduction of white matter in the corpus callosum. These results indicate an association between psychopathy and brain abnormalities in the prefrontal-temporo-limbic system which are areas that deal with emotional and learning processes as well as others. Although, the research indicates that psychopaths do have abnormal brains, a definite conclusion cannot be given without further research.
Keywords: Psychopathy, Frontal lobe, Temporal Lobe, Amygdala, Corpus Callosum, Brain Abnormalities
Introduction
Psychopathy is a subtype of a personality disorder. About 1% of the population are psychopaths. The concept of psychopathy came from Philippe Pine in the 19th century who was one of the founding fathers of modern psychiatry. He described a group of patients who were suffering from mania sans délire (insanity without delirium). They did not have any intellectual problems but they lacked moral and behavioural control due to cruelty, antisocial acts, alcohol and drug abuse (Kiehl and Lushing, 2014). Hervey Cleckley made a highly influential contribution with his book The Mask of Sanity in 1976. He described psychopathy as a mixture of interpersonal, affective and behavioural features and he expresses that psychopaths do not usually have signs or symptoms that many people associate with psychopathy. Not all of them hear voices or have delusions for example. Cleckley explains that psychopaths are able to appear normal but have a mental disorder that is hidden by a ‘mask’. He observes that psychopaths appear to be friendly and easy to talk to. He also explains that psychopaths tend to be highly intelligent and able to fool others easily with the way they say things but not necessarily what they say. Due to being able to appear normal, they are more dangerous than those who have been diagnosed with severe mental illnesses because their personality disorder is hidden (Moscovici, 2011).
It was Dr Robert Hare that developed a test for psychopathy in 1980 which was released to the public in 1991. This became the ‘gold standard’ used by the justice system, researchers and forensic psychiatrists to identify the traits and behaviours of psychopaths. This was called the PCL-R (psychopathy check list- revised) or The Hare as it is sometimes known (Egan, 2016). Hare created a 20 item checklist for the test. Each item is given a score: 0 if it does not apply to the person; 1 if it partially applies and 2 if it fully applies. The list includes: glibness and superficial charm, grandiose sense of self-worth, pathological lying, cunning/manipulative, lack of remorse, emotional shallowness, callousness and lack of empathy, failure to accept responsibility for actions, a tendency to boredom, a parasitic lifestyle, a lack of realistic long-term goals, impulsivity, irresponsibility, lack of behavioural control, behavioural problems in early life, juvenile delinquency, criminal versatility, a history of “revocation of conditional release” ( broken parole for example), multiple marriages, and promiscuous sexual behaviour. A score of 30 or above would qualify for a psychopath diagnosis. The average ‘normal’ person typically scores less than 5 and the average score for prisoners is 23 (Egan, 2016)
Many researchers and psychologists share the belief that psychopathy is a neurodevelopmental disorder. Kent Kiehl, who completed his masters and doctorate in Hares’ lab, is one of them. He has analysed over 5000 brains by travelling to local prisons with an fMRI (Functional magnetic resonance imaging) machine and introducing the inmates to violent and neutral words and imagery. Kiehl found that emotions, impulse control and cognition in psychopaths are affected by structural and functional abnormalities in the brain. The amygdala plays a role in the emotional processes and therefore, any abnormalities can be associated with psychopathy. This was confirmed in two neuroimaging studies (Blair, 2003). In the first study, Tiihonen and colleagues (2000) used an MRI to compare the relationship between the volume of amygdala and psychopathy in violent offenders. They concluded that reduced volumes of amygdala were associated with high levels of psychopathy. The second study was by Kiehl (2001) who came to the same conclusion. The frontal lobe is also linked with behavioural changes and psychopathy. An example of behavioural change is from Phineas Gage when after an accident, suffered damage to the frontal lobe. This caused a personality change even though other areas remained intact (speech, movement, intelligence etc). It was only after his death that this cause was suggested (Damasio et al., 1994).
Another suggestion is that the cause of psychopathy originates from a person’s childhood. The ability to both empathise and deceive is developed around the age of four. However, people who have personality disorders do not develop this and it is thought that this is from traumatic experiences or by how they are treated by adults for example through abuse or neglect. Craparo, Schimmenti, and Caretti (2013) did a study on the childhood background on criminal offenders in Italy. The results showed that there was more neglect or abuse as a child in offenders who obtained high scores in the PCL-R checklist. Therefore, they concluded that childhood trauma can lead to the development of psychopathic traits. This was consistent with a previous study in 1996 which looked at psychopathy and violence in young adults who had been abused and neglected. An experimental group of 652 individuals were compared against a matched control group of 489 individuals. The experimental group had higher PCL-R scores than the control group. These results showed a connection been childhood abuse and neglect and psychopathy (Weiler and Widom, 1996).
Chivers (2014) explains that, even though it is said that 1% of the population are psychopaths, not all of them will go on to commit crimes. Some end up having highly successful careers such as CEO’s and professional athletes due to their glibness and charm. Therefore, the justice system cannot pre-emptively punish someone just because they display psychopathy traits and behaviours as it is impossible to predict whether someone will commit a crime. Once a person has overstepped that boundary and committed a crime, then it is easier to predict the likelihood of them reoffending.
Theories of Psychopathy
There are two main theories that researchers believe explain psychopathy. The first theory is the somatic marker hypothesis proposed by Antonio Damasio (1994). He suggested that emotional processes play a role in decision making. It was Phineas Gage whose accident first provided evidence that the frontal lobe is associated with making decisions. Therefore, damage to this area (mainly the prefrontal cortex) reduces the ability to do that. It was found that individuals with prefrontal damage are also unable to express appropriate emotions. These are traits of psychopathy and it led to Damasio’s theory. He defined emotions as an assortment of changes in the body activated by the brains response to a stimulus. Eventually, emotions and their corresponding change in the body (somatic marker) become associated with the outcomes from a past situation. Therefore, if that situation were to happen again in the future, the body influences decision making in favour for a particular behaviour. For example, if in the past, a situation resulted in a positive emotion or somatic marker leaving the individual feeling happy, the brain is more likely to pursue that behaviour. It could also work in the opposite way. For example, if a past situation left the individual feeling unhappy or sad, the brain is more likely to oppose that behaviour in a similar future situation. (Bechara and Damasio, 2005). The associated link between the somatic marker theory and psychopathy was suggested in the Iowa gambling task study that examined the somatic markers in individuals with varying degrees of psychopathy. It was found that psychopaths who had a high PCL-R score had the same gambling behaviour as individuals with lesions on their frontal cortex (van Honk et al., 2002).
The second theory of the cause of psychopathy is the violence inhibition mechanism proposed by Blair. It is based on research done by Eibl-Eibesfeldt and Lorenz. Their theory was that animals are able to control violence from developed mechanisms (Weber et al., 2008). An example of this is when an aggressive dog stops fighting when its opponent bares its throat. It is believed that the violence inhibition mechanism is similar in humans and it is thought to be activated by distress signals. The main neurological area for this theory is the amygdala (Blair, 2001). Therefore, any abnormalities may result in a reduction in the ability to empathise (Weber et al., 2008). The violence inhibition mechanism is supported by serval studies. One study looked at the recognition of emotion in facial expressions in children with psychopathic features. There were 37 children in the study between the ages 9 and 15 years old from a school for children with behavioural problems. The results showed that children with psychopathic traits showed difficulties in recognising both sad and fearful facial expressions (Stevens, Charman and Blair, 2001).
The History of Neuroimaging and Brain Mapping
The oldest data known for brain mapping has come from lesions in people from trauma or diseases. There are three famous cases: Phineas Gage, Tan and H.M. It was Tan who lead to the understanding of the localisation of language skills when damage to the left frontal cortex left caused the loss of his language. However, the most famous patient was H.M when a bilateral medial temporal lobectomy caused permanent amnesia to new information. Savoy continues on to explain that, although evidence from patients for brain mapping continues to be a source of important information, the MRI (Magnetic Resonance Imaging) gives better information on the extent of diseases and trauma (Savoy 2001).
Functional MRI (fMRI) was developed in 1990 to detect and map blood oxygenation changes in the brain. The patients are subjected to stimuli (words, picture, videos etc.) and any regions that are stimulated are mapped and compared with brains in a resting state. It has proven useful in psychopathy in particular. The first study using the fMRI in criminal psychopaths was published in 2001 (Kiehl and Kofman 2011). This study from Kiehl and colleagues in 2001 was used to examine the process of emotions in criminal psychopaths during memory tasks. They used eight psychopaths, eight non-psychopaths from a maximum-security prison and eight healthy control participants from the public. The PCL-R from Hare was used to differentiate the inmates between psychopaths and non-psychopaths. The results show that criminal psychopathy is related to abnormalities in the brain mostly in the limbic system and frontal cortex structures.
Another way of brain mapping is through using electroencephalography (EEG) which is non-invasive and it is used extensively in neurological disorders. It can either be used to measure the continuous electrical signals (brain waves) or to record the responses from a stimulus. These are called event related potentials. An advantage of the EEG is that is has excellent temporal resolution however, it is not very sufficient in producing three-dimensional spatial localisation (Savoy, 2001). According to Tudor and Tudor (2005), the EEG was discovered by a German psychiatrist, Hans Berger in 1929. The first use of the EEG was on 6th July 1929 during a neurosurgical operation on a 17 year old. This became a massive breakthrough for the advancement of neuroscience.
Electroencephalography
A study by Calzada-Reyes and colleagues in 2012 compares EEG abnormalities in both psychopaths and non-psychopaths. They used 58 violent male offenders from a prison in Havana City. From using the PCL-R test, 31 of the offenders were psychopaths (experimental group) and the other 28 were non-psychopaths (control group). They gave each offender a questionnaire about their drug use, alcohol use which is shown in the table below:
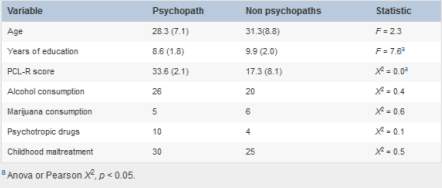
Table 1: showing environmental factors of both experimental and control group variables (Calzada-Reyes et al., 2012)
This shows that the experimental group (psychopaths) tend to have more alcohol and psychotropic drugs consumption. Furthermore, 55 of the offenders (30 psychopaths and 25 non-psychopaths) were subjected to childhood maltreatment. The EEG was recorded continuously and all participants were asked to stay relaxed, so that signals from movements were minimised.
The results show that, even though there were no significant differences found in the visual inspection of the EEG, the QEEG showed increased levels of beta activity on the left parieto-temporal regions of the brain and the bilateral occipital areas in the psychopath group. This was confirmed using LORETA. A low level of alpha activity on the left centro-temporal and parieto-central was also observed in the psychopath group compared to the control. This study indicates that the abnormalities in the fronto-temporo-limbic system contribute to the idea that neurodevelopment disorders are a cause of psychopathy (Calzada-Reyes et al., 2012).
Functional MRI
In 2003, Müller and colleagues used an fMRI to study the brain activation in psychopaths with the use of positive and negative images. They used a control group which consisted of six healthy men with no history of neuropsychiatric disorders. The experimental group were six male psychopathic patients from a high-security psychiatric facility. Images were used to assess the emotional process. Positive examples included ice cream, happy couples, puppies’ etc. neutral images included books, buildings, cutlery and negative images included bones, wounded people and aggressive animals/faces. The fMRI was used on a 1.5 Tesla MRI system with a 25-mT-gradient system with a head coil to measure the blood oxygen level dependant contrast (BOLD).
The results show that positive images increased the activation bilaterally in the fusiform cortex, the parietal cortex, the cerebellar hemispheres, the temporal and precentral cortex, and unilaterally left-sided in the gyrus frontalis inferior in psychopaths. There was also a reduction bilaterally in the occipital cortex and unilaterally right-sided in the medial frontal gyrus and medial temporal gyrus. The image below shows this (increased activation in blue and reduction in red).
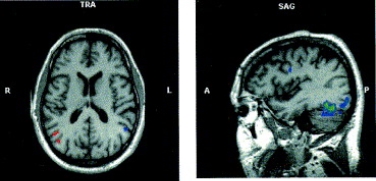
Figure 1: brain scan showing the differences in positive emotion processes. These show the regions of interest where there is an increased activation (blue) when compared to the control group (red) (Müller et al., 2003).
There was an increase in activation bilaterally in the medial temporal gyrus, occipital and the parietal cortex. It was also found bilaterally on the left side in the precentral cortex and the superior temporal gyrus. There was an increase on the right side in the inferior and medial frontal gyrus, the anterior cingulate and the amygdala. This is shown in blue on the image below. A reduction in activation was found unilaterally on the right side in the subgenual cingulate, the medial temporal gyrus and the gyrus fusiformis. It was also found unilaterally on the left side in the lobulus paracentralis, the dorsal cingulate, and the parahippocampal gyrus (Müller et al., 2003). This is shown in red.
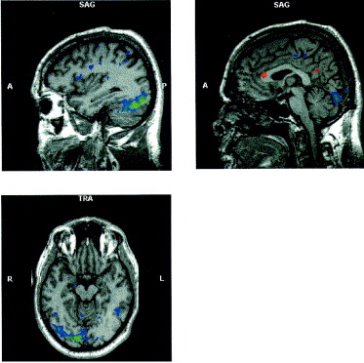
Figure 2: brain scan showing the differences in how emotions are processed from negative emotions in psychopaths. The regions of interest show an increased activation in psychopaths (blue) when compared to the control group (red) (Müller et al., 2003).
The conclusion of this study stated that there were increases and reductions in activation in the emotional-related sections of the brain from the stimuli. These differences were significantly different when compared with the healthy control group. This indicates that neurodevelopment plays a role in psychopathy.
The Prefrontal Cortex in Psychopathy
The frontal lobe is responsible for planning, decision making and cognition.
Many researchers believe that damage to the frontal cortex plays a role in psychopathy. A famous case in which damage to the prefrontal cortex caused a personality change was that of Phineas Gage (as mentioned earlier). Before the accident, he was trustworthy and dependable. However, the damage to his prefrontal cortex (PFC) resulted in him becoming disrespectful, unreliable and impulsive which are traits of psychopathy. Since this case, there have been studies researching the link between prefrontal damage (mainly ventromedial and orbitofrontal) and a lack in social behaviour and decision making (Hajak et al., 2008).
There have been several studies looking at the grey matter structure in the PFC. One study by Yang et al, uses three types of participants: 16 unsuccessful psychopaths (one conviction or more); 13 successful psychopaths (no convictions) and 23 non-psychopaths as a control group to compare against. It was found that the unsuccessful psychopaths had a lower PFC volume compared with the successful psychopaths and the control group. However, there was no significant difference in PFC volume when the successful psychopaths and control group were compared. In another study by Yang and colleagues, the regional cortical thickness was examined in 27 psychopathic participants and 32 non-psychopathic, healthy individuals. They were matched for age, gender and substance abuse. The results showed that psychopathic group had a reduced thickness in the PFC compared to the control group. It was found that there was thinning in the grey matter in the right frontal and temporal cortices. These results were consistent with the suggestion that grey matter volume is linked to psychopathy. One of the largest studies done was by Ermer and colleagues in 2011. 254 men from a prison were examined using voxel-based morphometry and multiple regression analysis to look at the relationship between the severity of psychopathy and the grey matter structure. The results showed a negative correlation between the PCL-R checklist and the grey matter volume/concentration (Koenigs, 2012).
In 2002, Laakso and colleagues investigated the correlation between prefrontal volume and psychopathy. It was found that people with an antisocial behaviour had smaller left dorsolateral, medial frontal and orbitofrontal cortices. However, this was not controlled for education and alcohol abuse. Therefore, once these were controlled, there were no significant differences. The results of prefrontal volume in psychopathy were rejected in this study (Hajak et al., 2008).
One study compared the abnormal ventromedial prefrontal cortex in children who have psychopathic traits in reversal learning. Children who have attention-deficit/hyperactivity disorders (ADHD) or oppositional defiant disorders (ODD) have increased aggressiveness and antisocial behaviours. A small group of these children also show traits of psychopathy such as lack of guilt and or remorse. Reversal learning is where an individual learns to respond to stimuli to gain a reward. Once the response is learned, there is no reward, therefore, they must learn to respond to new stimuli to gain that reward. It is thought that individuals with psychopathic traits are not able to do this. The cause of this impairment is believed to be from lesions on the orbital and PFC and it is suggested that the dorsal medial PFC is activated in conflict related situations and then the ventrolateral PFC responds. Recent studies in neuroimaging and lesion data have indicated that dysfunction in the ventromedial PFC causes an impairment in reversal learning in children and adults that display psychopathic traits. The fMRI was used to examine whether impairments in the reversal learning in children who exhibit psychopathic traits is from dysfunction in the ventromedial PFC or ventrolateral PFC. They also examined a group of children who had ADHD but showed no signs of psychopathic traits and a group of healthy children who had neither ADHD or psychopathic traits as a control group. The results from this study show that there were abnormalities in the ventromedial PFC in children with psychopathic traits. There was no evidence of any dysfunction in either the ventrolateral or dorsomedial PFC (Finger et al., 2008). All but one of the studies mentioned suggest that the prefrontal cortex plays a vital role in psychopathy.
The Amygdala in Psychopathy
The amygdala is involved in emotion processing and is important for the understanding of the severe aggression. It is also important for reward learning, social interaction and moral reasoning (Yang et al., 2009).
Impairment to the amygdala is another suggestion for a cause of psychopathy. The damage can result in individuals having problems with noticing distress cues in others or establishing fear responses (Pardini et al., 2014).
In one of the first studies in this area, the localisation of deformations in the amygdala in psychopaths was compared. They used 86 participants from Los Angeles in California and a group of these showed high rates of psychopathy. Psychopathy was again established using the PCL-R test. The results showed that 27 of these participants were psychopaths with a score of 23 or higher on the PCL-R test. 32 non-psychopaths were used as a control with a score of 15 or lower. MRI analysis was used to examine the amygdala. It was found that there was a decrease in the bilateral amygdala volume in the psychopathic individuals compared with the control group. The results showed that the reductions were mostly found in the basolateral, lateral, cortical and central nuclei of the amygdala. This study suggests that the amygdala is one of the key elements in what makes a psychopath. These results are also consistent with earlier studies examining lesions on the amygdala which show that damage to the amygdala is a cause of emotional impairments which is a trait of psychopathy (Yang et al., 2009). This was further researched by Pardini and colleagues in 2014. Reduced amygdala volumes in male participants were examined and whether it had caused a history of aggression or psychopathic traits in childhood. They also looked at whether the reduction in amygdala volume would have an impact in the future with increasing the risk violence. 503 males were initially chosen from Pittsburgh Youth Study (PYS) in 1986-87 in a longitudinal study. 56 of the 503 males were then chosen when they were 26 years old with varying degrees of violent histories: chronic serious violence; transient serious violence and no violence. The amygdala volume and degree of aggression were examined using automated segmentation. The results showed no significant difference between amygdala volume and the men grouped based on prior serious violence. However, men who had showed more aggressive behaviour and psychopathic traits between childhood and early adulthood had lower amygdala volumes. This also suggested that men with reduced amygdala volumes were more likely to commit violence in the future.
This was the first study to compare the amygdala volume and features of aggression and psychopathic traits from childhood to adulthood.
Another study looks at moral decision making in psychopaths. It is believed that emotion plays a part in moral decision making and activates the activity in the amygdala. An fMRI and moral dilemmas were used to examine the relationship between psychopaths and their brain activity. 17 volunteers from a community with different levels of psychopathy made judgements on ten situations based on the following types:
1) moral personal – emotion provoking (for example, should a baby be smothered to protect themselves and other people from a terrorist)
2) moral impersonal – less emotional (for example, should money found in a lost wallet be kept)
3) non-moral (for example, what transport is best to take – bus or train).
The levels of psychopathy ranged from 7.4 to 32 on the PCL-R test with 32 showing a high degree of psychopathy.
It was found that the participants who scored higher on the PCL-R test showed more of a reduction in activity in the amygdala during emotional moral decision-making. There was also reduced activity in the medial prefrontal cortex, posterior cingulate and angular gyrus. This is consistent with the hypothesis that the function of the amygdala is disrupted during moral decision-making in psychopaths. It is shown in all traits of psychopathy which highly suggests that abnormalities to the amygdala could play a vital role in psychopathy (Glenn, Raine and Schug, 2009).
Fear recognition in child psychopathy was examined by Dadds and colleagues in 2006. The failure to recognise fear appears both in psychopathy and patients with damage to the amygdala. This, therefore, adds to the theory that amygdala abnormalities are associated with psychopathy. This study looked at whether fear recognition deficits occur in children with psychopathic traits and whether they could be modified. The first experiment was comprised of 33 boys aged 8 to 15 years and the second experiment of 65 boys aged 9 to 17 years. The participants were from schools in Sydney, Australia. This study found that the failure to recognise fear is from the failure to visualise the eye region of other people’s faces. This can be modified by directing their attention to the eye region. This is one of the first studies to show this modification. However, it was noted that Richell and colleagues in 2003 found that individuals with psychopathic traits could identify emotions on faces through stimulus faces that were cut so to only show information from the eye region.
The Temporal Lobe in Psychopathy
The temporal lobe is involved in the sensory input, language and memory. The medial temporal lobe contains the hippocampus which is involved in short term memory.
It is believed that one possible cause of psychopathy is related to abnormalities in language skills. Research has shown that damage to language processes is more noticeable when psychopaths are asked to perform semantic processing tasks. One theory is that psychopathic individuals show difficulties processing abstract words. Concrete words are words that can be perceived with the five senses (touch, smell, sight, taste and hearing) as abstract words refer to actions, emotions and ideas. Kiehl et al (1999) noted event-related potential (ERP) data which showed that psychopaths were unable to distinguish between concrete and abstract words. This suggested that the frontal-temporal lobes were involved in the difficulty for psychopathic individuals to differentiate between the words.
One study uses an fMRI to examine temporal lobe abnormalities in criminal psychopaths. Eight psychopathic inmates (male) were used from a maximum security prison in Canada. The level of psychopathy was examined using the PCL-R test with the control group showing no psychopathic traits. There were no differences in age, education, or parental socioeconomic status and no substance abuse in the last six months before the study. For this study, stimulus words were chosen that were either concrete or abstract and showed no emotional meaning. The results were consistent with the hypothesis: compared to a control group; psychopathic individuals were significantly slower at understanding abstract words. The psychopathic experimental group showed difficulties in activating the right anterior superior temporal gyrus when processing abstract words. These findings were also consistent with previous research (Kiehl et al 2004).
This was further validated in a study by Hajak and colleagues in 2008. 17 psychopathic participants were compared against 17 healthy controls. All participants were male of a similar age with no substance abuse in the last six months prior to the study. The voxel-based morphometry (VBM) showed a reduced grey matter volume in the right and left superior temporal gyrus in psychopaths compared against the control group. This is shown in the figure below:
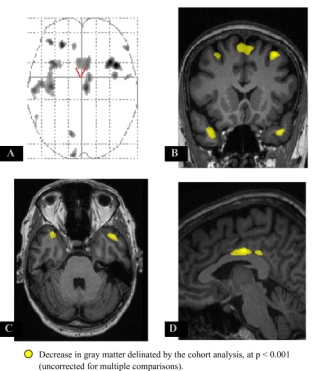
Figure 3: This shows there are structural differences in grey matter between psychopaths when compared to a control group. The reduction in grey matter is shown in yellow. A: glass brain. B: significant grey matter reduction in the premotor cortex and temporal lobes bilaterally. C: Significant grey matter reduction in the temporal lobes bilaterally. D: significant grey matter reduction in the right middle cingulate gyrus (Hajak et al., 2008).
It was found that the temporal cortex has a significant involvement in psychopathy.
Other behavioural studies have examined patients with temporal lobe epilepsy who show some traits of psychopathy. When the dysfunctional temporal lobe was removed, the patients’ hostility is reduced and the social relationships improve. This, along with other studies, is consistent with the theory that abnormalities in the medial and anterior temporal lobe play a significant role in psychopathy (Kiehl et al., 2006). A study in 2001 examines the association between psychopathy and the posterior hippocampus which is located in the temporal lobe. 18 male participants were studied all who had been convicted of various violent offences. All of them had at least one personality disorder and had been dependent on alcohol. An MRI was used in this study and the results showed a negative correlation between the volumes in the hippocampus and the PCL-R scores. This suggests that there may be an association between the hippocampus and psychopathy and it is also believed that the results in this study could provide some evidence towards the somatic marker theory (Laakso et al., 2001).
Corpus Callosum in Psychopathy
The corpus callosum is made up of axons and connects the right and left hemisphere of the brain. It contains white matter which allows the different structures of the brain to communicate with each other (Mooshagian, 2008). Although there has not been much research into the structure of the corpus callosum and its involvement in psychopathy, it is believed that some violent and anti-social offenders have functional abnormalities. One study compares the structure of the corpus callosum and the white matter in psychopaths and a control group. It also looks at whether the abnormalities are associated with an emotional deficit which is a psychopathic trait. 15 psychopaths were used as participants and 25 as a control. They were selected from five temporary employment agencies which allowed the experimental group to be demographically matched to the control. The white matter length, thickness and volume of the corpus callosum were measured using an MRI. The results showed that, when compared to the control group, the experimental group had a 22.6% increase in the volume of white matter. The white matter length was also 6.9% longer in the experimental group and 15.3% thinner compared to the control. Furthermore, after substance abuse was controlled, the callosal structure abnormalities were still present. This suggests that psychopathy could be neurodevelopmental (Raine et al., 2003). Recent studies have also used transcranial magnetic stimulation (TMS) to examine the association between the corpus callosum and aggression. The TMS measures the effectiveness of connectivity between the two hemispheres by analysing the signal transfer. It was found that there were higher signals between the right and the left side of the brain in psychopaths when compared to a control group. It suggests a reduced response in the right cerebral hemisphere in psychopathic individuals with aggressive tendencies (Schutter and Harmon-Jones, 2013). These results indicate an association between aggression and the corpus callosum which could be linked with psychopathy as one of the features is aggression.
Biochemistry of Psychopathy
Another possible cause of psychopathy could be through biochemistry. These are the chemical processes that occur in the living organisms. It is believed that monoamine oxidase (MAO) is associated with psychopathy. This is a chemical that is widely spread around the human body through blood platelets. There have been a few studies which relate low platelet MAO to personality disorders however; the relationship is still unclear (Lidberg et al., 1985). A study by Lidberg examines the platelet MAO activity in psychopaths. He examined 37 male subjects between the ages 23-62 years from a forensic psychiatry clinic in Stockholm against a control group. Blood samples were taken at the same time every day and then analysed for MAO activity. The results showed that the psychopathic group had a very low level of MAO activity which was expected as personality disorders are found in psychopathy.
Another study looked at the glucose metabolism in the prefrontal cortex. 22 participants who were accused of murder but pleaded not guilty by reason of insanity were compared against a control group who matched age and gender. The results showed that the murderers had significantly reduced glucose metabolism in the prefrontal cortex. There were no significant differences in the posterior frontal and temporal lobes which suggests it is localised to the prefrontal cortex, though further studies are required (Raine et al., 1994).
Discussion
It is believed by many researchers that abnormalities in the brain play an important role in psychopathy. Some studies have looked into structural and functional abnormalities mainly in the frontal lobe; amygdala, temporal lobe and corpus callosum and most researchers have arrived at the same conclusion. However, the connection between neurodevelopment disorders and psychopathy has not been fully understood as of yet and there are several improvements to be made in future studies.
The research that has been mentioned in this review suggests that the prefrontal–temporo-limbic system is involved in the development of psychopathy, both structurally and functionally. Overall it was found that the prefrontal and temporal cortex have a reduction in grey matter in psychopaths when compared to a control group. The amygdala is also believed to be involved in the cause of psychopathy and this has been suggested by several studies. The results showed that there were reductions in the basolateral, lateral, cortical and central nuclei of the amygdala in psychopaths. Other studies in this area also suggested that impairment to the amygdala which results in difficulties with emotion processing could also be a cause. This is because impairment to emotion processing is one of features of psychopathy. Even though the corpus callosum is believed to be associated with psychopathy, further research is required. It is worth noting, however, that the results from the study by Raine and colleagues (2003) suggests there is some involvement and this can act as a basis for future research in this area. His study examines the structure of the white matter and although this requires more research, it may also be important to examine the function and its association with psychopathy if any. Studies on the temporal lobe also suggest that it plays a vital role. It was found that there were functional deficits when a group of psychopaths were shown concrete and abstract words compared to a control group. They showed difficulties in activating the right anterior superior temporal gyrus when processing abstract words. This was also consistent with a previous study by Kiehl et al.
There have been a few studies on the biochemistry behind psychopathy, for example monoamine oxidase. It has been suggested there is an association between them. However, this also requires further research and there have not been many recent studies around it since 1980. The studies seem to suggest that there is not just one neurobiological cause to psychopathy but a series of brain abnormalities that are connected. Weber et al (2008) explains that amygdala deficits are found in psychopathic adults and children with psychopathic traits but it is believed that when completing tasks, the orbitofrontal cortex is impaired in adults only. This could be evidence on the development in psychopaths however; it could also be due to substance abuse which is sometimes linked with psychopathy. Overall, the research suggests that brain abnormalities are associated with psychopathy.
However, there are some methodological challenges which are important to consider when looking at neurobiological studies of psychopathy. One of the main problems is the definition of a psychopath. This is determined by the PCL- R test by Hare in most studies. However, there are a variety of cut off scores used by researchers. The standard cut off score is over 30 for psychopaths and under 20 for non-psychopaths. For example, Yang et al., (2009) has a cut off score of 23 of higher for the definition of a psychopath as Kiehl et al., (2004) has a cut off score of 28 or higher. This is due to the difficulty of finding individuals with high psychopathy scores above 30 in a forensic setting as explained by Koenigs (2012). It might be useful to set a slightly lower score as a cut off for everyone to follow to avoid any criticisms. Another methodological challenge is being able to gather a control group who match the experimental group in age, education and substance abuse history. These are important factors that could affect brain structure and function. An example of where this became important was in the study by Laakso and colleagues in 2002. The level of education and alcohol consumption was not controlled for in the initial experiment. Once these effects had been controlled, there were no significant differences between anti-social behaviour and prefrontal volume and therefore, the hypothesis was rejected. There are several studies, however, that do control the age, level of education and history of substance abuse and the results have shown a link between abnormalities in the brain and psychopathy. Therefore, even though the hypothesis by Laakso and colleagues were rejected, there is still an association between brain deficits and psychopathy.
Furthermore, it is not known in a few of the studies whether a control group was used and in most of the studies, the groups were of a small sample size. Although this allows for comparison with other studies that have used a similar sized group of participants, it does raise some doubt over whether the results are significant enough to support the theories. However, only it is believed only 1% of the population are psychopaths so it is difficult to find a large enough group for research. A lot of these studies are based on unsuccessful psychopaths (those who have been convicted); therefore, it is known whether the functional abnormalities are due to psychopathy or just physiological changes from being incarcerated.
In addition to this, there is relatively little research on female psychopathy and most of the research found has studied in males. This might be due to researchers assuming that the psychopathic features are transferable to women. It is believed that psychopathy is less common in females compared to males however; it is not known how the behavioural differences in psychopathy between the sexes are shown. Furthermore, there have been very few studies on how psychopathy is developed between men and women and if there are any significant differences (Wynn, Hoiseth and Pettersen, 2012). It may be possible for future studies to examine brain abnormalities in female psychopaths but with psychopathy being less common in women, it may be difficult.
Conclusion
In conclusion, the studies mentioned have suggested there is an association between brain abnormalities, mainly in the frontal and temporal cortex, amygdala and corpus callosum (the prefrontal–temporo-limbic circuit) and psychopathy. These abnormalities could be structural or functional. There are even some beliefs that the abnormalities are chemically which have been supported through a few studies. However, there is not enough research to make a clear, overall conclusion on whether psychopaths have abnormal brains or not. It is also worth mentioning that these brain regions also show deficits in individuals with other mental disorders, for example, schizophrenia. Further research is needed for a definite answer; however, the studies so far do support the theory that psychopaths have abnormal brains.
Bibliography
Bear, M., Connors, B. and Paradiso, M. (2016). Neuroscience. 4th ed. Philadelphia, Pa: Wolters Kluwer.
Bechara, A. and Damasio, A. (2005). The somatic marker hypothesis: A neural theory of economic decision. Games and Economic Behavior, [online] 52(2), pp.336-372. Available at: http://www.sciencedirect.com/science/article/pii/S0899825604001034 [Accessed 11 Apr. 2017].
Blair, J. (2003). Neurobiological basis of psychopathy. The British Journal of Psychiatry, [online] 182(1), pp.5-7. Available at: http://bjp.rcpsych.org/content/182/1/5 [Accessed 5 Feb. 2017].
Blair, R. (2001). ADVANCES IN NEUROPSYCHIATRY: Neurocognitive models of aggression, the antisocial personality disorders, and psychopathy. Journal of Neurology, Neurosurgery & Psychiatry, [online] 71(6), pp.727-731. Available at: http://jnnp.bmj.com/content/jnnp/71/6/727.full.pdf [Accessed 11 Apr. 2017].
Buchsbaum, M. (2004). Frontal Cortex Function. [online] Ajp.psychiatryonline.org. Available at: http://ajp.psychiatryonline.org/doi/pdf/10.1176/appi.ajp.161.12.2178 [Accessed 2 Apr. 2017].
Calzada-Reyes, A., Alvarez-Amador, A., Galán-García, L. and Valdés-Sosa, M. (2013). EEG abnormalities in psychopath and non-psychopath violent offenders. Journal of Forensic and Legal Medicine, [online] 20(1), pp.19-26. Available at: http://www.jflmjournal.org/article/S1752-928X(12)00100-X/pdf [Accessed 11 Feb. 2017].
Caretti, V., Schimmenti, A. and Craparo, G. (2013). Traumatic experiences in childhood and psychopathy: A study on a sample of violent offenders from Italy. European Journal of Psychotraumatology, [online] 4. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3871837/ [Accessed 24 Jan. 2017].
Chivers, T. (2014). Psychopaths: How can you spot one?. The Telegraph. [online] Available at: http://www.telegraph.co.uk/culture/books/10737827/Psychopaths-how-can-you-spot-one.html [Accessed 20 Dec. 2016].
Dadds, M., Perry, Y., Hawes, D., Merz, S., Riddell, A., Haines, D., Solak, E. and Abeygunawardane, A. (2006). Attention to the eyes and fear-recognition deficits in child psychopathy. The British Journal of Psychiatry, [online] 189(3), pp.280-281. Available at: http://bjp.rcpsych.org/content/189/3/280 [Accessed 3 Apr. 2017].
Damasio, A., Galaburda, A., Frank, R., Grabowski, T. and Damasio, H. (1994). The Return of Phineas Gage: Clues About the Brain from the Skull of a Famous Patient. Science, [online] 264(5162), pp.1102-1105. Available at: http://www.antoniocasella.eu/dnlaw/Damasio_1994.pdf [Accessed 20 Jan. 2017].
Egan, D. (2016). Into the mind of a psychopath. Discover Magazine. [online] Available at: http://discovermagazine.com/2016/june/12-psychopath-and-the-hare [Accessed 20 Dec. 2016].
Ferracuti, S., Girardi, P., Tatarelli, R., De Rossi, P., Criscuolo, S., Di Cesare, G., Alessi, M., Di Pietro, S., Rapinesi, C., Kotzalidis, G. and Del Casale, A. (2015). Functional Neuroimaging in Psychopathy. Neuropsychobiology, [online] 72(2). Available at: https://www.karger.com/Article/FullText/441189 [Accessed 21 Jan. 2017].
Finger, E., Marsh, A., Mitchell, D., Reid, M., Sims, C., Budhani, S., Kosson, D., Chen, G., Towbin, K., Leibenluft, E., Pine, D. and Blair, J. (2008). Abnormal Ventromedial Prefrontal Cortex Function in Children With Psychopathic Traits During Reversal Learning. Archives of General Psychiatry, [online] 65(5), p.586. Available at: http://jamanetwork.com/journals/jamapsychiatry/fullarticle/482697 [Accessed 27 Mar. 2017].
Glenn, A., Raine, A. and Schug, R. (2009). The neural correlates of moral decision-making in psychopathy. Molecular Psychiatry, [online] 14(1), pp.5-6. Available at: http://repository.upenn.edu/cgi/viewcontent.cgi?article=1058&context=neuroethics_pubs [Accessed 4 Apr. 2017].
Hajak, G., Klein, H., Schuierer, G., Röder, C., Taschler, H., Lange, K., Wagner, V., Sommer, M. and Müller, J. (2003). Abnormalities in emotion processing within cortical and subcortical regions in criminal psychopaths. Biological Psychiatry, [online] 54(2), pp.152–162. Available at: http://www.sciencedirect.com/science/article/pii/S0006322302017493 [Accessed 15 Feb. 2017].
Hajak, G., Schmidt-Wilcke, T., Weber, T., Döhnel, K., Sommer, M., Gänßbauer, S. and Müller, J. (2008). Gray matter changes in right superior temporal gyrus in criminal psychopaths. Evidence from voxel-based morphometry. Psychiatry Research: Neuroimaging, [online] 163(3), pp.213–222. Available at: http://www.sciencedirect.com/science/article/pii/S0925492707001709 [Accessed 11 Jan. 2017].
Hoffman, M. and Kiehl, K. (2011). THE CRIMINAL PSYCHOPATH: HISTORY, NEUROSCIENCE, TREATMENT, AND ECONOMICS. Jurimetrics, [online] 51, pp.355-397. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4059069/ [Accessed 21 Jan. 2017].
Kiehl, K., Bates, A., Laurens, K., Hare, R. and Liddle, P. (2006). Brain potentials implicate temporal lobe abnormalities in criminal psychopaths. Journal of Abnormal Psychology, [online] 115(3), pp.443-453. Available at: http://www.nrc-iol.org/cores/ccnlab/publications/kiehl_et_al_nn_021104.pdf [Accessed 3 Apr. 2017].
Kiehl, K., Harenski, C., Chen, C. and Decety, J. (2013). An fMRI study of affective perspective taking in individuals with psychopathy: Imagining another in pain does not evoke empathy. Frontiers in Human Neuroscience, [online] 7. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3782696/ [Accessed 21 Jan. 2017].
Kiehl, K., Smith, A., Mendrek, A., Forster, B., Hare, R. and Liddle, P. (2004). Temporal lobe abnormalities in semantic processing by criminal psychopaths as revealed by functional magnetic resonance imaging. Psychiatry Research: Neuroimaging, 130(1), pp.27-42.
Knight-Jadczyk, L. and Jadczyk, A. (1997). Hervey Cleckley: Discussion of Psychopathy traits. [online] Available at: http://www.cassiopaea.com/cassiopaea/cleckley-mos.htm [Accessed 4 Dec. 2016].
Koenigs, M. (2012). The role of prefrontal cortex in psychopathy. Reviews in the Neurosciences, [online] 23(3). Available at: https://www.degruyter.com/view/j/revneuro.2012.23.issue-3/revneuro-2012-0036/revneuro-2012-0036.xml [Accessed 26 Mar. 2017].
Laakso, M., Gunning-Dixon, F., Vaurio, O., Repo-Tiihonen, E., Soininen, H. and Tiihonen, J. (2002). Prefrontal volumes in habitually violent subjects with antisocial personality disorder and type 2 alcoholism. Psychiatry Research: Neuroimaging, [online] 114(2), pp.95-102. Available at: http://ac.els-cdn.com/S0925492702000057/1-s2.0-S0925492702000057-main.pdf?_tid=c5a37c72-1eff-11e7-99e1-00000aacb360&acdnat=1491947134_130d8c36faa48ba12f33ad286ecf510a [Accessed 11 Jan. 2017].
Laakso, M., Vaurio, O., Koivisto, E., Savolainen, L., Eronen, M., Aronen, H., Hakola, P., Repo, E., Soininen, H. and Tiihonen, J. (2001). Psychopathy and the posterior hippocampus. Behavioural Brain Research, [online] 118(2), pp.187-193. Available at: http://www.sciencedirect.com/science/article/pii/S0166432800003247 [Accessed 12 Apr. 2017].
Lidberg, L., Modin, I., Oreland, L., Tuck, J. and Gillner, A. (1985). Platelet monoamine oxidase activity and psychopathy. Psychiatry Research, [online] 16(4), pp.339-343. Available at: http://www.sciencedirect.com/science/article/pii/0165178185901258 [Accessed 12 Apr. 2017].
Liddle, P., Brink, J., Forster, B., Mendrek, A., Hare, R., Smith, A. and Kiehl, K. (2001). Limbic abnormalities in affective processing by criminal psychopaths as revealed by functional magnetic resonance imaging. Biological Psychiatry, [online] 50(9), pp.677–684. Available at: http://www.sciencedirect.com/science/article/pii/S0006322301012227 [Accessed 21 Jan. 2017].
Lushing, J. and Kiehl, K. (2014). Psychopathy. Scholarpedia, [online] 9(5), p.30835. Available at: http://www.scholarpedia.org/article/Psychopathy [Accessed 2 Dec. 2016].
Mooshagian, E. (2008). Anatomy of the Corpus Callosum Reveals Its Function. Journal of Neuroscience, [online] 28(7), pp.1535-1536. Available at: http://www.jneurosci.org/content/28/7/1535 [Accessed 3 Apr. 2017].
Moscovici, C. (2011). How do Psychopaths construct their mask of sanity?. [online] Available at: https://psychopathyawareness.wordpress.com/2011/01/19/how-do-psychopaths-construct-their-mask-of-sanity/ [Accessed 20 Dec. 2016].
Müller, J., Gänßbauer, S., Sommer, M., Döhnel, K., Weber, T., Schmidt-Wilcke, T. and Hajak, G. (2008). Gray matter changes in right superior temporal gyrus in criminal psychopaths. Evidence from voxel-based morphometry. Psychiatry Research: Neuroimaging, [online] 163(3), pp.213-222. Available at: http://www.sciencedirect.com/science/article/pii/S0925492707001709.
Neuroskills.com. (n.d.). Traumatic Brain Injury Resource Guide – Temporal Lobes. [online] Available at: http://www.neuroskills.com/brain-injury/temporal-lobes.php [Accessed 3 Apr. 2017].
Pardini, D., Raine, A., Erickson, K. and Loeber, R. (2014). Lower Amygdala Volume in Men is Associated with Childhood Aggression, Early Psychopathic Traits, and Future Violence. [online] Available at: http://www.sciencedirect.com/science/article/pii/S0006322313003120 [Accessed 28 Mar. 2017].
Raine, A., Buchsbaum, M., Stanley, J., Lottenberg, S., Abel, L. and Stoddard, J. (1994). Selective reductions in prefrontal glucose metabolism in murderers. Biological Psychiatry, [online] 36(6), pp.365-373. Available at: http://www.sciencedirect.com/science/article/pii/0006322394912114 [Accessed 12 Apr. 2017].
Raine, A., Lencz, T., Taylor, K., Hellige, J., Bihrle, S., Lacasse, L., Lee, M., Ishikawa, S. and Colletti, P. (2003). Corpus Callosum Abnormalities in Psychopathic Antisocial Individuals. Archives of General Psychiatry, [online] 60(11), p.1134. Available at: http://jamanetwork.com/journals/jamapsychiatry/fullarticle/207996 [Accessed 3 Apr. 2017].
Ryan, C. and BBC, (2003). What makes a psychopath?. BBC Health. [online] Available at: http://news.bbc.co.uk/1/hi/health/3116662.stm [Accessed 4 Dec. 2016].
Savoy, R. (2001). History and future directions of human brain mapping and functional neuroimaging. Acta Psychologica, [online] 107(s 1–3), pp.9–42. Available at: http://www.sciencedirect.com/science/article/pii/S000169180100018X [Accessed 20 Jan. 2017].
Schneider, F., Amunts, K., Habel, U. and Weber, S. (2008). Structural brain abnormalities in psychopaths—a review. Behavioral Sciences & the Law, 26(1), pp.7-28.
Schutter, D. and Harmon-Jones, E. (2013). The corpus callosum: A commissural road to anger and aggression. Neuroscience & Biobehavioral Reviews, [online] 37(10), pp.2481-2488. Available at: http://www.sciencedirect.com/science/article/pii/S014976341300184X [Accessed 12 Apr. 2017].
Stevens, D., Charman, T. and Blair, R. (2001). Recognition of Emotion in Facial Expressions and Vocal Tones in Children With Psychopathic Tendencies. The Journal of Genetic Psychology, [online] 162(2), pp.201-211. Available at: http://www.tandfonline.com/doi/pdf/10.1080/00221320109597961?needAccess=true&instName=Nottingham+Trent+University [Accessed 11 Apr. 2017].
Tudor, K. and Tudor, M. (2005). [Hans Berger (1873-1941)–the history of electroencephalography]. Acta medica Croatica : casopis Hravatske akademije medicinskih znanosti., [online] 59(4), pp.307-13. Available at: https://www.ncbi.nlm.nih.gov/pubmed/16334737 [Accessed 25 Jan. 2017].
Valdés-Sosa, M., Galán-García, L., Alvarez-Amador, A. and Calzada-Reyes, A. (2012). EEG abnormalities in psychopath and non-psychopath violent offenders. Journal of forensic and legal medicine., [online] 20(1), pp.19-26. Available at: https://www.ncbi.nlm.nih.gov/pubmed/23217372 [Accessed 25 Jan. 2017].
van Honk, J., Hermans, E., Putman, P., Montagne, B. and Schutter, D. (2002). Defective somatic markers in sub-clinical psychopathy. Neuroreport, [online] 13(8), pp.1025-1027. Available at: https://www.ncbi.nlm.nih.gov/pubmed/12060801 [Accessed 11 Apr. 2017].
Weber, S., Habel, U., Amunts, K. and Schneider, F. (2008). Structural brain abnormalities in psychopaths—a review. Behavioral Sciences & the Law, 26(1), pp.7-28.
Weiler, B. and Widom, C. (1996). Psychopathy and violent behaviour in abused and neglected young adults. Criminal Behaviour and Mental Health, [online] 6(3), pp.253-271. Available at: http://onlinelibrary.wiley.com/doi/10.1002/cbm.99/full [Accessed 12 Apr. 2017].
Wynn, R., Hoiseth, and Pettersen, G. (2012). Psychopathy in women: theoretical and clinical perspectives. International Journal of Women’s Health, [online] 4, p.257. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3379858/ [Accessed 12 Apr. 2017].
Yang, Y., Raine, A., Narr, K., Colletti, P. and Toga, A. (2009). Localization of Deformations Within the Amygdala in Individuals With Psychopathy. Archives of General Psychiatry, [online] 66(9), p.986. Available at: http://jamanetwork.com/journals/jamapsychiatry/fullarticle/210298 [Accessed 28 Mar. 2017].
Cite This Work
To export a reference to this article please select a referencing stye below:
Related Services
View all


Related Content
All TagsContent relating to: "Neurology"
Neurology is the specialist branch of medicine that deals with the treatment of disorders of the nervous system. This means that neurologists concern themselves with issues affecting the brain, the nerves, and the spinal cord.
Related Articles

DMCA / Removal Request
If you are the original writer of this dissertation and no longer wish to have your work published on the UKDiss.com website then please: