Bioprinting for Maxillofacial Repair
Info: 7753 words (31 pages) Dissertation
Published: 9th Dec 2019
Tagged: Medical Technology
1.0 Abstract
Maxillofacial defects are a major setback to a person’s life in terms of both well-being and appearance. Current techniques of repair for this condition have limitations and are often unethical in their use. A relatively new method of maxillofacial repair has come to light in the form of 3D bioprinting, which involves the reconstruction of organs/tissue, through 3D printing of biomaterials. This phenomenon has revolutionised this field of medicine and is rapidly growing for a number of reasons, including: advancements in technology, increased funding and elevating need for a solution. In this literature review, the bioprinting process will be explained as well as the different approaches, 3D printing methods, materials and challenges will be analysed and discussed. In addition, the current situation of bioprinting, in terms of clinical/commercial application, will be explained as well as prospects.
Table of Contents
- Abstract ………………………………………………………………………………. 1
- Introduction …………………………………………………………………………… 3
- Maxillofacial Trauma/Defects and Complications
- Current Techniques
- Bioprinting …………………………………………………………………………… 4
- Definition and Process
- Bioprinting Methods
- Inkjet Based
- Laser Assisted
- MicroExtrusion
- Stereolithography
- Biomaterials
- Scaffolds
- Challenges …………………………………………………………………………… 9
- Biological
- Technological
- Regulatory
- Ethical
- Clinical Application …………………………………………………………………. 11
- Conclusions and the Future …………………………………………………………. 11
- Acknowledgements …………………………………………………………………. 12
- References ……………………………………………………………………………. 12
2.0 Introduction
Maxillofacial repair is one of the most challenging subjects in today’s medicine. This is due to the complexity of the tissues present in the facial region and the vital functions that they are responsible for, such as seeing, chewing, speaking and protection (Zhang, et al., 2015). Several articles, such as Pagni et al (2012), Zhang et al (2015) and Datta et al (2017) all agree that craniofacial deformities cause significant clinical challenges when attempting to repair/reconstruct. There are techniques that have been used up to present that are not necessarily ethical or effective.
2.1 Maxillofacial Trauma/Defects and Complications
400,000 visits annually to accident and emergency are due to maxillofacial trauma (Radabaugh, et al., 2016). In addition to this, older people are more prone to fractures and soft tissue injuries, whilst younger people are more susceptible to dentialveolar trauma. The causes of injury include: sports, violence, traffic accidents and work accidents (Gassner, et al., 2003). This evidence shows that cranio-maxillofacial trauma is a rather common issue and can happen to anyone at any time. These abnormalities/defects can severely affect one’s aesthetics, function and psychosocial well-being. Due to the high complexity of tissue and immense impact on patient’s lives, researchers have found it challenging to develop new and improved techniques to tackle tissue repair and replacement in the face (Fong, et al., 2003). There appeared to be limited literature describing complications that develop in patients following maxillofacial trauma. These can be split into early/late and minor/major, however this categorisation is still under debate (Salentijn, et al., 2014).
2.2 Current Techniques
There are various techniques that have been used in the past to correct maxillofacial abnormalities and these techniques are still used in cases today, due to other, more efficient methods not being fully developed. Current techniques, however, have their flaws.
Autografting, which is the current ‘gold standard’ in maxillofacial reconstruction (Roseti, et al., 2017) involves taking bone or tissue from another part of the patient’s own body and using it to replace the bone or tissue that is damaged (DCI Donor Services Tissue Bank, 2017). For example, surgeons typically use hamstring tendon to repair anterior cruciate ligaments. There are several issues associated with this method including increased rehabilitation time, due to there being two or more body sites needing recovery, the tediousness of the harvesting process and of course the possibility of morbidity at the donor site of the patient (Visscher, et al., 2016). However, with technology and research developing every day and at a reasonable pace, surgeons have become increasingly more skilled in the autograft procedures and do what they must to potentially save a patient from long lasting pain or potentially death. A recent case was at the QE hospital in Birmingham, where a patient had a tumour attached to her upper jawbone, which would result in death. Surgeons removed the part of the upper jaw bone affected, along with the eye and replaced it with a graft from the patient’s hip bone (BBC2, 2018).
Allografts involves the same method as autograft, however the graft is obtained from another person (DCI Donor Services Tissue Bank, 2017). There are several advantages to this process over autografts, as several articles explain, mainly based around the abundant supply of the same tissue that had been damaged and the fact that there is only one body site that needs to be invaded on the patient, therefore decreasing recovery time and possible discomfort (Visscher, et al, 2016; Posnick, et al, 2015). Yet there are significant disadvantages to this method, including the unacceptance of the tissue and concerns of transmission of diseases, as well as ethical issues surrounding it (Visscher et al, 2016; Goldberg, et al, 1987).
Using metal constructs are also common practice for craniofacial surgery. Some materials, such as titanium are biocompatible and have very good strength-weight ratios. However, the manufacture of the complex structures is a challenge and time consuming, as well as the metals having low wear resistance and the risk of fatigue/fracture. (Visscher et al, 2016; Roseti et al, 2017)
Many articles related to current techniques all highlight the issues associated with them. There is a high rate of failure with these methods and the possibility of the body not accepting these foreign materials. (Gu et al, 2015; Fong et al, 2003; Bostrom & Mikos, 2002). Therefore, new, more advanced methods of maxillofacial repair are needed.
3.0 Bioprinting
From Fong, et al, 2003, due to impact on patient’s life from maxillofacial anomalies, researchers have struggled to develop new and improved methods of tissue regeneration. Now, a new strategy of maxillofacial repair, called bioprinting, is being developed and could have significant clinical benefits relating to this area of medicine.
3.1 Definition and Process
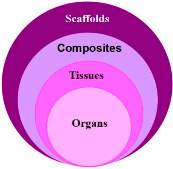 Bioprinting was originally defined as “organ printing” and a process that involved a computer-aided design model, converting it to an STL file, slicing and then printing (Mironov, et al., 2003). However, since then, different approaches have been developed for bioprinting and it is now applicable to other body components other than organs, such as bone, muscle, etc (An, et al., 2015). In more recent literatures, bioprinting can be defined as “layer by layer precise positioning of biological materials, biochemicals and living cells…to fabricate 3D structures” (Murphy & Atala, 2014); and many other authors back this up, such as Starly & Shirwaiker (2015, p.58), mentioning that it is the “automated deposition of biological molecules” and Bishop, et al (2017, p.186), describing it as “the precise layering of cells, biological scaffolds and biologic factors”. The complex 3D structures created can be either scaffolds, cell/biomaterial composites, homogeneous tissue and several tissue contained organs (Wang, et al., 2016) (Figure 1). When searching for literature for this review, it was discovered that the term ‘tissue engineering’ appeared frequently. This term is used to describe the process of combining engineering and life sciences to understand the relationship between structure and function, and development of biological replacements (O’Brien, 2011). Bioprinting is a form of tissue engineering.
Bioprinting was originally defined as “organ printing” and a process that involved a computer-aided design model, converting it to an STL file, slicing and then printing (Mironov, et al., 2003). However, since then, different approaches have been developed for bioprinting and it is now applicable to other body components other than organs, such as bone, muscle, etc (An, et al., 2015). In more recent literatures, bioprinting can be defined as “layer by layer precise positioning of biological materials, biochemicals and living cells…to fabricate 3D structures” (Murphy & Atala, 2014); and many other authors back this up, such as Starly & Shirwaiker (2015, p.58), mentioning that it is the “automated deposition of biological molecules” and Bishop, et al (2017, p.186), describing it as “the precise layering of cells, biological scaffolds and biologic factors”. The complex 3D structures created can be either scaffolds, cell/biomaterial composites, homogeneous tissue and several tissue contained organs (Wang, et al., 2016) (Figure 1). When searching for literature for this review, it was discovered that the term ‘tissue engineering’ appeared frequently. This term is used to describe the process of combining engineering and life sciences to understand the relationship between structure and function, and development of biological replacements (O’Brien, 2011). Bioprinting is a form of tissue engineering.
Figure 1
 The main steps to this unique science involve: imaging of the craniofacial defect (such as MRI or CT); then using CAD software to transform the scan into cross-sectional layers of the correct scale. Then additive manufacturing methods are used for printing biological material (Bishop, et al., 2017) (Figure 2). Bioprinting usually involves two approaches; direct and indirect. Direct printing consists of enclosing cells inside materials, which are then used as bioinks to be 3D printed (Gu, et al., 2015). Note that cells and biomaterials (for scaffolds) are printed simultaneously. Indirect printing, a more traditional approach to tissue engineering, involves printing a 3D scaffold, then seeding the cells inside these for them to culturize/regenerate. The scaffold degrades over time, leaving the printed tissue in place (Wang, et al., 2016). There is an additional processing stage after the bioprinting procedure, which involves a bioreactor. This tool offers a dynamic environment for cell-scaffold structures and facilitates its maturation.
The main steps to this unique science involve: imaging of the craniofacial defect (such as MRI or CT); then using CAD software to transform the scan into cross-sectional layers of the correct scale. Then additive manufacturing methods are used for printing biological material (Bishop, et al., 2017) (Figure 2). Bioprinting usually involves two approaches; direct and indirect. Direct printing consists of enclosing cells inside materials, which are then used as bioinks to be 3D printed (Gu, et al., 2015). Note that cells and biomaterials (for scaffolds) are printed simultaneously. Indirect printing, a more traditional approach to tissue engineering, involves printing a 3D scaffold, then seeding the cells inside these for them to culturize/regenerate. The scaffold degrades over time, leaving the printed tissue in place (Wang, et al., 2016). There is an additional processing stage after the bioprinting procedure, which involves a bioreactor. This tool offers a dynamic environment for cell-scaffold structures and facilitates its maturation.
Figure 2
Bioprinting for maxillofacial repair will be extremely beneficial when fully developed, as precise tissues/bone can be designed and manufactured specific to each patient on demand, improving both functionality, adapting time and aesthetics after surgery (Datta, et al., 2017).
3.2 Bioprinting Methods
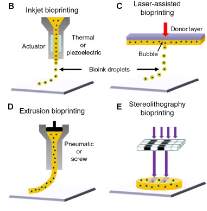 3D printing or ‘rapid prototyping’ is a growth industry expected to be worth £6.3 billion, and 26% of this is expected to be spent in medical applications (Krajekian, 2016). The 3D bioprinting industry was estimated to be worth. The global 3D bioprinting market was estimated to be £343 million in 2014, and this is predicted to rise to £1.28 billion by 2022 (Jessop, et al., 2017). Conventional 3D printing methods can be applied to bioprinting to produce the complex structures in the craniofacial region. The main advantage of using 3D printing technologies is their capability to produce large and complicated tissues rapidly with the internal and external structures being adaptable (Nyberg, et al., 2017). When searching for literature relating to the various bioprinting methods, there was a heavy number of useful and relevant articles, describing and comparing the methods, showing that knowledge of available routes is well known and they are sufficiently developed. Several articles highlight Inkjet based, laser assisted, microextrusion and stereolithography as the main techniques and they each have their own strengths, weaknesses and limitations. Brief concepts of the processes are shown in Figure 3.
3D printing or ‘rapid prototyping’ is a growth industry expected to be worth £6.3 billion, and 26% of this is expected to be spent in medical applications (Krajekian, 2016). The 3D bioprinting industry was estimated to be worth. The global 3D bioprinting market was estimated to be £343 million in 2014, and this is predicted to rise to £1.28 billion by 2022 (Jessop, et al., 2017). Conventional 3D printing methods can be applied to bioprinting to produce the complex structures in the craniofacial region. The main advantage of using 3D printing technologies is their capability to produce large and complicated tissues rapidly with the internal and external structures being adaptable (Nyberg, et al., 2017). When searching for literature relating to the various bioprinting methods, there was a heavy number of useful and relevant articles, describing and comparing the methods, showing that knowledge of available routes is well known and they are sufficiently developed. Several articles highlight Inkjet based, laser assisted, microextrusion and stereolithography as the main techniques and they each have their own strengths, weaknesses and limitations. Brief concepts of the processes are shown in Figure 3.
Figure 3
3.2.1 Inkjet Based
Both Dababneh & Ozbolat (2014) and Mandrycky, et al (2016) agree that bioprinting’s roots lie within inkjet printers, beginning use in the year. This is a non-contact process consisting of that deposits precise droplets of bioink under the control of a computer, to build up layer by layer the 3D structure. This method can then be further categorised into thermal or piezoelectric, depending on actuation mechanism (Boland, et al., 2006). It is the most common application and is the cheapest of them, as well as it being the most developed, due to the technology being introduced earliest. Now, inkjet printers are custom-designed to deal with printing at increasing resolution, precision and speed (Xu, et al., 2007). In addition to this, there is a cell viability of >85% for this process (Bishop, et al., 2017). However, a certain level of viscosity of bioink is needed, if not, the nozzle will potentially get clogged, which makes the deposition and precision more difficult to achieve (Kim, et al., 2010). In relation to printing the complex maxillofacial components, inkjet based printing is a very viable option, due to the high resolution and precision, as well as its ability to deposit biomaterials used for bone (Zhang & Zhang, 2015).
3.2.2 Laser Assisted
Laser assisted bioprinting is again a non-contact process, but nozzle free, which directs laser pulses through a ‘ribbon’ containing the bioink. The biological material is suspended on the bottom of the ribbon and when hit by the laser, vaporizes and creates a high-pressure bubble, which propels droplets to the substrate beyond the ribbon (Schiele, et al., 2010). This process is then repeated to build the structure layer by layer. An advantage of this method is the fact that there is no nozzle, therefore no clogging potential and ultimately the possibility of using a wider range of bioinks. Furthermore, there is a high degree of precision and resolution with this method, as well as a cell viability of >95%. However, there is a very high cost and time-consuming aspect associated (Nahmias et al.,2005); Kim, et al.,2010), yet when printing shapes as complex and important as craniofacial components, this weakness is not necessarily as important. Laser assisted techniques have been proven to print cells without damaging DNA or influencing the function (Gruene, et al., 2011), which is essential for maxillofacial application, due to the compound and dynamic behaviour of the different tissue in the face.
3.2.3 Microextrusion
The extrusion method of bioprinting consists of using either an air-force pump or a mechanical screw plunger to deposit bioinks. A continuous force is applied, which means that uninterrupted cylinders can be printed instead of single droplets (Saif & Sun, 2007). Post printing, the resulting structures can be solidified layer by layer either physically or chemically. This causes this method to be slower than others (Smith, et al., 2004). Cell viability can be as low as 40%, due to the high mechanical stresses the cells are exposed to. In addition, extrusion produces moderate resolution, which is not ideal for the complex structures in the craniofacial region (Mandrycky, et al., 2016). Extrusion based bioprinting is versatile, affordable and able to print porous structures, so it is utilised by many researchers worldwide (Ozbolat & Hospodiuk, 2015). Further advantages of this method include the moderate cost and possibility of using a wide range of materials (Yan, et al., 2005), however, this would not be a suitable technique for maxillofacial repair.
3.2.4 Stereolithography
The stereolithography (SLA) process is a nozzle-free technology that utilises photopolymerization. UV light is directed in a pattern, which cross links the bioink (that includes biocompatible polymer substances) to form a hardened layer. Each layer is solidified and the structure is built up as the substrate/platform is lowered (Guvendiren, et al., 2016). The continuing advancements in biocompatibility and biodegradation of encapsulated cells during processing makes this process a very promising future technology of bioprinting (Melchels, et al., 2009). Other strengths of this method is the low cost, high cell viability (>85%) and the high resolution of structures. There is a lengthy post-processing time associated with SLA, as well as a limit to the materials that are compatible for use. The main drawback of using SLA for medical purposes is the need for intense UV radiation for the layers to solidify (Guvendiren, et al., 2016).
3.3 Biomaterials
Similar to bioprinting techniques, the literature for this topic was of plenty, therefore a lot of information could be gathered. Some reading, like Fahmy, et al (2016) go into depth and only focus on available biomaterials, stating their advantages and disadvantages, whereas others, such as Gajendiran, et al (2017) and Li, et al (2016) give the requirements and brief descriptions of available materials, mainly because these articles focus on other aspects of bioprinting as well.
In relation to the maxillofacial region, biomaterials inks need to maintain their mechanical properties after printing. These attributes include strain, shear stress and compressive strength (Limpanuphap & Derby, 2002), and are essential for the tissue in the face, especially bone, in which scaffold-based approaches are preferred, as they allow for more favourable properties (Hospodiuk, et al., 2017). Furthermore, bioinks need to be ‘in sync’ with the human body (biocompatible). This parameter is usually the first to consider when fabricating scaffolds and will limit the number of suitable useable materials. The scaffold material must accommodate cells and the patient’s body, which requires support of cell growth, attachment and migration (Li, et al., 2016). Another requirement of biomaterials is appropriate porosity and interconnectivity. Cell behaviour is directly affected by pore size, shape and volume after being adhered to the scaffold material (Matsiko, et al., 2015). Open and interconnected pores allow delivery of oxygen and nutrients into the cells.
A wide range of biooinks have been developed for 3D bioprinting, which categorize into bioceramics, biopolymers (including hydrogels) and composites (Fahmy, et al., 2016); Each of these having their strengths, weaknesses and particular applications.
Firstly, bioceramics, such as Hydroxyapatite, Calcium Phosphate and Bioglass have the advantage of “upregulating osteogenesis” which means that it can facilitate cells that respond to this condition known as ‘brittle bone disease’. In addition, this material allows for space maintenance, which makes them interesting for reconstruction for maxillofacial defects (Kim, et al., 2010, p.523). Bioceramics also allow for proliferation of cells on the scaffold surface; however, the material is much too brittle to be used in craniofacial sites in a load bearing location (for example the temporomandibular joint) (Obregon, et al., 2015).
Hydrogels are agreed by both Gajendiran et al (2017) and Mandrycky et al (2016) to be the most common and useful form of bioink, due to their direct contact with cells for structural support, ease of fabrication, biodegradability and dominance of physical properties. Hydrogels contain biopolymers, either natural or synthetic (Zorlutuna, et al., 2013; Adepu, et al., 2017); natural polymers are preferred, due to their cell affinity, yet they are prone to unpredictable degradation and poor mechanical stability. Synthetic polymers are more controllable; therefore, they are mechanically better and provide better control over elastic modulus and specific cell stiffness (Zhang, et al., 2016). Other biopolymers include alginate, biogenic polyphosphate and biogenic silica, yet no sole polymer can satisfy all the needs required for bone replacement, which is a vital part of maxillofacial repair (Fahmy, et al., 2016)
Polymer/ceramic composites possess the correct properties needed to regenerate hard tissue like bone. They combine the good wear resistance of ceramics and toughness of polymers (Inzana, et al., 2014). Vorndran, et al (2010) highlights that low temperature 3D printing is capable of building polymer/mineral composites with highly beneficial properties related to growth factor and drugs, which will enhance bone regeneration or potentially fight infection.
When combined with the methods highlighted earlier, there are only certain biomaterials that can be printed through a certain bioprinter. This is down to the properties of the bioinks, such as viscosity, surface tension, adhesion, etc. (Table 1). There was a limited number of articles that compared biomaterials to appropriate methods, something that only Hospodiuk, et al (2017) managed from my literature search.
| Table 1 | |||
| Parameter | Dropwise or Inkjet | Laser assisted | Extrusion |
| Viscosity | Low (<100 mPa-s) | Medium (1–300 mPa-s) | Higher (>6–108 mPa-s) |
| Surface Tension | Medium | Low | Low |
| Fabrication speed | medium | low | high |
| Adhesion | Low | Adhesion within layers | Low |
3.4 Scaffolds
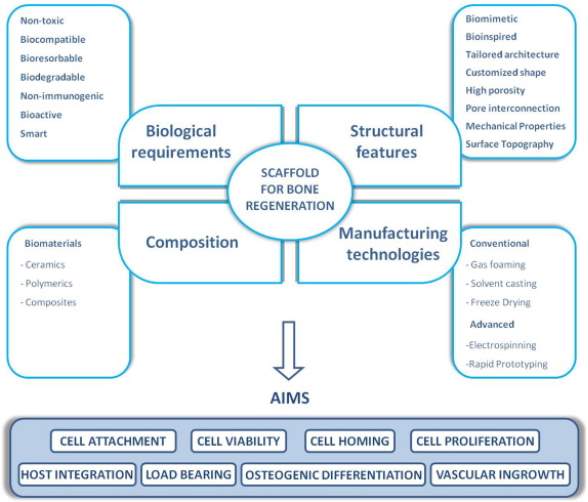 Gajendiran, et al (2017) describes scaffolds as templates for tissue formation and Roseti, et al (2017) describes them as vehicles for cells. All related literature obtained, agrees that scaffolds should have strict properties, no matter what the regenerated tissue. Gajendiran, et al (2017) in particular, describes scaffold requirements in a simple and easy to understand format, as well as go into depth about each topic. In addition, it gives a detailed diagram about what is needed for a successful scaffold (Figure 4). Scaffolds should be biocompatible, which is to allow or improve cell homing, viability, attachment and proliferation (Amini, et al., 2012). If cells are not able to grow and culturize inside the scaffold, then it simply will not replicate the tissue that was previously damaged. Biodegradability is another attribute scaffolds must possess, as the whole concept of tissue engineering is for the cells, over time, to replace the implanted scaffold, as they are not intended to be permanent implants. Mechanical properties of scaffolds should be consistent for the application intended, e.g. muscle, bone, etc, as well as be strong enough for surgeons to handle on implantations. Architecture is also an important aspect; scaffolds should have an interconnected pore system and high porosity, which will ensure cell penetration and diffusion of nutrients towards cells and diffusion of waste away from the cells.
Gajendiran, et al (2017) describes scaffolds as templates for tissue formation and Roseti, et al (2017) describes them as vehicles for cells. All related literature obtained, agrees that scaffolds should have strict properties, no matter what the regenerated tissue. Gajendiran, et al (2017) in particular, describes scaffold requirements in a simple and easy to understand format, as well as go into depth about each topic. In addition, it gives a detailed diagram about what is needed for a successful scaffold (Figure 4). Scaffolds should be biocompatible, which is to allow or improve cell homing, viability, attachment and proliferation (Amini, et al., 2012). If cells are not able to grow and culturize inside the scaffold, then it simply will not replicate the tissue that was previously damaged. Biodegradability is another attribute scaffolds must possess, as the whole concept of tissue engineering is for the cells, over time, to replace the implanted scaffold, as they are not intended to be permanent implants. Mechanical properties of scaffolds should be consistent for the application intended, e.g. muscle, bone, etc, as well as be strong enough for surgeons to handle on implantations. Architecture is also an important aspect; scaffolds should have an interconnected pore system and high porosity, which will ensure cell penetration and diffusion of nutrients towards cells and diffusion of waste away from the cells.
Figure 4
In relation to maxillofacial defects, scaffold will need to exhibit good structural and mechanical properties to resist contractive forces. There are different types of scaffolds used for craniofacial bioprinting (Figure 5). These properties will guarantee a suitable environment for cell/tissue growth. Due to the diversity of tissues in the face, site-specific scaffolds are necessary to mimic the housing tissue.
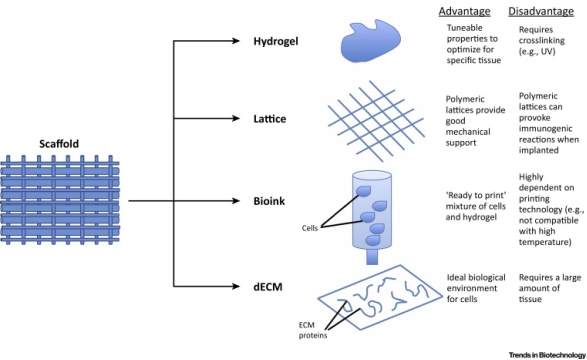 Scaffold-free modalities have certain advantages over scaffold-based modalities, however for they are unsuitable for certain types of maxillofacial tissues, like load-bearing bone (Visscher, et al., 2016). Visscher, et al (2016) was another very useful article for this topic in this literature review as it related to maxillofacial defects, whereas other articles, such as Roseti et al (2017), takes a more general approach, and do not target specific areas of the body.
Scaffold-free modalities have certain advantages over scaffold-based modalities, however for they are unsuitable for certain types of maxillofacial tissues, like load-bearing bone (Visscher, et al., 2016). Visscher, et al (2016) was another very useful article for this topic in this literature review as it related to maxillofacial defects, whereas other articles, such as Roseti et al (2017), takes a more general approach, and do not target specific areas of the body.
Figure 5
4.0 Challenges
Despite the significant progress in the development of bioprinting over the last two decades, it is still a relatively new process and there are challenges/limitations that are preventing it progressing into the clinical/commercial stage (Mandrycky, et al., 2016). There are a range of factors that need to be considered if it is going to progress, including biological, technological, regulatory and ethical (Jessop, et al., 2017). Jessop, et al (2017) gives a good overview of the range of challenges that researchers face, however, most articles, like Dababneh & Ozbolat (2014) and Al-Nawas & Goetze (2017) only focus on a single topic (biological and regulatory respectively). In addition to the existing challenges, application to maxillofacial areas will make further break throughs even more difficult, due to the function and complexity of the components. However, considering the speed at which technology is advancing in the modern world, there is confidence that bioprinting will become a commercial method for maxillofacial repair in the near future (Donderwinkel, et al., 2017).
4.1 Biological
The vital post-processing step of the 3D bioprinted construct becoming a piece of functional tissue is the main limitation of successful clinical translation. In vitro (bioreactor) or in vivo methods are still being developed and effects/the best route to take has no yet been determined (Mironov, et al., 2009). Another biological factor is the lack of vasculature, instead relying on porous scaffolds. Evidence has proven that pores promote blood vessel growth, however this process is much too slow to allow any important increase in tissue construct size and complexity (Cui & Boland, 2009). Other challenges of printing complex tissue include reducing cell viability from excessive biomanufacturer time, loss of regenerative potential and acidic by-products being released from degradation (Jessop, et al., 2017). Material selection is another limitation to bioprinting. Often most biomaterials lack the relevant properties needed for a particular tissue. The solution is to use composites, however incorporating more than one material requires secondary processing steps for the material, which increases cost, time and difficulty (Mandrycky, et al., 2016).
4.2 Technological
The main technological challenges faced by bioprinting is the actual bioprinters themselves. The techniques described earlier in this review are layer by layer methods, which have problems printing hollow, complex constructs. Voids are likely to appear if constructs are not supported, which cause offset features and incorrect geometry (Taylor, et al., 2013). A solution to this would be to incorporate a sacrificial material for support, but this requires extra material to be printed at the same time, which as Mandrycky et al (2016) described increases the complexity of the whole process as well as the time taken. Ensuring that printed constructs, especially in the maxillofacial area, have high resolution is another challenge faced by researchers. Stereolithography and inkjet based bioprinters currently offer the best resolutions available, however these methods are limited by lack of suitable biomaterials (He, et al., 2016). Both Jessop, et al (2017) and Mandrycky, et al (2016) agree that the combinations of the correct materials and methods pose the biggest challenge of bioprinting.
4.3 Regulatory
There were limited papers describing the regulations when regarding bioprinting. Li & Faulkner (2017) describes current regulations and is up to date and singles out that considerations involve the patient’s health and safety as a difference from conventional 3D printing. The sources of biomaterials are a concern, because the cells initially need to be obtained from the subject’s body, as they easily adapt to host tissues. Rejection rate of the patient reduces when using autogenic cells, however using allogenic cells for fabrication is also an option (Hourd, et al., 2015). In both cases, the activity of gathering these cells must meet standards of the Guide to Quality and Safety Assurance of Human Tissues and Cells for Patient Treatments (HTA, 2016). The Human Tissue Act 2004 also states that the transplantable material can only be removed by a licensed person and removal would have to be non-commercial. The manufacturing methods must also comply with current Good Manufacturing Practice (GDP) regulations and obtain approval from The Food and Drug Administration (FDA). Bioprinted structures containing cells require proper clinical trials and testing before approval for routine practice (Wolinsky, 2014). In addition to sourcing the biomaterials, there are regulations regarding the computer aided design from medical scans. Factors involve consumer safety, protection of data, confidentiality and product liability (Hourd, et al., 2015). Overall, the main regulatory challenge will be to continuously monitor, standardise and validate bioprinting manufacture from design all the way to actual production, which poses immense difficulty (Lee, et al., 2010).
4.4 Ethical
Again, there is limited literature about ethical issues shadowing bioprinting, and again Li & Faulkner (2017) was the most useful article as it relates the regulations/standards to ethical considerations associated with them. In terms of cells to be obtained, a fully informed consent procedure is needed to minimise the risk of violating ethics. Donors of cells/tissues should be informed about the use and purpose of the process (Varkey & Atala, 2015). The preparation of biomaterials can also be a concern with society and religion, in relation to human dignity and humanity, if stem cells are used as bioinks (Li & Faulkner, 2017).
5.0 Clinical Application
Visscher, et al (2016) was a very useful piece of literature as it gives an overview of the potential of clinical application of bioprinting, as well as it being relatable to the maxillofacial region. Al-Nawas & Goetze (2017) also highlights clinical application, however gives case studies that do not particularly relate to maxillofacial surgery, even though mentioned in the title of the article. There has been some evidence of 3D printing being used in maxillofacial repair, such as James Watson using his son’s scan (using a 3D camera) to 3D print the missing gaps removed to dispose of a cancerous tumour (NUH News, 2015). Biomaterials were not used, however the process of using family resemblance to rebuild body features was a breakthrough at the time and shows that new routes/strategies are still being introduced, which ultimately proves that research and development is improving in medicine. Bioprinting clinical applications are at quite an early stage and further development is still needed. Nevertheless, promising preclinical and animal trials have been performed, for example the treatment of 13 subjects involving implanting scaffolds at four different parts within the craniofacial region (Sandor, et al., 2014). Arslan-Yildriz et al (2016) gives a current biomedical application overview of different types of tissue regeneration including bone and skin, which are useful when considering maxillofacial repair.
6.0 Conclusions and the Future
In this literature review, the bioprinting for maxillofacial repair topic has been described and sources have been compared and analysed. Notable readings include Jessop et al (2017), Mandrycky et al (2016) and (Mitchell, 2017), as these all give an in-depth overview of every aspect of bioprinting. In addition, Datta, et al (2017) and Nyberg et al (2017) relate bioprinting to maxillofacial/craniofacial regeneration, which was convenient when attempting to make connections in this review. These papers mentioned have also been published within the past 5 years, so is state of the art information. Due to bioprinting being a recent technology there were limited books on the subject, so articles were the main source of information for this review.
In terms of the future of bioprinting, it is still in the early stages of development and is far away from commercial applications Visscher et al (2016). This is a combination of biomaterial, technology, scaffold limitations as well as the advanced requirements of the tissue that needs to be repaired/regenerated. Maxillofacial defects are adding to the barriers between bioprinting and commercial use. The complexity of tissue in and around the face, the additional needs of these tissues (e.g. load bearing) and finding a suitable bioink material to effectively retain these properties all pose difficulty Nyberg et al (2017). However, with the increasing speed of development into bioprinting; successful and effective bioprinting could be applied clinically/commercially in the near future.
7.0 Acknowledgements
This literature review is the work of Jack Wilson, a student of the University of Nottingham at time of writing (2018). The work was completed under the supervision of Dr Joel Segal in alignment with a module led by Dr Richard Cobb, within the faculty of engineering. Credit to both for their support.
8.0 References
Adepu, S. et al., 2017. Three-dimensional bioprinting for bone tissue regeneration. Current Opinion in Biomedical Engineering, Volume 2, pp. 22-28.
Al-Nawas, B. & Goetze, E., 2017. 3-D pressure in the maxillofacial surgery. The maxillofacial surgeon, 10(4), pp. 234-243.
Amini, A., Laurencin, C. & Nukavarapu, S., 2012. Bone Tissue Engineering: Recent Advances and Challenges. Critical Reviews in Biomedical Engineering, 40(5), pp. 363-408.
An, J., Joanne Ee Mei Teoh, Suntornnond, R. & Chua, C. K., 2015. Design and 3D Printing of Scaffolds and Tissues. Engineering, 1(2), pp. 261-268.
Arslan-Yildriz, A. et al., 2016. Towards artificial tissue models: past, present, and future of 3D bioprinting. Biofabrication, 8(1).
Bishop, E. et al., 2017. 3-D bioprinting technologies in tissue engineering and regenerative medicine: Current and future trends. Genes and Diseases, 4(4), pp. 185-195.
Boland, T., Xu, T., Damon, B. & Cui, X., 2006. Application of inkjet printing to tissue engineering. Biotechnology, Volume 1, pp. 910-917.
Bostrom, R. & Mikos, A., 2002. Tissue engineering of bone. Bioengineering of bone regeneration, 18(10), pp. 995-1002.
Cui, X. & Boland, T., 2009. Human microvasculature fabrication using thermal inkjet printing technology. Biomaterials, 30(31), pp. 6221-6227.
Dababneh, A. B. & Ozbolat, I. T., 2014. Bioprinting Technology: A Current State-of-the-Art Review. Journal of Manufacturing Science and Engineering, 136(6).
Datta, P. et al., 2017. Bone tissue bioprinting for craniofacial reconstruction. Biotechnology and Bioengineering, 114(11), pp. 2424-2431.
DCI Donor Services Tissue Bank, 2017. Allograft vs. Autograft. [Online]
Available at: http://tissuebank.dcids.org/who-we-serve/patient-education/allograft-vs-autograft/
[Accessed 28 January 2018].
Donderwinkel, I., van Hest, J. C., Cameron & R, N., 2017. Bio-inks for 3D bioprinting: recent advances and future prospects. Polymer Chemistry, 8(31), pp. 4451-4471.
Fahmy, M. D., Jazayeri, H. E., Razavi, M. & Masri, R., 2016. Three-Dimensional Bioprinting Materials with Potential Application in Preprosthetic Surgery. Journal of Prosthodontics, 25(4), pp. 310-318.
Fong, K. et al., 2003. New Strategies for Craniofacila Repair and Replacement: A Brief Review. Journal of Craniofacial Surgery, 14(3), pp. 333-339.
Gajendiran, M. et al., 2017. Conductive biomaterials for tissue engineering applications. Journal of Industrial and Engineering Chemistry, 51(1), pp. 12-26.
Gassner, R. et al., 2003. Cranio-maxillofacial trauma: a 10 year review of 9543 cases with 21067 injuries. Journal of Cranio-Maxillofacial Surgery, 31(1), pp. 51-61.
Goldberg, V. M., Victor, M. & Sharon, D., 1987. Natural history of autografts and allografts. Clinical Orthopaedics and Related Research, Volume 225, pp. 7-16.
Gruene, M. et al., 2011. Laser Printing of Three-Dimensional Multicellular Arrays for Studies of Cell-Cell and Cell-Environment Interactions. Tissue Engineering Part C: Methods, 17(10), pp. 973-982.
Gu, Q. et al., 2015. Three-dimensional bio-printing. Science China Life Sciences, 58(5), pp. 411-419.
Guvendiren, M., Molde, J., Soares, R. & Kohn, J., 2016. Designing Biomaterials for 3D Printing. Acs Biomaterials Science and Engineering, 2(10), pp. 1679-1693.
He, Y. et al., 2016. Research on the printability of hydrogels in 3D bioprinting. Scientific Reports, p. 29977.
Hospodiuk, M., Dey, M., Sosnoski, D. & Ozbolat, I., 2017. The bioink: A comprehensive review on bioprintable materials. Biotechnology Advances, 35(2), pp. 217-239.
Hourd, P., Medcalf, N., Segal, J. & Williams, D., 2015. A 3D bioprinting exemplar of the consequences of the regulatory requirements on customized processes. Regenerative Medicine, 10(7), pp. 863-883.
HTA, 2016. Human Tissue Act 2004. [Online]
Available at: https://www.hta.gov.uk/policies/human-tissue-act-2004
[Accessed 31 January 2018].
Inzana, J. et al., 2014. 3D printing of composite calcium phosphate and collagen scaffolds for bone regeneration. Biomaterials, 35(13), pp. 4026-4034.
Jessop, Z. et al., 2017. 3D bioprinting for reconstructive surgery: Principles, applications and challenges. Journal of Plastic, Reconstructive and Aesthetic Surgery, 70(9), pp. 1155-1170.
Kim, J. et al., 2010. Piezoelectric inkjet printing of polymers: Stem cell patterning on polymer substrates. Polymer, 51(10), pp. 2147-2154.
Kim, K., Yeatts, A., Dean, D. & Fisher, J., 2010. Stereolithographic bone scaffold design parameters: osteogenic differentiation and signal expression. Tissue Engineering Part B, 16(5), pp. 523-539.
Krajekian, J., 2016. 3D Printing Role in Oral and Maxillofacial Surgery: Current and Future Trends. Advances in Dentistry and Oral Health, 2(3).
Lee, M. et al., 2010. Considerations for tissue-engineered and regenertive medicine product development prior to clinical trials in the United States. Tissue Engineering Part B, 16(1), pp. 41-54.
Li, J., Chen, M., Fan, X. & Zhou, H., 2016. Recent advances in bioprinting techniques: approaches, applications and future prospects. Journal of Transational Medicine, Volume 14, p. 271.
Limpanuphap, S. & Derby, B., 2002. Manufacture of biomaterials by a novel printing process. Journal of Materials Science: Materials in Medicine , 13(12), pp. 1163-1166.
Li, P. & Faulkner, A., 2017. 3D Bioprinting Regulations: a UK/EU Perspective. European Journal of Risk Regulation, 8(2), pp. 441-447.
Mandrycky, C., Wang, Z., Kim, K. & Kim, D., 2016. 3D bioprinting for engineering complex tissues. Biotechnology Advances, 34(4), pp. 422-434.
Matsiko, A., Gleeson, J. & O’Brien, F., 2015. Scaffold mean pore size influences mesenchymal stem cell chondrogenic differentiation and matrix deposition. Tissue Engineering-Part A, 21(3-4), pp. 486-497.
Melchels, F., Feijen, J. & Grijpma, D., 2009. A poly(d,l-lactide) resin for the preparation of tissue engineering scaffolds by stereolithography. Biomaterials, 30(23), pp. 3801-3809.
Mironov, V. et al., 2003. Organ printing: computer-aided jet-based 3D tissue engineering. Trends in Biotechnology, 21(4), pp. 157-161.
Mironov, V. et al., 2009. Organ printing: Tissue spheroids as building blocks. Biomaterials, 30(12), pp. 2164-2174.
Mitchell, M. G., 2017. Bioprinting: Techniques and Risks for Regenerative Medicine. s.l.:Elsevier Science and Technology Books.
Murphy, S. V. & Atala, A., 2014. 3D bioprinting of tissues and organs. Nature Biotechnology, 32(1), pp. 773-785.
Nahmias, Y., Schwartz, R., Verfaillie, C. & Odde, D., 2005. Laser-guided direct writing for three-dimensional tissue engineering. Biotechnology and Bioengineering, 92(2), pp. 129-136.
NUH News, 2015. Facing the Future. NUH News, April, p. 1 & 6.
Nyberg, E. et al., 2017. 3D-Printing Technologies for Craniofcial Rehabilitation, Reconstruction, and Regeneration. Annals of Biomedical Engineering, 45(1), pp. 45-57.
Obregon, F. et al., 2015. Three-Dimensional Bioprinting for Regenerative Dentistry and Craniofacial Tissue Engineering. Journal of Dental Research, 94(9), pp. 143-152.
O’Brien, F. J., 2011. Biomaterials and scaffolds for tissue engineering. materialstoday, 14(3), pp. 88-95.
Ozbolat, I. & Hospodiuk, M., 2015. Current advances and future perspectives in extrusion-based bioprinting. Biomaterials, 76(1), pp. 321-343.
Pagni, G. et al., 2012. Bone repair cells for craniofacial regeneration. Advanced Drug Delivery Reviews, 64(12), pp. 1310-1319.
Posnick, J. & Sami, A., 2015. Use of Allogenic (lliac) Corticocancellous Graft for Le Fort I Interpositional Defects: Technique and Results. Journal of Oral and Maxillofacial Surgery, 73(1), p. 168.
Radabaugh, J., Zhang, P. & Wang, D., 2016. Barriers to Repair in Maxillofacial Trauma. JAMA Facial Plastic Surgery, 18(3), pp. 177-182.
Roseti, L. et al., 2017. Scaffolds for Bone Tissue Engineering: State of the art and new perspectives. Materials Science and Engineering: C, 78(1), pp. 1246-1262.
Saif, K. & Sun, W., 2007. Biopolymer deposition for freeform fabrication of hydrogel tissue constructs. Materials Science and Engineering C, 27(3), pp. 469-478.
Salentijn, E. et al., 2014. A ten-year analysis of the traumatic maxillofacial and brain injury patient in Amsterdam: Incidence and aetiology. Journal of Cranio-Maxillofacial Surgery, 42(6), pp. 705-710.
Sandor, G. et al., 2014. Adipose stem cells used to reconstruct 13 cases with cranio-maxillofacial hard-tissue defects. Stem Cells Translational Medicine, 3(4), pp. 530-540.
Schiele, N. et al., 2010. Laser-based direct-write techniques for cell printing. Biofabrication, 2(3).
Seliktar, D., Dikovsky, D. & Napadensky, E., 2013. Bioprinting and Tissue Engineering: Recent Advances and Future Perspectives. Israel Journal of Chemistry, 53(9-10), pp. 795-804.
Smith, C. et al., 2004. Three-Dimensional BioAssembly Tool for Generating Viable Tissue-Engineered Constructs. Tissue Engineering, 10(9-10), pp. 1566-1576.
Starly, B. & Shirwaiker, R., 2015. 3D Bioprinting Techniques. In: 3D Bioprinting and Nanotechnology in Tissue Engineering and Regenerative Medicine. s.l.:Elsevier, pp. 57-77.
Surgeons: At The Edge Of Life. 2018. BBC 2. 8 January, 20:00
Taylor, R. et al., 2013. Sacrificial layer technique for axial force post assay of immature cardiomyocytes. Biomedical Microdevices, 15(1), pp. 171-181.
Varkey, M. & Atala, A., 2015. Organ Bioprinting: A Closer Look at Ethics and Policies. Research Gate, p. 275.
Visscher, D. O., Farre-Guasch, E., Helder, M. N. & Gibbs, S., 2016. Advances in Bioprinting Technologies for Craniofacial Reconstruction. Trends in Biotechnology, 34(9), pp. 700-710.
Vorndran, E. et al., 2010. Simultaneous Immobilization of Bioactives During 3D Powder Printing of Bioceramic Drug-Release Matrices. Advanced Functional Materials, 20(10), pp. 1585-1591.
Wang, X. et al., 2016. 3D Bioprinting Technologies for Hard Tissue and Organ Engineering. Materials, 9(10), p. 802.
Wolinsky, H., 2014. Printing organs cell-by-cell: 3-D printing is growing in popularity, but how should we regulate the application of this new technology to health care?. EMBO Reports, 15(8), pp. 836-838.
Xu, T., H, Kincaid & Yoo, A. A. J., 2007. High-Throughput Production of Single-Cell Microparticles Using an Inkjet Printing Technology. Journal of Manufacturing Science and Engineering, 130(2).
Yan, Y. et al., 2005. Fabrication of viable tissue-engineered constructs with 3D cell-assembly technique. Biomaterials, 26(29), pp. 5864-5871.
Zhang, G. L., Fisher, J. P. & Leong, K., 2015. 3D Bioprinting and Nanotechnology in Tissue Engineering and Regenerative Medicine. XVIII ed. London: London: Academic Press.
Zhang, H. et al., 2016. Three-dimensional bioprinting is not only about cell-laden structures. Chinese Journal of Traumatology, 19(4), pp. 187-192.
Zhang, L. G., 2015. 3D Bioprinting and Nanotechnology in Tissue Engineering and Regenerative Medicine. In: J. P. Fisher & K. W. Leong, eds. 3D Bioprinting Techniques. s.l.:Elsevier, pp. 57-77.
Zhang, X. & Zhang, Y., 2015. Tissue Engineering Applications of Three-Dimensional Bioprinting. Cell Bichemistry and Biophysics, 72(3), pp. 777-782.
Zorlutuna, P., Vrana, N. & Khademhosseini, A., 2013. The expanding world of tissue engineering: the building blocks and new applications of tissue engineered constructs. IEEE Reviews in Biomedical Engineering, Volume 6, pp. 47-62.
Cite This Work
To export a reference to this article please select a referencing stye below:
Related Services
View all


Related Content
All TagsContent relating to: "Medical Technology"
Medical Technology is used to enhance the medical care and treatment that patients are given in healthcare settings. Medical Technology can be used to identify, diagnose and treat medical conditions and illnesses.
Related Articles

DMCA / Removal Request
If you are the original writer of this dissertation and no longer wish to have your work published on the UKDiss.com website then please: